

Abstract
Context
Nicotine-dependent smokers exhibit craving and brain activation in the prefrontal and limbic regions when presented with cigarette-related cues. Bupropion hydrochloride treatment reduces cue-induced craving in cigarette smokers; however, the mechanism by which bupropion exerts this effect has not yet been described.
Objective
To assess changes in regional brain activation in response to cigarette-related cues from before to after treatment with bupropion (vs placebo).
Design
Randomized, double-blind, before-after controlled trial.
Setting
Academic brain imaging center.
Participants
Thirty nicotine-dependent smokers (paid volunteers).
Interventions
Participants were randomly assigned to receive 8 weeks of treatment with either bupropion or a matching placebo pill (double-blind).
Main Outcome Measures
Subjective cigarette craving ratings and regional brain activations (blood oxygen level-dependent response) in response to viewing cue videos.
Results
Bupropion-treated participants reported less craving and exhibited reduced activation in the left ventral striatum, right medial orbitofrontal cortex, and bilateral anterior cingulate cortex from before to after treatment when actively resisting craving compared with placebo-treated participants. When resisting craving, reduction in self-reported craving correlated with reduced regional brain activation in the bilateral medial orbitofrontal and left anterior cingulate cortices in all participants.
Conclusions
Treatment with bupropion is associated with improved ability to resist cue-induced craving and a reduction in cue-induced activation of limbic and prefrontal brain regions, while a reduction in craving, regardless of treatment type, is associated with reduced activation in prefrontal brain regions.
Originally marketed as an atypical antidepressant, bupropion hydrochloride was found to enhance smoking cessation in patients with depression and is now the most commonly recommended nonnicotinic pharmacotherapy for smoking cessation in the world.1 Bupropion improves quit rates2-4 and prolongs abstinence in nicotine-dependent smokers.5,6 Standard 8-week treatment with bupropion (administered with brief counseling) results in approximately 40% short-term abstinence (7 weeks)3 and 20% to 30% long-term abstinence (12 months).4,7,8 Smokers treated with bupropion describe a reduction in nicotine withdrawal symptoms including negative affect, urge to smoke, difficulty concentrating, and irritability.9,10 Numerous studies encompassing a wide spectrum of clinical populations have replicated the success of treatment with bupropion, 11-15 suggesting a common mechanism by which this medication facilitates smoking cessation.
Bupropion and its metabolites appear to modulate smoking-induced dopamine release by increasing extracellular dopamine and norepinephrine levels in subcortical regions (striatum and locus coeruleus, respectively) through the inhibition of dopamine and norepinephrine reuptake transporters.16-24 Enhancing subcortical dopamine and norepinephrine may facilitate smoking cessation by mitigating the effects of nicotine-evoked dopamine transmission from the ventral tegmental area to the ventral striatum, thereby reducing nicotine reward and withdrawal.25,26 Bupropion also acts as an antagonist at nicotinic acetylcholine receptors, decreasing the probability of their activation and desensitization.27-32 Therefore, bupropion may also block nicotinic receptors and reduce the reinforcing value of smoking.33
Environmental cues associated with nicotine reinforcement induce cigarette craving, which propagates smoking habits in smokers and relapse in abstinent individuals. 34-39 Human brain imaging studies using functional magnetic resonance imaging (fMRI) and positron emission tomography scanning have provided insight into brain regions associated with cue-induced cigarette craving. Nicotine-dependent smokers exhibit activation in brain regions related to attention (prefrontal cortex), emotion (amygdala), reward (ventral tegmental area), and motivation (striatum) while viewing cigarette-related cues.40-45 A number of factors including level of nicotine dependence, 46-48 length of abstinence and/or severity of withdrawal, 49-51 expectancy to smoke,52,53 and genotype54 may affect cue-induced neural activation.
Although brain regions mediating cue-induced craving have been closely examined,55 little research has focused on understanding how smoking cessation treatments alter this well-characterized phenomenon. Animal studies of bupropion and nicotine self-administration, discrimination of nicotinelike effects, and reinforcement have provided conflicting evidence regarding the neural mechanisms by which bupropion aids smoking cessation in humans. 56,57 Human studies using positron emission tomography have shown that bupropion treatment attenuates cue-induced increases in glucose metabolism in the anterior and posterior cingulate gyri.58,59 Furthermore, recently abstinent smokers treated with bupropion and group therapy display lower levels of craving and less increase in glucose metabolism in the striatum, thalamus, and midbrain while viewing smoking-related cues compared with identically treated nonabstinent smokers.60 Taken together, these studies establish that smoking cessation treatments not only attenuate self-reported cue-induced craving but also attenuate cueinduced neural activation within the limbic system and associated prefrontal brain regions.
