

Abstract
Background:
In recent times, domestic violence against women by marital partners has emerged as an important public health problem.
Objectives:
1. To determine the prevalence, characteristics and impact of domestic violence against nurses by their marital partners, in Delhi, India. 2. To identify nurses’ perceptions regarding acceptable behavior for men and women.
Materials and Methods:
A facility-based pilot study was conducted at All India Institute of Medical Sciences (AIIMS), New Delhi. Data were collected using self-administered standardized questionnaire, among 60 ever married female nurses working at AIIMS hospital, selected by convenience sampling. The principal outcome variables were controlling behavior, emotional, physical and sexual violence by marital partners. Data were analyzed using SPSS 12 software. The test applied was Fisher's exact test and 1-sided Fisher's exact test.
Results:
Sixty percent of nurses reported marital partner perpetrated controlling behavior, 65% reported emotional violence, 43.3% reported physical violence and 30% reported sexual violence. About 3/5th of nurses (58%) opined that no reason justified violence, except wife infidelity (31.67%). Of the physically or sexually abused respondents, 40% were ever injured, and 56.7% reported that violence affected their physical and mental health.
Conclusion:
There is a high magnitude of domestic violence against nurses and this is reported to have affected their physical and mental health.
Keywords: Accepted behavior, domestic violence, nurses, prevalence, impact
Introduction
In recent years, domestic violence against women has emerged as an important social as well as public health problem. Domestic violence by marital partners is the most common form of violence against women. This has emerged as a central concern because it not only impedes women's economic and social development and capacity for self-determination but also has serious impact on their physical and mental health and overall development.(1–3) Domestic violence is manifested through physical, sexual, psychological and economic abuse.(1) The “protection of women from Domestic Violence Act, 2005” says that any act, conduct, omission or commission that harms or injures or has the potential to harm or injure will be considered domestic violence by the law. Even a single act of omission or commission may constitute domestic violence.(4,5)
Globally 20-50% women continue to suffer from domestic violence.(1) A WHO multi-country study reported that the proportion of women who had ever experienced physical or sexual violence or both by an intimate partner ranged from 15 to 71% with the majority between 29 and 62%.(2) In India, the third National Family Health Survey (NFHS-3) shows that at least 37.2% ever-married women have ever experienced spousal violence. The few studies available in India reveal high physical abuse of Indian women ranging from 18 to 70%.(6–12) Evidence on psychological and sexual violence is very limited. In a community-based study in India, of the 40% women who reported experiencing any violence during their marriage, 56% indicated to have poor mental health.(13) A multisite study revealed that 15% of the women reported one or more incidents of forced sex.(14)
Nursing is one of the most women-centered profession and is impacted by violence on several fronts. The nature of duty, and work schedules of nurses are unique that can have distinct implications for their family life experiences with marital partners. There are high levels of role conflict with the domestic role and significant level of occupational stress. Nurses may have been recipients of abuse or witnessed abuse, either at home or work place. Nurses with knowledge of either personal experience of domestic violence or experience among family and friends were better care providers for victims.(15,16) Limited studies are available on prevalence of domestic violence against nurses globally. In India, statistical evidence on the prevalence of domestic violence against nurses, its characteristics and impact, and their perceptions regarding acceptable behavior for men and women is nonexistent. To understand the issues related to domestic violence among nurses present study was planned. Domestic violence is a sensitive and intimate issue. The researchers were not certain whether such information will be provided by the subjects or not. So, this study was planned as a pilot study.
Materials and Methods
This descriptive, exploratory facility-based survey was conducted at All India Institute of Medical Sciences (AIIMS), New Delhi. AIIMS is an autonomous tertiary care hospital engaged in educational, research and patient care services. From its various departments, four departments were selected for sampling of participants i.e., main hospital, private ward (new and main hospital), Dr. Bhim Rao Ambedkar Institute Rotary Cancer Hospital (BRAIRCH) and Dr. Rajendra Prasad Centre for Ophthalmic Sciences (RPC) where nurses function in three shifts. Using convenience sampling 60 ever-married nurses were proportionately sampled from the list of 1150 nurses of the selected departments. Categories of nurses included Assistant Nursing Superintendent(ANS), Sister Grade I (sister-in-charge) and Sister Grade II (staff nurse).
