

Abstract
BACKGROUND:
Primary health care system is the basic core of public service provision in Iran. This study aimed to assess clients’ satisfaction with primary health care in Tehran, the capital of Iran, as a metropolitan.
METHODS:
Through a cross-sectional study in 2009-10, four urban primary health care clinics were selected through stratified random sampling. Four hundred participants were interviewed in the selected clinics about their satisfaction with the primary health care services and setting. Six domains of satisfaction including accessibility to services, continuity of care, humaneness of staff, comprehensiveness of care, provision of health education and effectiveness of services were calculated from selected variables. The descriptive statistics, chi-square and t-tests were used when appropriate.
RESULTS:
The mean age of users of health services was 31.3 years (SD=9.6). Thirteen percent of participants were male. The most common reasons for asking health services reported as vaccination, family planning and children care. Overall, primary health care services were suitable for eighty percent of the participants. The mean and standard deviation for Access to services was 2.11 (SD=3.44), continuity of care was -0.35 (SD=3.49), humanness of staff was 3.93 (SD=5.70), comprehensiveness of care was -0.53 (SD=3.66), provision of health educational materials was -1.45 (SD=3.64) and effectiveness of services was 4.30 (SD=7.47).
CONCLUSIONS:
Primary health care is a comprehensive and suitable strategy to provide health services in public health. Package of services in primary health care may affect clients’ satisfaction. Using family doctors may improve the indices.
Keywords: Primary Health Care, Patient Satisfaction, Community Health Centers, Iran, Tehran
Iran is an ancient country with more than three thousands year's history of civilization. It's capital, Tehran, is one of the most populous metropolitans, holding a population of more than 13.5 million.1 The Ministry of Health of Iran has a unique structure that makes it different from ministries of health in most other countries; the Iranian parliament authorized the government to integrate medical education into the Ministry of Health in 1986 and established a new Ministry, named Ministry of Health and Medical Education. This Ministry is responsible for both population health and training health workforces. There are more than 40 medical universities distributed in 31 provinces of Iran. The chan cellor of each medical university is in charge of health care provision and also medical education in the related province.2
Public health services are provided through a nation-wide network which is established based on primary health care (PHC) system. In this system, different referral levels have been defined; in rural areas, there is a health house for at least 1500 people. The health house is staffed by a multi-potential community health worker named Behvarz.3 The health houses are supervised by rural health centers. Each rural health center has one or more general practitioners, several health technicians, midwives, and administrative personnel working there. Selected rural health centers also have delivery facilities attached to them.
The first line of health care provision in urban areas is health posts which are similar to health houses but cover much larger population. The health posts are also staffed by three health technicians (usually family health technician, environmental health technician and midwife) who are trained at university level. The health post is under-supervision of an urban health center which is similar to rural health center. The urban and rural health centers in turn are supervised by a district health network. In terms of patient care, the health centers refer to district general hospitals in which there are at least four general specialties including internist, general surgeon, pediatrician and obstetrician. District general hospital in turn refers to the provincial university teaching hospitals as the highest level of referral system.4,5
After establishment of Ministry of Health and Medical Education, the coverage of primary health care increased quantitatively to more than 95% in rural areas; but improving the quality of care remained one of the main concerns in primary health care in Iran especially in urban areas.6 As patient satisfaction is one of the important indicators of quality of primary health care and health care performance,7 this study aimed to assess the satisfaction degree with primary health care in urban health centers of Tehran, the capital of Iran to define which areas could be focused to improve efficacy of their health services in met-ropolitans.
Methods
Through a cross-sectional study, clients of four urban health centers of primary health care in Tehran, the capital of Iran, participated in this study. These centers were supervised by Shahid Beheshti University of Medical Sciences and Health Services which is responsible for health provision of different socio-economic classes in most areas of Tehran. These centers were randomly selected through strata of different socio-economics classes.
The study was conducted in the waiting room of the four selected health centers over a period of 120-days from Nov 2009 to March 2010. Four hundreds participants from Tehran were selected through a convenient sampling, one hundred from each center. They lived in the geographic zone of the health center and registered in the center or requested for physician's visit and were included in the study after signing informed consent agreement to be as a participant.