This study aimed to assess the effect of standardized treatment with bupropion on regional brain activation in response to smoking-related cues while participants either passively allowed or actively resisted craving. Based on previous research, we hypothesized that participants treated with bupropion would show a greater treatment-induced reduction in activation of limbic and prefrontal regions associated with cue-induced craving compared with participants treated with placebo. We hypothesized that this effect would be accentuated while participants resisted craving.
METHODS
PARTICIPANTS
Healthy, treatment-seeking cigarette smokers (≥10 cigarettes per day) who met DSM-IV criteria for nicotine dependence were recruited through local newspaper and internet advertisements. Potential participants underwent telephone and in-person screenings. For the telephone screening, a research assistant obtained medical, psychiatric, and substance-abuse histories without personal identifiers. Two study investigators (R.E.O. and A.L.B.) performed the in-person screenings, which included screening questions from the Structured Clinical Interview for DSM-IV61 and administration of the Smoker’s Profile, Fagerström Test for Nicotine Dependence (FTND),62,63 Urge to Smoke Scale,40,64 and Hamilton Depression65 and Anxiety66 rating scales. Potential participants provided breath samples for a carbon monoxide assay, using a MicroSmokerlyzer (Bedfont Scientific Ltd, Kent, England) at the time of initial screening to verify recent smoking. Breath carbon monoxide level (at a cutoff of >5 ppm) is highly associated with self-reported smoking, correlates negatively with time since last cigarette, and correlates positively with carboxyhemoglobin levels.67,68 All participants received a detailed verbal and written description of the study procedures before giving informed consent, as approved by the Greater Los Angeles Veterans Affairs Healthcare System Institutional Review Board.
Exclusion criteria included (1) history of any Axis I psychiatric diagnosis other than nicotine dependence, (2) medical conditions that might affect brain function, (3) current use of medications that could alter brain function, (4) pregnancy, and (5) current illicit drug use other than occasional use of marijuana. All potential participants were required to have a negative result on a urine test for drug use during the in-person screening session and immediately prior to each scanning session. Participants who reported recreational alcohol (≤ 1 drink per day), marijuana (≤ 1 use per week), or caffeine (≤ 2 cups of coffee per day or the equivalent) use who did not meet the criteria for abuse/dependence were allowed to participate but were instructed to abstain for at least 24 hours before scanning.
fMRI PROCEDURE
Thirty-four participants underwent the first fMRI scan within 1 week of the in-person screening. They were instructed to smoke their usual morning cigarette(s) prior to scanning. A research assistant interviewed the participants and measured exhaled carbon monoxide breath samples at the start of each session (7:00 AM) to ensure that they had smoked prior to the fMRI session. The structural MRI image began at 7:15 AM followed by an fMRI scan including neutral and smoking cue videos at 7:25 AM. This procedure standardized the time since the last cigarette (25 minutes) and allowed for moderate craving69 while avoiding the possibility of a ceiling effect caused by prolonged abstinence. Thirty participants underwent an identical posttreatment scan (4 dropouts) while taking the study medication at the end of the 8-week treatment period.
Functional imaging was performed with a 1.5-T Magnetom Sonata scanner (Siemens AG, Erlangen, Germany) using a gradient-echo, echo-planar acquisition sequence in which the repetition time was 2.5 seconds; echo time, 45 milliseconds; flip angle, 80°; image matrix, 128 × 64; field of view, 40 × 20 cm; and in-plane resolution, 3 mm. Sixteen slices, each 4 mm thick, with a 1-mm gap between slices were obtained every 2.5 seconds for 45 seconds while participants were exposed to cigarette-related and neutral cues and during control periods (resting state with neutral visual stimulus: flashing white boxes on black background). High-resolution spin-echo echo-planar scans (128 × 256 matrix; in-plane resolution, 1.5 mm; repetition time, 4000 milliseconds; echo time, 54 milliseconds; 4 excitations) obtained in the same plane as the functional scans were acquired with bandwidth matched to that of the functional studies. The spatial distortions of the functional and high-resolution spin-echo echo-planar imaging scans were held in common to facilitate the subsequent spatial normalization procedure.
CUE PRESENTATION AND CRAVING MONITORING
Our group and a collaborator developed and validated 18 cigarette- related and 9 neutral cue videos used in this study.70,71 The cigarette-related videos include professional actors and actresses smoking in a variety of generic settings (eg, writing a letter, standing outside of a building, driving). The neutral cue videos were similar but included no smoking-related behaviors. Cue videos were 45 seconds in length and were seen from the first-person viewpoint.
