

Abstract
Background:
Influenza viruses cause annual epidemics and occasional pandemics that have claimed the lives of millions. Understanding the role of specific perceptions in motivating people to engage in precautionary behavior may help health communicators to improve their messages about outbreaks of new infectious disease generally and swine flu specifically.
Objectives:
To study the knowledge and practices of health care providers regarding swine flu and to study the attitudes and practices of health care providers toward the prevention of the swine flu epidemic.
Materials and Methods:
The present study was a cross-sectional (descriptive) study and was conducted in the month of September, 2009, among doctors and nurses. A maximum of 40% of the total health care providers of GTB Hospital were covered because of feasibility and logistics, and, therefore, the sample size was 334.
Results:
Around 75% of the health care providers were aware about the symptoms of swine flu. Mostly, all study subjects were aware that it is transmitted through droplet infection. Correct knowledge of the incubation period of swine flu was known to 80% of the doctors and 69% of the nurses. Knowledge about high-risk groups (contacts, travelers, health care providers) was observed among 88% of the doctors and 78.8% of the nurses. Practice of wearing mask during duty hours was observed among 82.6% of doctors and 85% of nurses, whereas of the total study population, only 40% were correctly using mask during duty hours.
Conclusions:
Significant gaps observed between knowledge and actual practice of the Health Care Provider regarding swine flu need to be filled by appropriate training. Data indicate that the health care providers are very intellectual, but they do not themselves practice what they preach.
Keywords: Swineflu, H1N1, pandemic, health care provider, influenza
Introduction
The outbreak of human infection due to the novel swine-origin influenza A (H1N1) virus began in Mexico in March 2009. Because clinical symptoms of infection with the novel influenza virus do not differ from those of seasonal human influenza, there is a continued need for subtyping and laboratory confirmation.(1) Pigs experimentally infected with pandemic 2009 H1N1 influenza A virus developed respiratory disease; however, there was no evidence for systemic disease to suggest that pork from pigs infected with H1N1 influenza would contain infectious virus.(2) Evidence that this new strain could pass from human to human led the World Health Organization quickly raising its pandemic alert level to phase 5, representing “a strong signal that a pandemic is imminent and that the time to finalize the organization, communication and implementation of the planned mitigation measures is short.” This was subsequently raised to phase 6, indicating that a full global pandemic was under way. Given the lack of any specific vaccine against swine flu, mitigation measures have so far focused on identifying, treating and isolating people who have the disease and educating the public about the steps that individuals can take to reduce the risk of transmission. These recommendations include using tissues when sneezing, washing hands regularly with soap and water and setting up a network of “flu friends” to provide mutual assistance should someone become ill.(3)
This flu season, health care providers must be prepared to treat patients who have the seasonal flu and also those who have contracted a novel strain of the H1N1 influenza virus. Although H1N1 flu is sometimes incorrectly called “swine flu,” the virus is transmitted from person to person. Symptoms of the H1N1 flu include fever, chills, nausea, vomiting, body aches, lethargy and fatigue, which usually appear in rapid succession. People at high risk include children, pregnant women and those with certain medical conditions. The most common cause of death from the virus is respiratory failure, but other causes of mortality include sepsis, dehydration and electrolyte imbalance.(4) Pneumonia is the most common complication of seasonal influenza. This complication is rare in interpandemic eras, but becomes more frequent when a pandemic occurs. Among nonpulmonary complications of influenza are various forms of central nervous system involvement, including encephalitis, transverse myelitis, aseptic meningitis and the Guillan-Barre syndrome.(5) The first line of defense against H1N1 flu is vaccination. Treatment includes use of antiemetics, antipyretics and respiratory support.(4) Although the majority of hospitalized persons infected with novel influenza A (H1N1) recovered without complications, certain patients had severe and prolonged disease. All hospitalized patients with novel influenza A (H1N1) infection should be monitored carefully and treated with antiviral therapy, including patients who seek care >48 h after the onset of illness.(6) The distribution of proper information to the public on the status of the H1N1/09 virus pandemic will be important to achieve a broad awareness of the potential risks and the optimum code of behavior during the pandemic.(7)
Adequate amounts of vaccine or antivirals are unlikely to be available early on in a pandemic, and the latter could become ineffective because of resistance. These factors have focused attention on the use of nonpharmaceutical public health interventions to inhibit human to human transmission and fueled interest in answering important questions about influenza epidemiology and transmission.(8) Here, the objective of the study was to study the knowledge and practices of health care providers toward the prevention of the swine flu epidemic.