Persian version of a validated questionnaire was used as data collecting tool. It covers the standard domains used in North American and European surveys by other authors, including Donabedian,8 Ware et al.9 and Margolis et al..10 It contains 42 items in six major domains including eight items for accessibility of services, six items for continuity of care, eight items for humaneness of staff, five items for comprehensiveness of care, five items for provision of health education, and ten items for effectiveness of services. Each item was scored using a five-point Likert scale. The pilot study was administered by the survey team in order to validate the Persian version of questionnaire. Face and content validity were checked and Chronbach's Alfa calculated as 0.7. Data gathering has been done through the questionnaire by face to face interview.
Variables were listed as age, gender, nationality, chief complaint, literacy, job, type of insurance, type of transportation to health center, number of previous health visits, distance of home from health center, number of chairs in the health center, car parking facilities, time spent in the waiting room, health center operating hours , number of the staff in health center, physical seclusion for men and women, the coverage of health service, presence of the same doctor in each visit, choices for care other than health center, referral system, easy access to medical records, follow up system, vaccination services, respecting the clients by all health center staffs, paying attentions to the clients complaints, respecting clients privacy and culture, malpractice, documentation, periodic checkups of the clients and their family, checking patients’ body temperature, weight, blood pressure and physical examination at every visit, answer to the clients’ questions, explanation of drug instructions by pharmacist, using educational medias (materials, videos, advices), physicians’ access to the medical records of the clients, appropriateness of visit duration, duration of the laboratory tests, access to medications (available in local pharmacies), skillful doctors, physical environment, and clients’ overall satisfaction with the health service of the center.
Finally, positive records in Likert scale for domains of satisfaction recoded to 1 and 2, negative records recoded to -1 and -2 and neutral records recoded to zero and analyzed again. Mean of each domain then divided by the number of items in each domain and the domains ranked based on this score.
Data were analyzed by SPSS software (Version 16.0). The descriptive statistics, chi-square and t-tests were used when appropriate. The P values of less than 0.05 were considered to be significant.
The project received approval from the Shahid Beheshti University of Medical Sciences.
Results
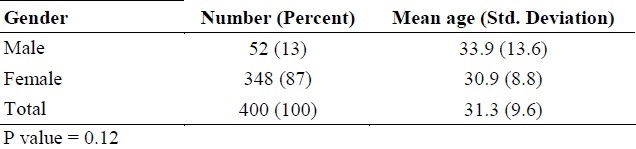
The mean age of users of health services was 31.3 years (SD=9.6). Minimum and maximum age of participants was 13 and 85 years, respectively. Only 13 percent of users of health services were male (table 1). Among participants, 93 (23.5%) had higher education degree, 172 (43.5%) had diploma, 117 (29.6%) had primary and secondary school, and only 13 (3.2%) were illiterate. Highly educated people satisfied with health services less than the others (P< 0.001). More than 24% of participants had no insurance coverage. The most common reasons for seeking health services reported as vaccination (22.8%) and family planning (20.3%), children care (18.3%), maternal care (3.8%), and common cold (12.5%). Other non-medical (16.2%) and other medical (6.1%) issues were the remaining causes of getting to the health centers.
Table 1.
Age and sex distribution of clients in the selected Health Centers in Tehran
Most of the clients were satisfied by the operating hours of the clinics, comprehensiveness of services, sufficiency of health center stuff, presence of the same doctor at each visit, entertainment and facilities of clinic, adequacy of the chairs in the waiting room, privacy and confidentiality, accurate documentation, answer to all questions, delivering the medical file in each visit, time spent for visit, availability of drugs, trust on physicians and medical stuff, clean and tidy health center, vaccination services, gender separation in health centers, respectful behavior of physician, staff and reception, waiting time for visit and visit duration.
Two-thirds of the clients had no need to be referred to hospital or transfer of medical records from hospital to the health center.