Participants viewed the cue videos through MRI-compatible goggles with an attached headphone/microphone headset (MRVision 2000 Ultra; Resonance Technology, Northridge, California). Before scanning, participants received instructions on how to provide craving ratings using an optically isolated universal serial bus interface consisting of a 5-button response box (Rowland Institute at Harvard, Cambridge, Massachusetts). Participants were instructed to respond from 1 (definitely not) to 5 (definitely) on the question, “I crave a cigarette right now” (taken from the Urge to Smoke scale64) immediately following each cue presentation. Owing to the repetitive nature of measuring acute craving and time constraints inherent in the fMRI scanning procedure, a single-item craving questionnaire was substituted for a more comprehensive multidimensional craving survey.72
Each scanning session consisted of 3 runs, with each run including 3 cue conditions. During each run, participants viewed 1 neutral cue video, 1 crave-allow cigarette-related cue video, and 1 crave-resist cigarette-related cue video. Prior to initiation, participants were instructed to allow themselves to crave cigarettes during the cigarette-related cue videos unless explicitly instructed to resist craving (eg, “during the next video clip, try to resist any feelings of craving for cigarettes”). The cue videos were presented in a randomized fashion (Latin square design).
SMOKING CESSATION TREATMENT PROCEDURE
Following the first fMRI scan, participants met with a research physician and were randomly assigned to smoking cessation treatment with either bupropion sustained release (n = 17) or a matching pill placebo (n = 17) in a double-blind fashion. Participants were instructed to start taking 1 pill (150 mg of bupropion or 1 placebo pill) daily for the first 3 days of treatment, followed by titration up to 2 pills daily, separated by 8 hours, for the remaining 8 weeks of treatment. Participants met with the physician weekly to monitor treatment adherence and adverse effects. The physician instructed participants to set a smoking quit date of 2 weeks after the initiation of treatment and continued to encourage participants to quit throughout the study. Participants continued to take bupropion or the pill placebo through the completion of the second fMRI scan. Participants who quit smoking during the study (confirmed by self-reports and exhaled carbon monoxide ≤ 3 ppm) were not required to smoke prior to the second fMRI scan. Three bupropion- treated participants stopped taking the study medication owing to relocation (n = 1), vocational constraints (n = 1), and self-reported lack of efficacy (n = 1). One placebo-treated participant also stopped taking the study medication owing to self-reported lack of efficacy. All of these participants were withdrawn from the study because they did not have both the before-treatment and after-treatment data needed for the primary study analyses, leaving a final sample size of 30. No participants included in the study described significant adverse effects of study medication requiring a reduction in dosage or discontinuation of administration.
DEMOGRAPHIC AND TREATMENT VARIABLES ANALYSIS
Mean (SD) values of demographic and treatment variables were determined independently for each treatment group. To ensure that the randomly assigned study groups were similar at baseline, t tests and a χ2 test (for sex) were performed on the demographic variables. To evaluate treatment outcomes, the treatment groups were compared together and independently using unpaired and paired t tests, respectively, on the primary smoking outcome measures (cigarettes per day, FTND scores, and exhaled carbon monoxide levels).
SELF-REPORTED CRAVING ANALYSIS
A within-subject repeated-measures analysis of variance including a between-group variable (treatment type), was used to test for interactions and/or effects of treatment type (bupropion and placebo), cue condition (crave-allow, crave-resist, and neutral), time (before to after treatment), and run on self-reported craving. Secondarily, craving scores were averaged across the 3 runs for each cue condition and an unpaired t test was used to assess group differences in the self-reported craving for each condition before treatment, after treatment and in the change from before to after treatment. A paired t test was also used to assess within-group differences in self-reported craving for each condition from before to after treatment.
fMRI STATISTICAL ANALYSIS
Preprocessing
Images were preprocessed using FEAT (FMRI Expert Analysis Tool) Version 5.4.2 from the FMRIB Software Library (http://www.fmrib.ox.ac.uk/fsl) and the following steps: motion correction using the Linear Registration Tool (MCFLIRT)73; exclusion of nonbrain areas using the Brain Extraction Tool74; spatial smoothing with a Gaussian kernel of 5mmfull-width at half maximum; mean-based intensity normalization to remove linear trends; and nonlinear, high-pass temporal filtering to exclude low-frequency confounds such as breathing (Gaussian-weighted least squares straight line fit, with σ= 25.0 seconds). Time series statistical analysis was carried out using Improved Linear Model with local autocorrelation correction.75
Level 1: Within-Participant, Within-Run
Voxelwise general linear model analyses of the 3 cue conditions (crave-allow, crave-resist, and neutral) were modeled as explanatory variables in the first-level analysis. Each scan was registered to a high-resolution T1-weighted structural image using FMIRB’s Linear Registration Tool (FLIRT)76 and coregistered to MNI152 (Montreal Neurological Institute, Montreal, Quebec, Canada) standard space. Contrasts at this level compared parameter estimates of the hemodynamic response with the 3 cue conditions vs each of the other cue conditions and rest.