Materials and Methods
A cross-sectional (descriptive) study was conducted in the month of September, 2009 among the doctors and nurses working at Guru Teg Bahadur Hospital associated to UCMS, Delhi.
Doctors (senior residents, junior residents and interns) and staff nurses from the departments having a service component on the hospital side, who have been working for at least the past 6 months in this hospital and gave consent to be a part of the study, were included in the study. Non Academic Junior Residents, Nursing students, those who did not give consent and those who did not respond even after two visits were excluded from the study.
Total estimated doctors and staff nurses were 834 as per information from the Academic Section, UCMS and Administrative office, GTB Hospital. A maximum of 40% of the total health care providers of the GTB Hospital were covered because of feasibility and logistics, and, therefore, the sample size was 334. To meet this sample, a total of 400 health care providers were contacted. A response rate of 83.5% was obtained. Subjects were selected, as far as possible, by proportionate sampling out of the total working staff during the study period. A list of all the health care workers was prepared, separately for each of the categories. Proportionate sample from each category of health care providers was selected from the lists by randomization.
A pretested, semi-open ended questionnaire was used for obtaining sociodemographic profile (of health care providers), knowledge and practices of the respondents regarding swine flu. The questionnaire was interviewer administered. A written permission from the Principal, UCMS and Medical Superintendant at GTB Hospital was taken prior to the study. The subjects selected for the study were contacted personally during the time period of data collection. A written consent from each subject was taken and the respondent was counseled to provide correct information. The information collected was kept strictly confidential and anonymity was maintained.
Results
A total of 334 health care providers were included in the study, of which 161 were doctors (57 Senior Residents, 61 Junior Residents and 43 Interns) and 173 were staff nurses. About one-fourth of the doctors were female, whereas majority of the nurses (98.8%) were females by gender. Majority of the doctors (79.9%) were in the younger age group (<32 years), whereas majority of the nurses (71.1%) were older than 32 years.
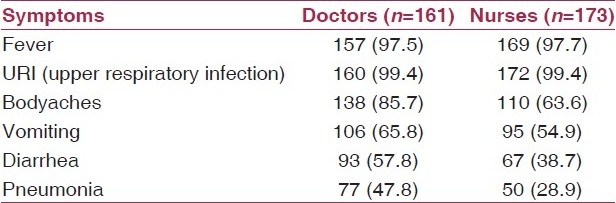
Most of the study participants in both the categories of health care provider had knowledge about the symptoms of H1N1 infection [Table 1]. The common symptoms of swine flu responded were fever, upper respiratory infection, body aches and vomiting.
Table 1.
Knowledge about the symptoms of swine flu
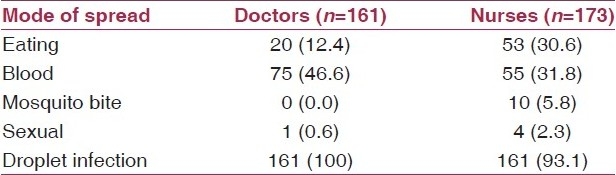
The period of communicability of H1N1 infection (10 days) was correctly known to 81.4% of the health care providers. Respiratory mode of spread of infection was answered correctly by all the doctors as compared with 93.1% of the nurses. Surprisingly, about half of the doctors and one-third of the nurses had misconceptions that it can be transmitted by blood; one-fifth of the respondents opined that swine flu can also be spread by consuming food infected with H1N1 virus [Table 2].
Table 2.
Knowledge regarding the mode of spread of swine flu
As far as the incubation period of the swine flu disease is concerned, 93.2% of the doctors and 68.8% of the nurses replied it correctly as 1–7 days.
Majority of the study participants (70%) opined that contacts, health care providers and travelers were exposed to the risk of infection. About 30% remained clueless about the high-risk population of swine flu disease. Knowledge about who are at a higher risk of developing complications after getting H1N1 (i.e., children <5 years, pregnant women, geriatric population and persons suffering from chronic disease) was higher among doctors (83%) as compared with nurses (71%).
In the present study, 97% of the health care providers knew that government hospitals are the only place where swine flu tests were being performed. Throat swab examination is the correct method for diagnosing swine flu infection, correctly known to majority of the respondents (doctors 97.5%, nurses 92.5%).