A WHO multicountry study on women's health and life experiences Questionnaire version 10, 2003(17) was adapted to collect data through self report from October to November 2009. Information was obtained on sociodemographic characteristics i.e., family/household characteristics, demographic characteristics of respondents and their husbands, nurses’ opinion about acceptable behavior for men and women, domestic violence and the consequent injuries and impacts.
Domestic violence/marital partner violence is defined as any act of physical, sexual, emotional or social violence against a person within or beyond the confines of home. The terms violence and abuse have been used interchangeably. Physical violence is defined as the use of physical force against a person that results in physical, sexual or psychological harm and includes acts like slapping, pushing, hitting with fist, kicking, choking and use of weapon, etc. Sexual violence consisted of violent sexual acts like nonconsensual sex, physically forced sex and any degrading or humiliating sexual act. Emotional/psychological violence was measured by violent emotional acts like humiliation, intimidation and threatening to hurt. Social violence/controlling behavior refers to the general attempts to restrict contact with one's family of birth and friends, ignoring and treating indifferently, being suspicious that she is unfaithful or expecting her to ask his permission before seeking health care for herself. These definitions of violence have been identified based on previous studies in other settings.(2,7)
Marital partners referred to “current or ever married partners” of respondents. Minor injuries include cuts, punctures, bites, scratches, abrasions, bruises, sprains or dislocations. Major injuries referred to penetrating injury, deep cuts, gashes, broken eardrum, eye injuries, fractures, broken bones, broken teeth or internal injuries.
Permission for data collection was obtained from Chief Nursing Officer, AIIMS. Nurses were contacted individually and informed written consent was obtained. Data were collected using questionnaire in English in their respective areas of work while maintaining anonymity and confidentiality.
Data were analyzed using SPSS 12.0 package and applying Fisher's exact test and 1-sided Fisher's exact test.
Results
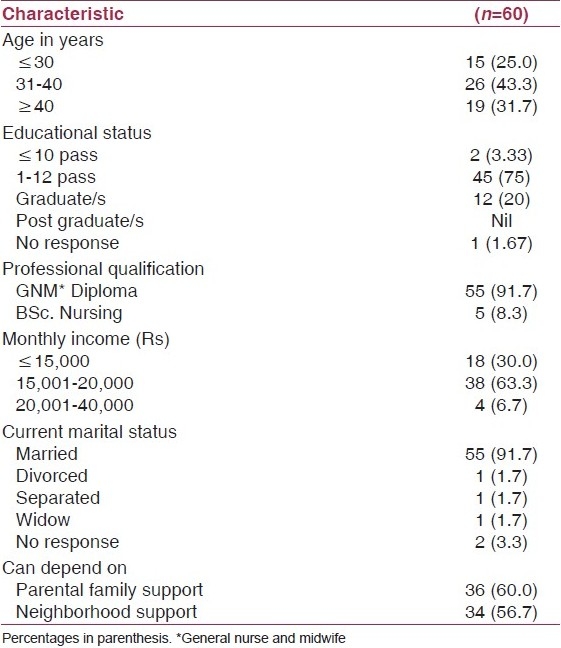
Eight of the eligible study subjects refused to participate in study citing various reasons like shortage of time (n=5), study requiring too intimate information (n=4), not interested (n=3), and one subject could not be contacted despite three visits to the area of work. Some subjects cited more than one reason. The sociodemographic characteristics of the study population and their marital partners are summarized in Tables 1–3. Most of the study subjects were Sister Grade I (48.3%) followed by Sister Grade II (43.3%). Thirty percent nurses reported that their marriage involved dowry. Majority of study subjects’ husbands (43.3%) were 11th/12th passed or graduate (41.67%). Forty percent of the nurses reported drinking behavior in their husbands.
Table 1.