Level 2: Within-Participant, Within-Session
The second-level, within-participant analysis used FMRIB’s fixed effects model. This analysis was conducted individually for each participant to determine the relative activation between cue conditions during before-treatment and after-treatment sessions (crave-allow vs neutral; crave-resist vs neutral; crave-allow vs crave-resist).
Level 3: Between-Group, Before and After Treatment
The third level of analysis assessed between-group differences (bupropion vs placebo) in activation between cue conditions before and after treatment separately using FMRIB’s Local Analysis of Mixed Effects (FLAME 1).77-79 Participant’s self-reported cigarettes per day was measured prior to each fMRI scan, then de-meaned and included as a covariate in the analysis to control for the effect of cigarette use on regional brain activation.
Level 4: Within- and Between-Group, Before to After Treatment
The fourth and primary level of analysis examined pretreatment to posttreatment activation changes within each group and between the 2 groups relative to cue condition using FLAME 1.77-79 Participants’ change in reported cigarettes smoked per day from before to after treatment was de-meaned and included as covariate in this analysis to control for the effect of reduced cigarette use on regional brain activation. A region-of- interest analysis was applied to the regions where significant group differences were observed using FMRIB’s featquery to assess correlations (Pearson) between mean percentage of signal change and change in craving from before to after treatment. (For thoroughness, group differences were also assessed in regions where significant activation/deactivation differences were observed between the crave-resist and craveallow vs neutral conditions in all participants before treatment.)
Level 5: fMRI and Self-reported Craving
The fifth-level analysis examined the relationship between changes in self-reported craving and fMRI activation from before to after treatment in all participants and each treatment group separately using FLAME 1. Participants’ change in self-reported craving from before to after treatment was demeaned and applied as a covariate of interest in this analysis. A region-of-interest analysis was applied to the regions where significant associations were observed using FMRIB’s featquery to assess group differences (unpaired t test) in mean percentage of signal change from before to after treatment.
STATISTICAL PARAMETERS
z Statistic images were thresholded using clusters determined by z > 2.3, with an adjusted corrected cluster significance threshold of P = .05 for the first, second, third, and fourth level of analysis. 80 The fifth level of analysis used clusters determined by z > 2.1, with an adjusted corrected cluster significance threshold of P = .05.
RESULTS
DEMOGRAPHIC AND SMOKING CHARACTERISTICS
No differences were observed between the bupropion-treated participants (n = 14) and the placebo-treated participants (n = 16) on demographic measures or number of years smoking. At the initiation of treatment, no differences were observed between the treatment groups on reported cigarettes per day, exhaled carbon dioxide, or FTND scores. At the completion of treatment, bupropion-treated participants reported significantly lower FTND scores compared with placebo-treated participants (P = .04, 2-tailed t test). Bupropion-treated participants also exhibited greater reductions in FTND scores (P = .04, 2-tailed t test) and exhaled carbon dioxide (P = .02, 2-tailed t test) from before to after treatment than placebo-treated participants. No difference was observed in the number of participants who quit smoking in each treatment group during the study. Within-group analyses revealed that bupropion-treated participants exhibited significant decreases in reported cigarettes per day (P = .001, 2-tailed t test), exhaled carbon dioxide, and FTND scores (P = .001, 2-tailed t test), while placebo-treated participants exhibited significant decreases in reported cigarettes per day (P = .001, 2-tailed t test) and FTND scores (P = .006, 2-tailed t test) but not exhaled carbon dioxide (Table 1).
Table 1.