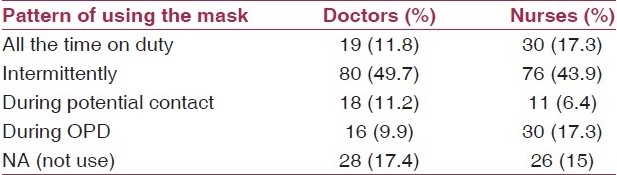
Home quarantine for 7–10 days is an effective method to prevent the spread of infection, correctly known to majority of the doctors (85%) as compared with nurses (59%). A distance of 6 feet to be maintained from a patient of swine flu was rightly known to 55% of the study subjects. About four-fifths of the doctors and 53.2% of the nurses had the knowledge of Personal Protective Equipments (PPE) [Figure 1]. Of this, about three-fourth of doctors and 45% of the nurses knew about various components of PPE (i.e., N95 mask, gloves, gown, cap and shoes). A comparable proportion of doctors (82.6%) and nurses (85%) reported wearing of mask while on duty. Of this, only 20.4% of the nurses and 14.3% of the doctors were wearing the face mask all the time on duty. Majority of the nurses (74.6%) as compared with doctors (20.5%) knew that the mask needs to be changed after 6 h of use [Table 3].
Figure 1.
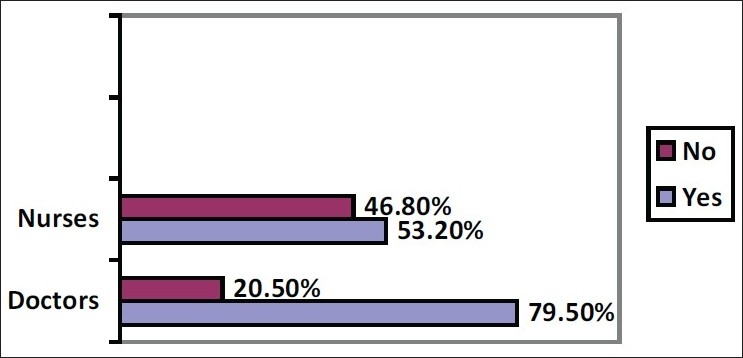
Correct knowledge of PPE
Table 3.
Pattern of use of mask
Correct practice of removing the face mask (lower string to be untied first) was known to 48% of the doctors and 44.5% of the nurses. Proper disposal of the used face mask (either in a yellow bag or treat with hypochlorite solution) was practiced by about three-fifths of the doctors as compared with half of the nurses.
Three or more habits were changed by the health care providers to prevent the infection. About 95% of the doctors and 85% of the nurses knew about the effective treatment (Oseltamivir) available against swine flu. The major side-effects of Oseltamivir elicited were gastritis, vomiting and depression.
Majority of the doctors (70.8%) and nurses (67%) agreed that enough measures were taken by the hospital authorities to prevent and control the swine flu epidemic. Surprisingly, one-third of the health care providers responded that vaccine against swine flu is available, while actually it was not when this study was conducted.
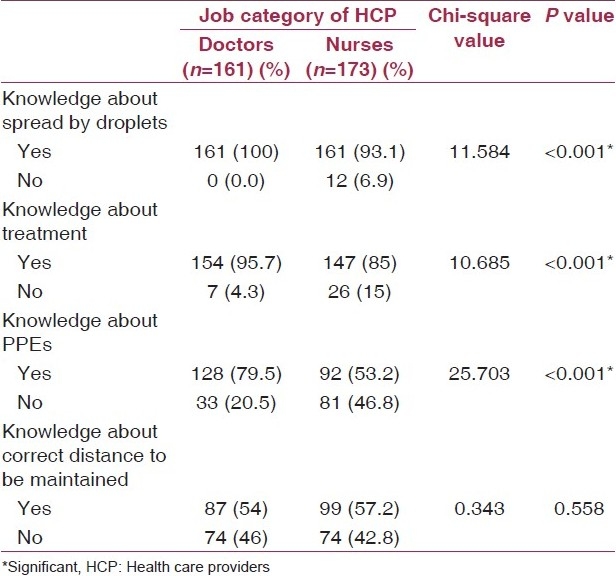
Doctors had better knowledge about the mode of spread, treatment and PPE as compared with nurses, and this difference was statistically significant (P<0.001) [Table 4].
Table 4.