Active follow-up, contest on services, disrespectfulness to believes and traditions, mistreating, periodical check-up, checking temperature, weight, blood pressure and comprehensive physical examination in all visits, accuracy of diagnosis, trust on laboratory tests, properly working equipment was much less indicated in the participants.
Level of satisfaction was not high with respectful behavior of laboratory staff, checking temperature, weight, and blood pressure in all visits, description on the way of taking drug, educational materials, helpful education and advice, car parking and facilities of clinic and the educational videos in the health centers.
The distance from home to clinic was suitable in 256 clients. Most of them (51.3%) accessed the health centers by walking. 119 subjects claimed that the car parking and facilities of clinic was not enough. The outcome of the existing visits for 218 (62.8%) subjects was visiting without prescription of medication, drug prescription for 86 (24.8%), advise to specialist outpatient visit for 5 (1.4%) and refer to hospital for 3 (0.9%).
In a question about overall satisfaction with primary health care system, results of Likert scale were 31 (7.8%) very much, 57 (14.4%) much, 231 (58.8%) suitable, 59 (14.9%) few and 17 (4.3%) very few. Overall satisfaction (P>0.05) and different domains of satisfaction (P>0.05 for all) were not affected by gender except for continuity of care (P=0.04).
When positive records in Likert scale for domains of satisfaction recoded to 1 and 2, negative records recoded to -1 and -2 and neutral records recoded to zero, the calculated mean and standard deviation are shown in table No. 2. By dividing mean of each domain to number of items in each domain, the domains ranked as Humanness of staff, Effectiveness of services, Access to services, Continuity of care, Comprehensiveness of care, Provision of health educational materials.
Table 2.
Means for domains of satisfaction in the selected Health Centers in Tehran
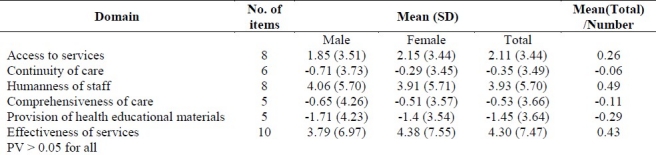
The mean scores of six mentioned domains also analyzed based on sex of participants. As shown in (table No. 2) men's satisfaction with the cares has no difference in any of six dimensions with women.
Discussion
The purpose of this study was to assess the satisfaction of clients with the primary health care system in Tehran, the capital of Iran. The results showed that overall satisfaction, access to services, humanness of staff and effectiveness of services had acceptable situation in clients’ perspective whereas continuity of care, comprehensiveness of care, provision of health educational materials needed more attention to provide an effective health services.
High overall satisfaction with primary health care showed that successful service provision through this system is based on stakeholders need. This can be considered as a key measure for assessment of the quality of health services and predictor of compliance11 and utilization12 which is associated with the continuity of care,13,14 the physician's communication skills15,16 and confidence in the primary health care system.17
Nada Al Emadi et al.18 found the overall satisfaction of 75% which was less than ours (80%). Emadi's highest score of satisfaction domains was for accessibility to the health services and the lowest was for comprehensiveness of care. These two domains in our study were in middle ranks. Our study supported the Margolis's finding10 that reported continuity of health care and health education scores as the lowest and effectiveness and humanness as the highest scores although its overall satisfaction was lower than that in our study.