Distribution of respondents with respect to family characteristics
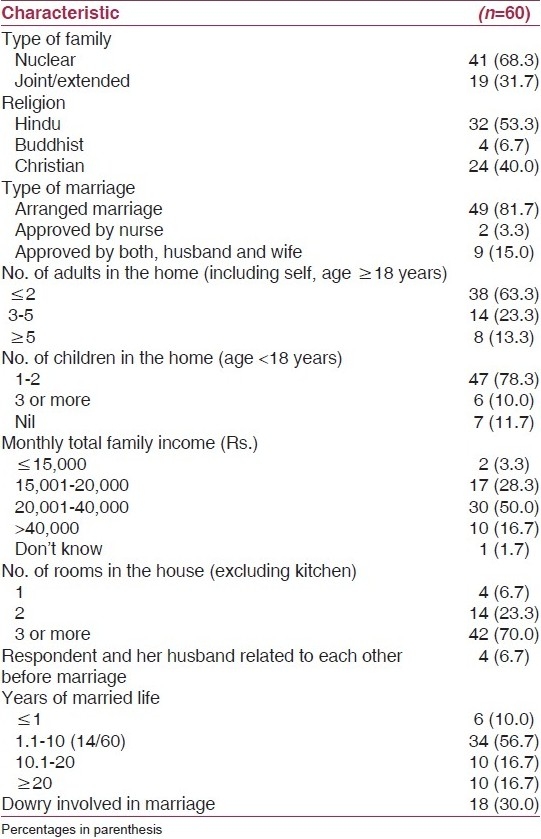
Table 3.
Respondents’ marital partner characteristics
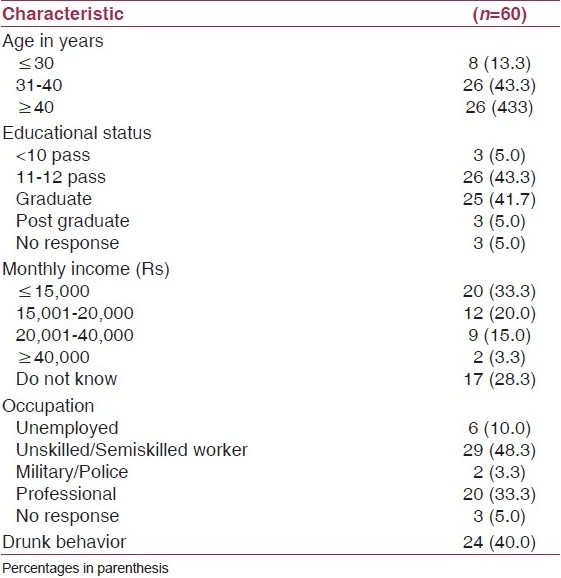
Table 2.
Respondent characteristics
Half of the 60 respondents (50%) agreed that a good wife obeys her husband even if she disagrees. Majority (71.7%) responded that family problems should only be discussed within the family. About 3/5th of respondents (58%) opined that no reason justified violence. The most accepted reason for violence was wife infidelity (31.7%). Acceptance of wife beating was higher among nurses who had experienced violence (46.1%) than those who had not(15.5%). Majority of the respondents agreed that a married woman can refuse to have sex with her husband if she does not want to (70%), if he is drunk (61.67%), if she is sick (78.33%) or if he mistreats her (66.67%). But 10% respondents felt that women did not have the right to refuse sex under any of these circumstances . About half (48.3%) of the study subjects and their husbands quarrel sometimes while 28.3% quarrel often.
Table 4 illustrates the prevalence of domestic violence against nurses by their marital partners. The prevalence of emotional, physical and sexual violence ever in life was 65, 43.3 and 30% respectively. Twenty-three percent(14/60) participants reported both physical and sexual violence while 50% (30/60) reported physical and/or sexual violence showing the overlap. Three-fourth of the study subjects reported at least one form of domestic violence i.e., overall domestic violence. Emotional, physical and sexual violence in the past 1 year (current violence) was reported by 48.3, 35 and 16.7% nurses, respectively. Nurses who were divorced, separated and widow (one each) reported all the three forms of domestic violence i.e., emotional, physical and sexual violence. Of the two nurses who did not reveal their marital status, one reported experiencing emotional as well as physical violence
Table 4.
