

Abstract
Dyspepsia with mild, stabbing epigastric discomfort without history of trauma is a very common symptom that emergency physicians see in their daily practice. Vascular emergencies, mostly the aortic dissection and aneurysm, are always described in the differential diagnosis with persistent symptoms. Isolated celiac artery dissection occurring spontaneously is a very rare diagnosis. The involvement of branch vessels is generally observed and patients show various clinical signs and symptoms according to the involved branch vessel. Here we are presenting a case with spontaneous isolated celiac artery dissection, without any branch vessel involvement or visceral damage, detected by computed tomography scans taken on admission.
KEYWORDS: Celiac Artery, Dissection, Spontaneous, Isolated, Splanchnic Artery
Dyspepsia with mild, stabbing epigastric discomfort without history of trauma is a very common symptom that emergency physicians see in their daily practice. Vascular emergencies, mostly the aortic dissection and aneurysm, are always described in the differential diagnosis with persistent symptoms.1 The clinical course of aortic dissection is generally catastrophic even with modern surgical interventions. But, this situation may not be true for isolated splanchnic artery dissections especially for the celiac artery dissection (CAD).
Spontaneous dissection of a splanchnic artery, including the superior mesenteric artery (SMA), and inferior mesenteric artery (IMA), and the celiac artery, without aortic dissection is an uncommon occurrence. Among them, the isolated CAD is the least commonly reported one.2 Most previous publications about spontaneous isolated CAD are case reports. There are several management modalities applied by the physicians on a case by-case basis like endovascular repair or interventional radiological approach.3 But, conservative treatment options by anticoagulants and anti-platelets besides antihypertensives are also noted.4 Some of the reported cases showed progression with several serious events and some remained un-complicated.2
Here we are presenting a patient with spontaneous isolated CAD who was managed conservatively with only antihypertensive agents and remained symptom free after 10 months of follow-up.
Case Report
A 40 year-old male smoker was presented with low back pain and mild epigastric discomfort. He had been taking non-steroidal antiinflammatory drugs for his back pain for two days. The patient was complaining of stabbing epigastric pain. He came to the emergency room with 5 hours of epigastric discomfort early in the morning. He had dyspeptic symptoms with some certain foods for 2 years and had a heavy meal last night. Two hours before, he ingested two tablets of antacid and felt much better. The patient's medical history revealed hypertension for 5 years. He was using 2 different groups of antihypertensive drugs but he stopped taking them for 1 month.
At presentation, his blood pressure was 200/100 mmHg at both arms and he had a mild epigastric discomfort pathologically. The physical examination was otherwise normal. Initial blood tests including cardiac enzymes, complete blood count, renal function tests, liver enzymes, amylase, lipase, and d-dimer were in normal ranges. Serial ECG's were all normal sinus rhythm.
Intravenous proton pump inhibitor was started, and his blood pressure was lowered with short acting ACE inhibitor orally. After 1 hour he felt much better. But, the pain in the epigastric region did not resolve totally. So a contrast enhanced thoracic and abdominal computed tomography (CT) scan was performed to rule out vascular emergencies. There was no dissection or aneurysm at the thoracic and abdominal aorta but isolated celiac artery dissection was observed. There was normal flow at hepatic and renal arteries. Liver, spleen, bowel, and kidney perfusions were also normal (Figure 1). Cardiovascular surgery consultation was performed. The patient was managed with only antihypertensive drugs.
Figure 1.
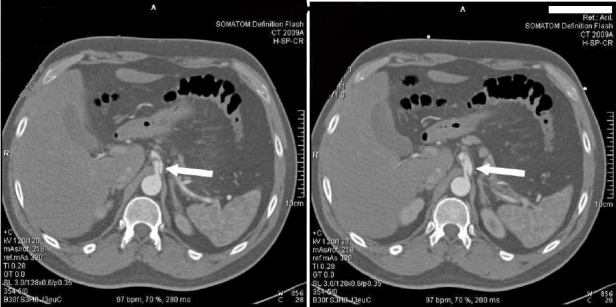
Upper abdominal contrast-enhanced CT scan revealed celiac artery dissection
Ten months later he was asymptomatic with good blood pressure control. Because he remained asymptomatic, he denied a radiological follow up.
Discussion
Dissection of an artery occurs with intimal layer disruption which allows blood to enter the media, and separates the intimal and adventitial layers. The dissecting column of blood forms a false lumen and may extend proximally, distally, or both. Classical presenting symptom is sharp, stabbing pain radiating to back in the chest and upper abdomen.1 Risk factors listed at previous reports include hypertension, cystic medial necrosis, abdominal aortic aneurysm, fibromuscular dysplasia, trauma, pregnancy, and connective tissue disorders. However, most of the patients in some series are generally healthy with no underlying disease. The definitive cause has not been well understood yet.5,6
For the diagnosis, conventional angiography, doppler ultrasonography, CT, and magnetic resonance imaging can be used. As in our case, contrast-enhanced CT is the advised technique because of its convenience, quickness, low invasiveness, and reliability.6,7 CT scan can provide high quality images of dissection site and also gives knowledge about the extension of the lesion, aneurysm formation, and intramural hematomas.