Extension of primary health care in Iran mainly focused on rural areas. Its primary health care coverage increased to more than 95% in rural areas as health houses and rural health centers since 1972.3 In urban areas, access to health care services through private sector has been reported good; so extension of urban public health centers have been considered only during last few years. This policy has been led to higher levels of equity in health between rural and urban areas.19
Most Iranians get to the primary health care centers for vaccination and family planning. Private sector in Iran has an important role in lesser utilization of public services in men and highly educated people in Iran as men are at work during the day and prefer to use private sector services. Treatment of the inpatients and even outpatients is not the main concern in public health centers, as the private sector covers most of them especially in urban areas.2 Some weak points of service provision may be related to this fact that in Iran the main activity of health centers is towards health promotion and disease prevention but in other countries which use primary health care as the core of care provision, like Oman, health centers cover inpatient and emergency situations and have more physicians and more working time.20
Continuity of care was one of the partially week points of primary health care system in urban area. The best description might be absence of the family physician. It is reported that low patient satisfaction which is associated with lower trust in caregivers and greater chance of physician change results in lesser continuity of care. Since 2003, a new wave of reform started in Iranian health system based on World Health Organization recommendations. The reform targeted the functions of health system especially financing21 and family physician as a position defined in the health system.22 All the villages and cities with a population of less than 20,000 were covered by family physicians and now it is in extension phase to larger cities. It will cover the gap of service provision in urban areas and in future can improve the patient's view on the acceptability of the primary care.23 Also, using evidenced-based clinical practice guidelines and protocols have been considered in this reform which can lead to delivering high-quality care.24
In accessibility to service's criteria, the parking facility was significantly dissatisfactory. Most of Iranians get the health centers by walking; it may be due to short distance of the centers to their living places. It should be considered whether living far from these centers is a barrier for access to public health services.
In Iran, female staffs are responsible for family planning, maternal care and other women cares. Hansen et al. found that for female patients, being visited by a female provider was associated with higher perceived quality as we found in Iranians.25
This study paid attention to users of health services in urban area and had no focus on people did not use the primary health care services at all. As this is a different target population, further studies should develop to assess this issue.
Primary health care introduced as the best strategy for attaining the goal “health for all, 2000” by WHO in 1978 and again has been paid attention in 2008; WHO annual report in 2008 was named “Primary health care: now more than ever”.19 Public health authorities can use the results of this study for evidence based policy making on service provision. The results showed the weaknesses of primary health care system from clients view points. For quality improvement, it is important to consider all views of all stakeholders in a systematic way. This study focused on clients as one of the main stakeholders of service provision process.
Conclusion
Primary health care could be recommended as a comprehensive and suitable strategy to provide health services in public health even in metropolitans. Paying attention to clients’ satisfaction is a basic step for quality improvement and should be done intermittently. In Tehran and most different areas, the overall satisfaction had acceptable situation from users’ perspective. Package of services in primary health care may affect clients’ satisfaction degree. Using family doctors may improve the indices.
Authors’ Contributions
MRS was the manager of the entire project, consultant for design, analyzing the data and finalizing the manuscript; RMA was responsible for drafting the initial design proposal, reports, and data collection.
Acknowledgments