Demographic and Smoking Characteristics
| Characteristic | Mean (SEM) by Treatment
|
|
|---|---|---|
| Bupropion | Placebo | |
| Age, y | 40.4 (2.8) | 42.9 (3.1) |
| Sex, % | ||
| Male | 64 | 75 |
| Female | 36 | 25 |
| Smoking duration, y | 20.3 (3.9) | 22.5 (3.4) |
| Quit rates, % | 21.4 | 5.3 |
| Cigarettes per day, No. | ||
| Before treatment | 24.4 (2.6)a | 22.8 (2.5)a |
| After treatment | 8.5 (2.5)a | 13.0 (2.8)a |
| Change | -15.9 (3.2) | -9.8 (2.1) |
| Exhaled carbon monoxide | ||
| Before treatment | 24.5 (3.9)a | 20.3 (2.5) |
| After treatment | 13.8 (3.0)a | 18.7 (2.7) |
| Change | -10.7 (3.5)b | -1.6 (1.7)b |
| FTND score | ||
| Before treatment | 6.1 (0.4)a | 6.2 (0.5)a |
| After treatment | 2.5 (0.6)a,b | 4.3 (0.6)a,b |
| Change | -3.6 (0.6)b | -1.9 (0.6)b |
Abbreviations: FTND, Fagerström Test for Nicotine Dependence; SEM, standard error of the mean.
P < .01 within group.
P < .05 between group.
SELF-REPORTED CRAVING
A within-subject repeated-measures analysis of variance revealed a significant 3-way interaction between treatment group (bupropion and placebo), cue condition (crave-allow, crave-resist, neutral), and time (before to after treatment) (F2,24 = 3.60; P = .04) on self-reported craving (scale, 1-5) measured immediately following each cue condition (Figure 1), indicating that bupropion-treated smokers displayed a significantly different craving response pattern to the cue conditions from before to after treatment compared with placebo-treated participants. Significant effects of cue condition (F2,24= 14.88; P < .001), time (F1,25 = 7.66; P = .01), and run (F2,24= 5.86; P = .005) were also observed on self-reported craving, indicating that the smoking-related cues elicited more craving than neutral cues, craving decreased from before to after treatment, and craving increased across runs in all participants.
Figure 1.
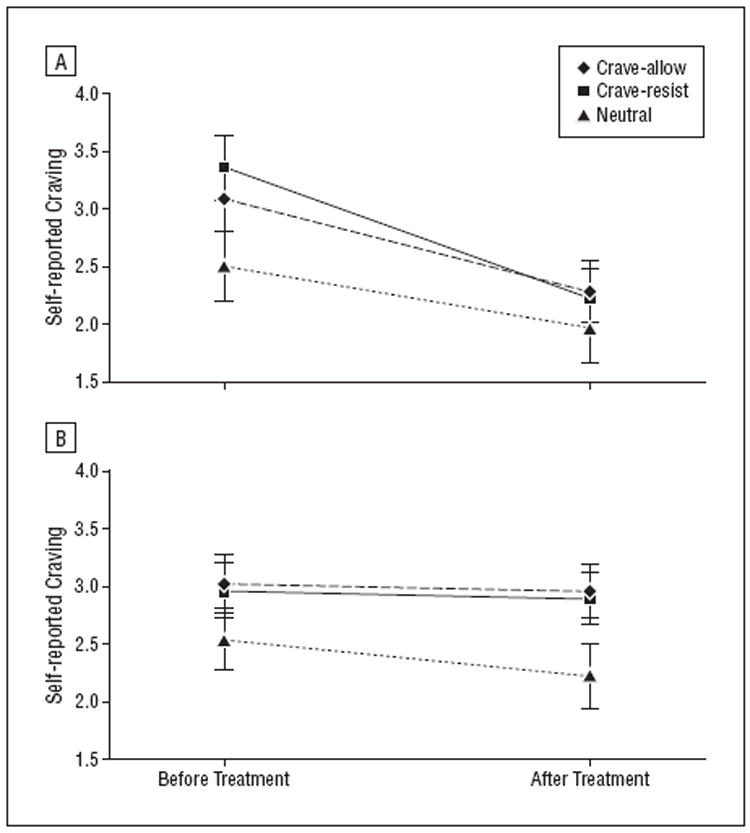
Average self-reported craving (on a scale of 1-5) for each cue condition before and after treatment for patients treated with bupropion (A) or placebo (B).
No significant group differences were observed in craving during any of the cue conditions at baseline (before treatment). An unpaired t test demonstrated that, on average, the bupropion-treated participants reported significantly less craving after treatment (P = .04) and significantly greater reduction in craving from before to after treatment (P = .02) during the crave-resist condition compared with placebo-treated participants. No group differences were observed during the crave-allow or neutral cue conditions before treatment, after treatment, or in the change from before to after treatment (Table 2).
Table 2.