Prevalence of domestic violence against nurses
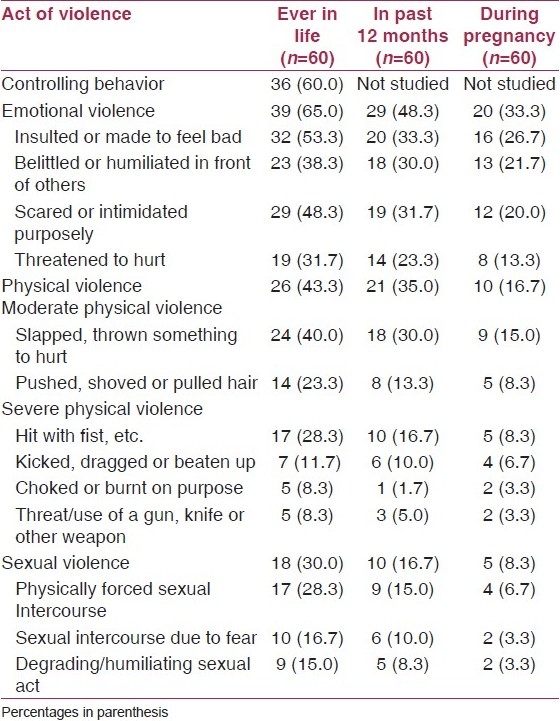
Being slapped was the most common act of physical violence (40%) reported by the respondents. Upto 18.86% (11/60) of ever-pregnant nurses were physically abused, 7.5% were kicked in the abdomen during pregnancy and in 30% cases the slapping/beating got worse than before pregnancy. 45.8% (11/24) of the physically abused victims were kicked or beaten when pregnant. Majority of respondents reported that most of the violent acts were still continuing. Far from being isolated acts of violence, several acts occurred many times.
Forty percent study subjects (12/30) were injured ever in life as a result of acts of physical or sexual violence by (any of) their husband/s. Minor injuries ranged from 25 to 66.7% while major injuries ranged from 8.3 to 16.7%. Also 33.3% were hurt badly enough to have needed health care but only three (25%) received health care for the injuries inspite of being health professionals themselves and having easy access to health care.
Over half of the study subjects (56.7%) reported that physical or sexual violence (n=30) affected their physical and mental health and caused inability to concentrate (56.7%), loss of confidence in own abilities (26.7%) and inability to work/sick leave (23.3%). Also 20% of nurses left home (even if overnight) due to violence and 2 (6.7%) even divorced or separated from their husbands.
It was reported that problems with husband's family was the most common (26%) reason for physical or sexual violence followed by money problems, difficulties at his work and disobedience by wife (20% each). Five (16.7%) nurses reported husband's drinking behavior and their own refusal to sex as the reasons for this violence. Half of the respondents (50%) reported there was no particular reason for violent behavior of husband. Some cited more than one reason.
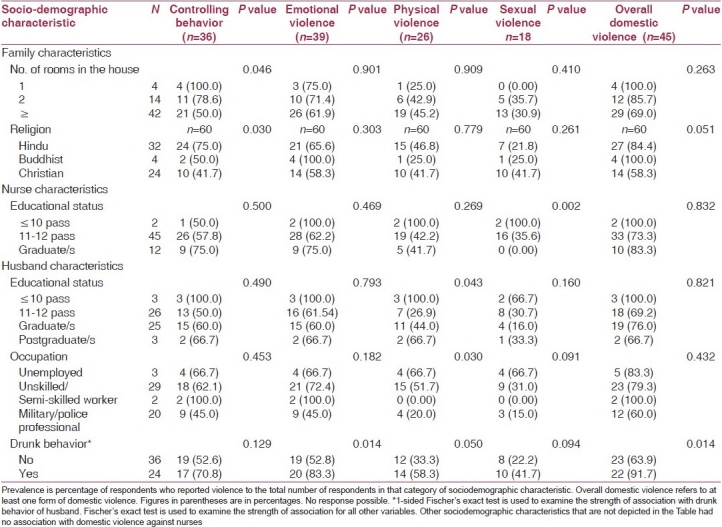
Table 5 depicts the association between the various forms of lifetime domestic violence and some of their sociodemographic characteristics. Fisher's exact test and 1-sided Fisher's exact test (only for drinking behavior) were used for this assessment. A significant association of domestic violence prevalence against nurses was seen with number of rooms in the household (excluding kitchen), religion, education of nurse and education, occupation and drinking behavior of husband. The husband's controlling behavior was lowest in Christians. Physical violence was higher if husband was less educated or unemployed. Sexual violence was significantly decreased as educational levels of respondents increased. No association was observed between domestic violence against nurses and other sociodemographic characteristics i.e., type of family, type of marriage, number of adults and children in the family, the nurse being related to husband before marriage, dowry, monthly income (of nurse, her husband and family); age, current marital status and professional qualification of nurse, years of married life, family and neighborhood support and age of husband.