We would like to thank authorities of Shahid Beheshti University of Medical Sciences and also managers and staff of Torab Health center, 12 Bahman Health center, Beasat-Alnabi Health center and Hazrate Roghaiah Health center for their invaluable support and help for collecting data.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Statistical Center of Iran. Statistical pocketbook of The Islamic Republic Of Iran 2006 - 2007 [Online] 2009. [cited 2010 June.1]. Available from: URL: http://amar.sci.org.ir/index_e.aspx .
- 2.Mehrdad R. Health system in Iran. JMAJ. 2009;52(1):69–73. [Google Scholar]
- 3.Barzegar MA, Djazayery A. Evaluation of rural primary health care services in Iran: report on vital statistics in West Azarbaijan. Am J Public Health. 1981;71(7):739–42. doi: 10.2105/ajph.71.7.739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Couper ID. Medicine in Iran: A brief overview. SA Fam Pract. 2004;46(5):5–7. [Google Scholar]
- 5.Shadpour K. Primary health care networks in the Islamic Republic of Iran. East Mediterr Health J. 2000;6(4):822–5. [PubMed] [Google Scholar]
- 6.Sadrizadeh B. Primary health care experience in Iran. MJIRC. 2004;7(1):79–90. [Google Scholar]
- 7.Cleary PD, McNeil BJ. Patient satisfaction as an indicator of quality care. Inquiry. 1988;25(1):25–36. [PubMed] [Google Scholar]
- 8.Donabedian A. Evaluating the quality of medical care.1966. Milbank Q. 2005;83(4):691–729. doi: 10.1111/j.1468-0009.2005.00397.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ware JE, Jr, Davies-Avery A, Stewart AL. The measurement and meaning of patient satisfaction. (3-15).Health Med Care Serv Rev. 1978;1(1):1. [PubMed] [Google Scholar]
- 10.Margolis SA, Al-Marzouq S, Revel T, Reed RL. Patient satisfaction with primary health care services in the United Arab Emirates. Int J Qual Health Care. 2003;15(3):241–9. doi: 10.1093/intqhc/mzg036. [DOI] [PubMed] [Google Scholar]
- 11.Kincey J, Bradshaw P, Ley P. Patients’ satisfaction and reported acceptance of advice in general practice. J R Coll Gen Pract. 1975;25(157):558–66. [PMC free article] [PubMed] [Google Scholar]
- 12.Roghmann KJ, Hengst A, Zastowny TR. Satisfaction with medical care: its measurement and relation to utilization. Med Care. 1979;17(5):461–79. doi: 10.1097/00005650-197905000-00002. [DOI] [PubMed] [Google Scholar]
- 13.Williams SJ, Calnan M. Key determinants of consumer satisfaction with general practice. Fam Pract. 1991;8(3):237–42. doi: 10.1093/fampra/8.3.237. [DOI] [PubMed] [Google Scholar]
- 14.Nutting PA, Goodwin MA, Flocke SA, Zyzanski SJ, Stange KC. Continuity of primary care: to whom does it matter and when? Ann Fam Med. 2003;1(3):149–55. doi: 10.1370/afm.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Weiss GL, Ramsey CA. Regular source of primary medical care and patient satisfaction. QRB Qual Rev Bull. 1989;15(6):180–4. doi: 10.1016/s0097-5990(16)30289-5. [DOI] [PubMed] [Google Scholar]
- 16.Tung YC, Chang GM. Patient satisfaction with and recommendation of a primary care provider: associations of perceived quality and patient education. Int J Qual Health Care. 2009;21(3):206–13. doi: 10.1093/intqhc/mzp006. [DOI] [PubMed] [Google Scholar]
- 17.Weiss GL. Patient satisfaction with primary medical care.Evaluation of sociodemographic and predispositional factors. Med Care. 1988;26(4):383–92. doi: 10.1097/00005650-198804000-00007. [DOI] [PubMed] [Google Scholar]
- 18.Emadi NA, Falamarzi S, Al-Kuwari MG, Al-Ansari A. Patients’ satisfaction with primary health care services in Qatar. MEJFM. 2009;7(9):4–9. [Google Scholar]
- 19.Geneva: World Health Organization; 2008. World Health Organization. The World Health Report 2008 - Primary Health Care (Now More Than Ever) [Google Scholar]
- 20.Annual Health Report. Masghat: Ministry of Health Sultanate of Oman; 2008. Ministry of Health Sultanate of Oman,Department of Health Information &Statistics. [Google Scholar]
- 21.Geveva: World Health Organization; 2000. World Health Organization, World Health Staff. The World Health Report 2000 - Health Systems: Improving Performance. [Google Scholar]
- 22.Sohrabi MR, Saadat S, Hajihashemi Z. Family medicine Residency Program: Is it Worth to Establish? Teb va Tazkieh. 2004;55(3):66–74. [Google Scholar]
- 23.Marcinowicz L, Konstantynowicz J, Chlabicz S. The patient's view of the acceptability of the primary care in Poland. Int J Qual Health Care. 2008;20(4):277–83. doi: 10.1093/intqhc/mzn020. [DOI] [PubMed] [Google Scholar]
- 24.Al-Ahmadi H, Roland M. Quality of primary health care in Saudi Arabia: a comprehensive review. Int J Qual Health Care. 2005;17(4):331–46. doi: 10.1093/intqhc/mzi046. [DOI] [PubMed] [Google Scholar]
- 25.Hansen PM, Peters DH, Viswanathan K, Rao KD, Mashkoor A, Burnham G. Client perceptions of the quality of primary care services in Afghanistan. Int J Qual Health Care. 2008;20(6):384–91. doi: 10.1093/intqhc/mzn040. [DOI] [PubMed] [Google Scholar]