Average Self-reported Craving
| Treatment Condition | Mean (SEM) by Treatment
|
|
|---|---|---|
| Bupropion | Placebo | |
| Crave-resist | ||
| Before treatment | 3.28 (0.17)b | 2.92 (0.28) |
| After treatment | 2.17 (0.25)a,b | 2.93 (0.19)a |
| Change | -1.10 (0.31)a | 0.01 (0.26)a |
| Crave-allow | ||
| Before treatment | 3.03 (0.23) | 3.06 (0.26) |
| After treatment | 2.48 (0.29) | 2.99 (0.24) |
| Change | -0.54 (0.37) | -0.07 (0.26) |
| Neutral | ||
| Before treatment | 2.41 (0.22) | 2.44 (0.31) |
| After treatment | 2.12 (0.30) | 2.21 (0.25) |
| Change | -0.36 (0.32) | -0.23 (0.24) |
Abbreviation: SEM, standard error of the mean.
P < .05 between groups.
P < .05 within group.
fMRI: EFFECTS OF TREATMENT
Between-Group: Before to After Treatment
In the contrast of crave-resist vs neutral from before to after treatment, participants treated with bupropion exhibited significantly greater treatment-induced reductions in activation in the left ventral striatum, right medial orbitofrontal cortex, and bilateral anterior cingulate cortex compared with participants who received placebo (Figure 2; Table 3). No treatment-induced increases in activation were observed in this comparison. The groups showed no difference in activation changes from before to after treatment in comparisons of crave-allow vs neutral or crave-allow vs crave-resist.
Figure 2.
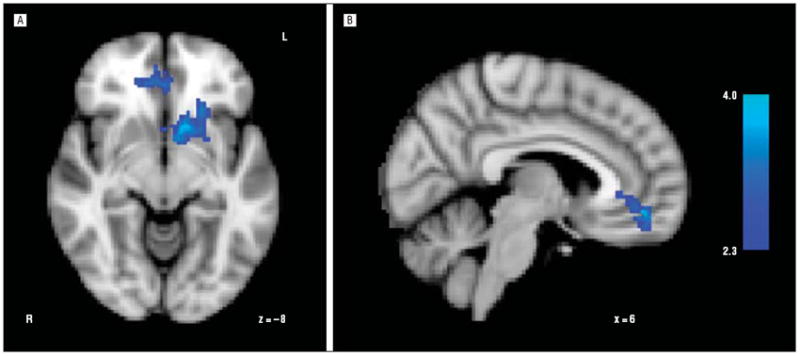
Significant between treatment group differences in change in regional brain activation from before to after treatment during the crave resist vs neutral cue condition. Bupropion-treated participants exhibited significantly greater treatment-induced reductions in activation in the left ventral striatum (A), bilateral anterior cingulate cortex (A and B), and right medial orbitofrontal cortex (B) compared with placebo-treated participants (z threshold >2.3; cluster threshold, P < .05). Z-axis values correspond to MNI152 standard space coordinates.
Table 3.
Local Maxima for Significant Within- and Between-Group Activations
| Region (Contrast) | z Score | x, y, and z Coordinatesa | ||
|---|---|---|---|---|
| Between groups: before to after treatment (bupropion > placebo) | ||||
| Ventral striatum, left | 4.10 | -14, | 14, | -10 |
| 3.65 | -12, | 6, | -12 | |
| Medial orbitofrontal cortex, left | 3.58 | 6, | 46, | -10 |
| Anterior cingulate cortex, bilateral | 3.48 | 0, | 36, | -4 |
| Within bupropion: before to after treatment (pretreatment > posttreatment) | ||||
| Precuneus, bilateral | 3.80 | 2, | -68, | 56 |
| 3.42 | 0, | -76, | 44 | |
| 3.04 | -2, | -64, | 48 | |
| Lateral occipital cortex, bilateral | 3.25 | -12, | -80, | 50 |
| 3.12 | 48, | -74, | 24 | |
| 2.98 | 40, | -78, | 34 | |
| Anterior cingulate cortex, bilateral | 2.91 | 8, | 40, | -8 |
| 2.88 | 2, | 40, | 10 | |
| 2.83 | -4, | 40, | 22 | |
| Between groups: after treatment (placebo > bupropion) | ||||
| Anterior cingulate cortex, left | 3.90 | -4, | 34, | 0 |
| Ventral striatum, left | 3.67 | -18, | 14, | -10 |
| 3.59 | -14, | 14, | -10 | |
| 3.56 | -10, | 14, | -8 | |
Coordinates in MNI152 standard space; x, y, and z refer to right/left (x: positive = right), anterior/posterior (y: positive = anterior), and dorsal/ventral (y: positive = dorsal).