Table 5.
Association between some sociodemographic characteristics and prevalence of domestic violence
Discussion
Women are often reluctant to reveal their domestic violence status due to shame, fear of ridicule and reprisal by family and friends or belief that no one will understand their plight. In the present study too, four nurses (50%) refused to participate in the study as it required revealing too intimate information.
In the present study wife beating was believed to be justified under certain circumstances by 42% respondents while the International Institute for Population studies reported 56% of Indian women believed wife beating to be justified in certain circumstances.(18) The WHO multicountry study (2005) findings revealed that acceptance of wife beating was higher among women who had experienced violence than those who had not. Also 10-20% women did not have the right to refuse sex under any of the given circumstances.(2) These findings are similar to the findings of the present study.
Sixty percent study subjects in present study reported one or more type of partner controlling behavior. A wide variation (21-90%) in partner controlling behavior has also been reported in WHO multicountry study.(2) Two-thirds (65%) of respondents reported some form of emotional, physical or sexual violence. This high proportion is consistent with high levels of violence against women recorded in other studies in India(6–12) and also in Bangladesh (53-62%).(19) But only 18-25% of nurses reported lifetime physical or sexual intimate partner violence and 22.8-42% have reported experiencing lifetime emotional abuse by an intimate partner in other parts of the world.(20,21)
However, one needs to view these findings cautiously as some of the behavior may not be considered inappropriate by respondents or their marital partners e.g., restricting wife's contact with family or friends, or having sex with wife when she is not willing.
In the present study 45.8% (11/24) of the physical violence victims were kicked or beaten when pregnant. This concurs with earlier findings in India that of the (45%) physical violence victim women, 50% were kicked, beaten or hit when pregnant.(11) The findings reveal that pregnancy does not provide immunity against domestic violence.
In our study, higher violence was reported if husband had lower educational status, or indulged in drinking behavior. The prevalence of violence decreased with increased number of rooms in the house and increase of education of the couple. Increased rooms probably meant more personal space and privacy and hence better understanding. Higher socioeconomic status was also reported to have protective effect against domestic violence in a nation-wide study in India.(10)
Present data revealed that 40%(12) participants were ever injured due to physical or sexual violence. The reasons cited for domestic violence in the present study are almost in concurrence with the findings of Maharashtra study by Jain et al.(7)
The study did not assess the direct costs of domestic violence. But, since 33% of the nurses experiencing domestic violence required medical care; this could lead to significant cost to the health care system as well as loss of productivity.
Limitations
Small sample size and convenience sampling has limited the generalizability of the present study. Being a facility based-pilot study, causal association cannot be established between domestic violence and sociodemographic characteristics.
Conclusions
The present study indicates the high magnitude of domestic violence against nurses. The ongoing nature of violence, its acceptance and frequent justification under any circumstances poses a challenge to their empowerment. The perceived impact of violence in the form of health and other effects like sickness/absenteeism were very high and suggest the need for interventions even at workplace.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Florence, Italy: UNICEF Innocenti Research Centre; 2000. [Last accessed on 2007 Jun 10]. Domestic Violence against Women and Girls. Innocenti Digest, 6. Available from: http://www.unicef.icdc.org/publications/pdf/digest6e.pdf . [Google Scholar]
- 2.Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C. Initial results on prevalence, health outcomes and women's responses. Geneva: World Health Organization; 2005. WHO Multi-country study on Women's Health and Domestic Violence against Women. [Google Scholar]
- 3.Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359:1331–6. doi: 10.1016/S0140-6736(02)08336-8. [DOI] [PubMed] [Google Scholar]
- 4.Kaur R, Garg S. Addressing domestic violence against women: An unfinished agenda. Indian J Community Med. 2008;33:73–6. doi: 10.4103/0970-0218.40871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.The Protection Of Women From Domestic Violence Act, 2005. Indian Laws and Bare Acts at Vakilno1.com. [Last accessed on 2010 Aug 30]. Available from: http://www.vakilno1.com/bareacts/Domestic.Violence/Domestic.Violence.Act.2005.htm .