Results of cross.tabulations with job category of HCP
Discussion
Influenza A viruses causes recurrent outbreaks at the local or global scale, with potentially severe consequences for human health and the global economy. Swine influenza virus infections in humans have been reported in the United States, Canada, Europe and Asia. There are no unique clinical features that distinguish swine influenza in humans from typical influenza. Although a number of the case patients have predisposing immunocompromising conditions, healthy persons are also clearly at risk for illness and death from swine influenza. Sporadic cases of swine influenza in humans, combined with seroepidemiological studies demonstrating increased risk of swine influenza in occupationally exposed workers, highlight the crucial role that this group may play in the development of new strains of influenza virus. Persons who work with swine should be considered for sentinel influenza surveillance, and may be an important group to include in pandemic planning.(9)
In the present study, 93% doctors and 84% nurses had knowledge that the drug tamiflu (Oseltamivir) is effective against swine flu. As per the Center for Disease Control and Prevention (CDC), tamiflu is very effective among swine flu-positive patients.(6)
As expected, doctors had better knowledge as compared with nurses about swine flu due to their educational level. When it comes to practice the prevention against the disease, nurses are the front runners.
Rubin et al. conducted a study among the general population to assess whether perceptions of the swine flu outbreak predicted changes in behavior among members of the public in England, Scotland and Wales.(2) Here, it had been seen that 37.8% of the participants (n=377) reported performing any recommended behavior change over the past 4 days because of swine flu, whereas our study was conducted among a different group of the study population, where 59% of the study participants changed habits as a preventive step against the transmission of infection. Here, the percentage was high because in this study, the participants were health care providers and, therefore, they were expecting more knowledge about the preventive measures and also the first contact person with swine flu-positive patients.
Behavior modification is an important preventive strategy to contain the spread of H1N1 infection was demonstrated by a majority of the health care providers. Statistically significant differences were observed among doctors and nurses regarding knowledge of mode of spread of infection, PPEs, medicine for swine flu treatment and availability of vaccine (P < 0.001).
Conclusion
Significant gaps observed between knowledge and actual practice of the health care providers regarding swine flu need to be filled by appropriate training. Data indicate that the health care providers are very intellectual, but they do not themselves practice what they preach.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Cutler J, Schleihauf E, Hatchette TF, Billard B, Watson-Creed G, Davidson R, et al. Investigation of the first cases of human-to-human infection with the new swine-origin influenza A (H1N1) virus in Canada. CMAJ. 2009;181:159–63. doi: 10.1503/cmaj.090859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vincent AL, Lager KM, Harland M, Lorusso A, Zanella E, Ciacci-Zanella JR, et al. Absence of 2009 pandemic H1N1 influenza A virus in fresh pork. PLoS One. 2009;4:e8367. doi: 10.1371/journal.pone.0008367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rubin GJ, Amlôt R, Page L, Wessely S. Public perceptions, anxiety, and behaviour change in relation to the swine flu outbreak: Cross sectional telephone survey. BMJ. 2009;339:b2651. doi: 10.1136/bmj.b2651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ball K. The enigma of the H1N1 flu: Are you ready? AORN J. 2009;90:852–66. doi: 10.1016/j.aorn.2009.11.048. [DOI] [PubMed] [Google Scholar]
- 5.Petrosillo N, Di Bella S, Drapeau CM, Grilli E. The novel influenza A (H1N1) virus pandemic: An update. Ann Thorac Med. 2009;4:163–72. doi: 10.4103/1817-1737.56008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention (CDC). Hospitalized patients with novel influenza A (H1N1) virus infection - California, April-May, 2009. MMWR Morb Mortal Wkly Rep. 2009;58:536–41. [PubMed] [Google Scholar]
- 7.Michaelis M, Doerr HW, Cinatl J., Jr An influenza A H1N1 virus revival - pandemic H1N1/09 virus. Infection. 2009;37:381–9. doi: 10.1007/s15010-009-9181-5. [DOI] [PubMed] [Google Scholar]
- 8.Aledort JE, Lurie N, Wasserman J, Bozzette SA. Non-pharmaceutical public health interventions for pandemic influenza: An evaluation of the evidence base. BMC Public Health. 2007;7:208. doi: 10.1186/1471-2458-7-208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Myers KP, Olsen CW, Gray GC. Cases of swine influenza in humans: A review of the literature. Clin Infect Dis. 2007;44:1084–8. doi: 10.1086/512813. [DOI] [PMC free article] [PubMed] [Google Scholar]