Within-Group: Before to After Treatment
When assessed independently, bupropion-treated participants exhibited significantly reduced activation during the crave-resist vs neutral condition in the bilateral anterior cingulate cortex, precuneus, and lateral occipital cortex from before to after treatment (Figure 3; Table 3). These participants showed no treatment-induced increases in activation in this comparison and no activation changes during comparisons of crave-allow and neutral or crave-allow and crave-resist. The placebo- treated participants showed no significant changes in activation from before to after treatment for any of the cue condition comparisons.
Figure 3.
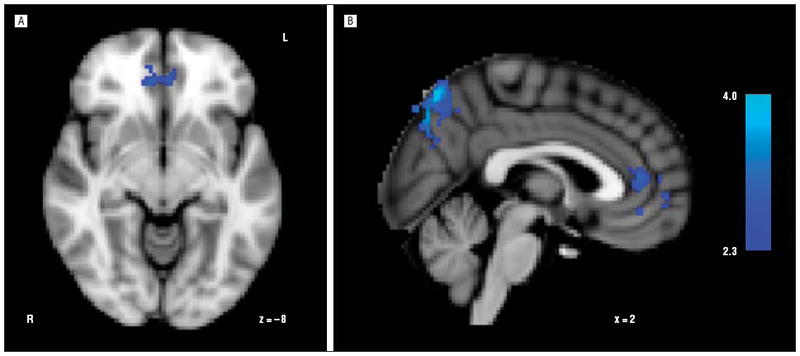
Significant within-treatment group (bupropion-treated) differences in regional brain activation from before to after treatment during the crave-resist vs neutral cue condition. Bupropion-treated participants exhibited significant treatment-induced reductions in activation in the bilateral anterior cingulate (A and B), bilateral precuneus (B), and lateral occipital cortex following treatment (z threshold, >2.3; cluster threshold, P < .05). Z-axis values correspond to MNI152 standard space coordinates.
Between Groups: Before and After Treatment
Prior to treatment, the 2 groups displayed no differences in activation to any of the cue condition comparisons. After treatment, bupropion-treated participants exhibited significantly less activation in the left ventral striatum and left anterior cingulate cortex than placebo-treated participants when comparing crave-resist vs neutral (Figure 4; Table 3). The bupropion-treated participants exhibited no regions of greater activation in this comparison. The groups did not differ significantly following treatment when comparing crave-allow and neutral or crave-allow and crave-resist.
Figure 4.
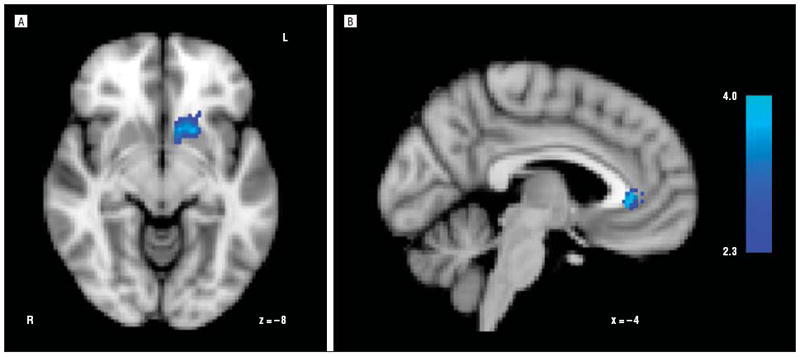
Significant between-treatment group differences in regional brain activation following treatment during the crave-resist vs neutral cue condition. Bupropion-treated participants exhibited significantly less activation in the left ventral striatum (A) and left anterior cingulate cortex (B) compared with placebo-treated participants (z threshold, >2.3; cluster threshold, P < .05). Z-axis values correspond to MNI152 standard space coordinates.
Region-of-Interest Analysis
In regions where significant between-group differences were observed from before to after treatment (Figure 2; Table 3), bupropion-treated participants who reported a reduction in craving following treatment demonstrated a positive correlation between reduction in craving and reduced mean percentage of signal change (r = 0.695; P = .02). This correlation was also observed when placebo-treated participants were included in the analysis (r = 0.488; P = .01), but not when placebo-treated participants were assessed alone. Two bupropion-treated participants were excluded owing to lack of treatment response and 1 was excluded for not completing posttreatment craving responses. (No group differences were observed in brain regions that differed significantly between cue conditions in all participants before treatment.)