- 6.Ministry of Health and Family Welfare. National Family Health Survey-3. India fact sheet 2005-06. [Last accessed on 2010 Jul 2]. Available from: http://www.nfhsindia.org/summary.html .
- 7.Jain D, Saron S, Sadowski L, Hunter W. Violence against women in India: Evidence from rural Maharashtra, India. Rural Remote Health. 2004;4:304. [PubMed] [Google Scholar]
- 8.Martin SL, Tsui AO, Maitra K, Marinshaw R. Domestic violence in northern India. Am J Epidemiol. 1999;150:417–26. doi: 10.1093/oxfordjournals.aje.a010021. [DOI] [PubMed] [Google Scholar]
- 9.Vachher AS, Sharma A. Domestic violence against women and their mental health status in a colony in Delhi. Indian J Community Med. 2010;35:403–5. doi: 10.4103/0970-0218.69266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jeyaseelan L, Kumar S, Neelakantan N, Peedicayil A, Pillai R, Duvvury N. Physical spousal violence against women in India: Some risk factors. J Biosoc Sci. 2007;39:657–70. doi: 10.1017/S0021932007001836. [DOI] [PubMed] [Google Scholar]
- 11.Rao V. Wife-beating in rural South India: A qualitative and econometric analysis. Soc Sci Med. 1997;44:1169–80. doi: 10.1016/s0277-9536(96)00252-3. [DOI] [PubMed] [Google Scholar]
- 12.Babu BV, Kar SK. Domestic violence against women in eastern India: A population-based study on prevalence and related issues. [Last accessed on 2009 Jun 8];BMC Public Health. 2009 9:129. doi: 10.1186/1471-2458-9-129. Available from: http://www.biomedcentral.com/1471.2458/9/129.104k . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kumar S, Jeyaseelan L, Suresh S, Ahuja RC. Domestic violence and its mental health correlates in Indian women. Br J Psychiatry. 2005;187:62–7. doi: 10.1192/bjp.187.1.62. [DOI] [PubMed] [Google Scholar]
- 14.International Clinical Epidemiological Network: Domestic Violence in India: A Summary Report of a Multi. Site Household Survey. Washington, DC: International Centre for Research on Women and the Centre for Development and Population Activities; 2000. [Google Scholar]
- 15.Willson P. Domestic Violence: Are Nurses Hiding the Facts? [Last accessed on 2008 Nov 30];Internet J Adv Nurs Pract. 1998 2:1. Available from: http://www.ispub.com/journal/the_internet_journal_of_advance…-60k . [Google Scholar]
- 16.Nurses Can Help Domestic Violence Victims 2001. Springhouse PA: Springhouse. 2001. [Last accessed on 2009 Jan 10]. Available from: http://mentalhealth.about.com/library/sci/0801/blnurse801.htm .
- 17.Final core questionnaire version 10. Department of Gender and Women's Health. Geneva: WHO; 2003. World Health Organization. WHO multi-country study on women's health and life events. [Google Scholar]
- 18.Kidwai R. New Delhi: The Telegraph; 2007. [Last accessed on 2007 Mar 23]. Silent acceptance of violence at home. Available from: http://www.telegraphindia.com/1001117/front_pa.htm . [Google Scholar]
- 19.Khan ME, Aeron A. Prevalence, nature and determinants of violence against women in Bangladesh. J Fam Welf. 2006;52:33–5. [Google Scholar]
- 20.Bracken MI, Messing JT, Campbell JC, La Flair LN, Kub J. Intimate partner violence and abuse among female nurses and nursing personnel: Prevalence and risk factors. Issues Ment Health Nurs. 2010;31:137–48. doi: 10.3109/01612840903470609. [DOI] [PubMed] [Google Scholar]
- 21.Díaz-Olavarrieta C, Paz F, de la Cadena CG, Campbell J. Prevalence of Intimate Partner Abuse Among Nurses and Nurses’ Aides in Mexico. [Last accessed on 2010 Jun 25];Arch Med Res. 2001 32:79–87. doi: 10.1016/s0188-4409(00)00262-9. Available from: http://www.arcmedres.com/article/S0188.4409(00)00262.9/abstract . [DOI] [PubMed] [Google Scholar]