CAD without the involvement of aorta and the other splanchnic arteries is very rare. The SMA dissection alone and involvement of both SMA and CA were reported much frequently than isolated CAD. We have found 25 cases of isolated CAD except our presenting case, at PubMed (since 1966), with the key words of “celiac artery”, “dissection”, “spontaneous”, “splanchnic artery”. Nordanstig et al. summarized 24 of them. Two of the listed cases in Nordastig's report were postmortem diagnosis. Seventeen male and seven female patients were reported. The most common presenting symptom was abdominal pain. There were also asymptomatic patients. Eight patients were treated with invasive methods, while others were approached conservatively. Overall outcome was good in both types of treatment modalities. Complications included ischemia, aneurysm formation, and rupture.2 As far as we know; Wang et al. published the last case of spontaneous isolated CAD in the literature. The reported patient was a 44 year-old male presenting with chest and abdominal pain, and he was treated conservatively.8
The involvement of branch vessels is generally observed and patients showed various clinical signs and symptoms according to the involved branch vessel.9 Our patient demonstrated normal flow at hepatic and renal arteries in CT scan. Liver, spleen, bowel, and kidney perfusions were also normal. There was no aneurysmatic dilatation of the celiac artery. To our knowledge, there is only one spontaneous isolated CAD case reported previously except our patient, without any branch vessel involvement or visceral damage, detected by CT scans taken on admission.8
Traditional open surgery, endovascular surgery, and interventional radiological approach are invasive options of the splanchnic artery dissection treatment. Indications for surgery in SMA dissection include increasing the size of the aneurysm, intraluminal thrombosis, abnormal blood flow through the vessel, and the persistent symptoms despite antico-agulation.3 In case of CAD, Glehen et al. recommend surgical repair in the presence of complications like occlusive lesions, aneurysm formation, and arterial rupture, or extension of the CAD into hepatic arteries.10 The recommended conservative treatments include anticoagulants, anti-platelets, and antihypertensives.4 We followed up our patient only with antihypertensive regimen. Since there was normal flow at the visceral branches with intact organ perfusions, we did not use anticoagulants and anti-platelets.
Conclusion
In conclusion spontaneous CAD should be included in the differential diagnosis of refractory epigastric pain in the emergency room. It is a rare situation but may be underestimated in the past because of its probable benign nature. With continued improvement of the use of contrast enhanced CT scan in emergency room, the lesions may be diagnosed more commonly. We thought that uncomplicated cases with normal visceral perfusions can be managed only with strict control of blood pressure. But, for a definitive way of treatment large series of cases and prospective studies are needed.
Authors’ Contributions
TCO and SY followed-up the patient and searched the literature. OY, SEC and OG searhed the literature and contribute to discussion part. All authors have read and approved the content of the manuscript.
Footnotes
Conflict of Interests
Authors have no conflict of interests.
References
- 1.Tintinalli J, Stapczynski J, Stapczynski O, Cline D, Cydulka R, Meckler G. 7th ed. New York: McGraw-Hill Professional; 2011. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. [Google Scholar]
- 2.Nordanstig J, Gerdes H, Kocys E. Spontaneous isolated dissection of the celiac trunk with rupture of the proximal splenic artery: a case report. Eur J Vasc Endovasc Surg. 2009;37(2):194–7. doi: 10.1016/j.ejvs.2008.10.009. [DOI] [PubMed] [Google Scholar]
- 3.Sparks SR, Vasquez JC, Bergan JJ, Owens EL. Failure of nonoperative management of isolated superior mesenteric artery dissection. Ann Vasc Surg. 2000;14(2):105–9. doi: 10.1007/s100169910019. [DOI] [PubMed] [Google Scholar]
- 4.Fenoglio L, Allione A, Scalabrino E, Alberto G, Benedetti V, Pomero F, et al. Spontaneous dissection of the celiac artery: a pitfall in the diagnosis of acute abdominal pain.Presentation of two cases. Dig Dis Sci. 2004;49(7-8):1223–7. doi: 10.1023/b:ddas.0000037816.57229.6f. [DOI] [PubMed] [Google Scholar]
- 5.Kim JH, Roh BS, Lee YH, Choi SS, So BJ. Isolated spontaneous dissection of the superior mesenteric artery: percutaneous stent placement in two patients. Korean J Radiol. 2004;5(2):134–8. doi: 10.3348/kjr.2004.5.2.134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.D’Ambrosio N, Friedman B, Siegel D, Katz D, Newatia A, Hines J. Spontaneous isolated dissection of the celiac artery: CT findings in adults. AJR Am J Roentgenol. 2007;188(6):W506–11. doi: 10.2214/AJR.06.0315. [DOI] [PubMed] [Google Scholar]
- 7.Takayama T, Miyata T, Shirakawa M, Nagawa H. Isolated spontaneous dissection of the splanchnic arteries. J Vasc Surg. 2008;48(2):329–33. doi: 10.1016/j.jvs.2008.03.002. [DOI] [PubMed] [Google Scholar]
- 8.Wang JL, Hsieh MJ, Lee CH, Chen CC, Hsieh IC. Celiac artery dissection presenting with abdominal and chest pain. Am J Emerg Med. 2010;28(1):111–5. doi: 10.1016/j.ajem.2009.02.023. [DOI] [PubMed] [Google Scholar]
- 9.Oh S, Cho YP, Kim JH, Shin S, Kwon TW, Ko GY. Symptomatic spontaneous celiac artery dissection treated by conservative management: serial imaging findings. Abdom Imaging. 2011;36(1):79–82. doi: 10.1007/s00261-010-9657-x. [DOI] [PubMed] [Google Scholar]
- 10.Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM. Spontaneous dissection of the celiac artery. Ann Vasc Surg. 2001;15(6):687–92. doi: 10.1007/s10016-001-0012-0. [DOI] [PubMed] [Google Scholar]