fMRI and Self-reported Craving
A positive association was observed between changes in self-reported craving and activation changes from before to after treatment in the bilateral medial orbitofrontal cortex and left anterior cingulate cortex in all participants during the crave-resist vs rest comparison (Figure 5, Table 4). The treatment subgroups did not demonstrate this association when assessed independently. A positive association was also observed in all participants between craving and activation changes in the bilateral precentral gyrus during the crave-allow vs rest comparison. In this same comparison, placebo-treated participants demonstrated a positive association in the right precentral gyrus, postcentral gyrus, precuneus, posterior cingulate cortex, frontal pole, central opercular cortex, inferior frontal gyrus, and transverse temporal gyrus. The bupropion-treated participants demonstrated no association in this comparison (Table 4). In regions where an association was observed between changes in craving and activation during the crave-resist condition (Figure 5, Table 4), bupropion-treated participants exhibited significantly greater reductions in mean percent signal change from before to after treatment (t28 = 2.301; P = .03) compared with placebo-treated participants.
Figure 5.
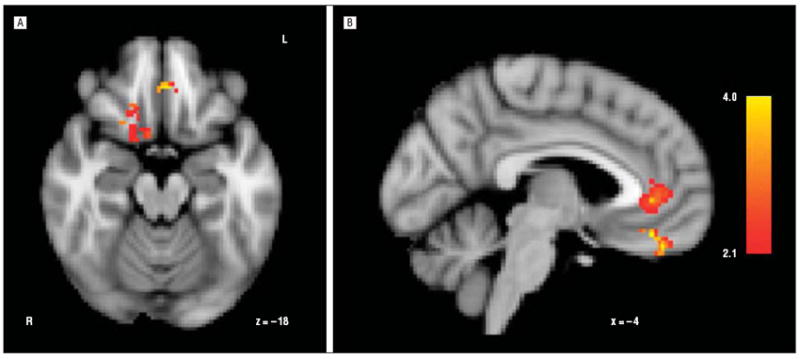
Brain regions correlated between changes in self-reported craving and changes in activation from before to after treatment during the crave-resist vs neutral cue conditions. A significant association was observed between reduction in self-reported craving and reduced activation in the bilateral medial orbitofrontal cortex (A) and left anterior cingulate cortex (B) in all participants (z threshold, >2.1; cluster threshold, P < .05). Z-axis values correspond to MNI152 standard space coordinates.
Table 4.
Local Maxima for Significant Associations Between Reduced Craving and Reduction in Activation From Before to After Treatment
| Cue Condition, Association, and Region | z Score | x, y, z Coordinatesa | ||
|---|---|---|---|---|
| Crave-resist: all subjects | ||||
| Medial orbitofrontal cortex, bilateral | 4.06 | 0, | 38, | -18 |
| 3.87 | -4, | 44, | -24 | |
| 3.86 | -6, | 40, | -22 | |
| Anterior cingulate cortex, left | 3.67 | -8, | 42, | 2 |
| 3.58 | -4, | 38, | 0 | |
| Crave-allow: all subjects | ||||
| Precentral gyrus, bilateral | 3.31 | 2, | -22, | 60 |
| 3.25 | 8, | -30, | 68 | |
| 3.23 | -6, | -14, | 60 | |
| 3.09 | 10, | -22, | 62 | |
| 2.99 | 28, | -26, | 50 | |
| Crave-allow: placebo-treated subjects | ||||
| Precuneus, right | 3.85 | 18, | -54, | 10 |
| 3.65 | 12, | -52, | 12 | |
| 3.10 | 10, | -60, | 46 | |
| 2.85 | 10, | -52, | 40 | |
| Precentral gyrus, bilateral | 3.46 | 8, | -30, | 68 |
| 3.22 | 12, | -26, | 44 | |
| 3.17 | -6, | -14, | 60 | |
| Postcentral gyrus, right | 3.25 | 42, | -32, | 52 |
| 3.21 | 40, | -30, | 58 | |
| 3.24 | 12, | -44, | 70 | |
| Posterior cingulate cortex, right | 3.98 | 8, | -48, | 30 |
| 2.93 | 12, | -42, | 40 | |
| Frontal pole, right | 3.78 | 24, | 68, | 16 |
| 3.72 | 28, | 62, | 12 | |
| 3.30 | 32, | 56, | 10 | |
| 3.18 | 42, | 56, | 10 | |
| 3.08 | 30, | 54, | 22 | |
| Central opercular cortex | 3.36 | 50, | -2, | 2 |
| 3.12 | 48, | 6, | 2 | |
| Inferior frontal gyrus | 3.07 | 62, | 16, | 16 |
| Transverse temporal gyrus | 3.20 | 46, | -24, | 6 |
| Superior temporal gyrus | 3.10 | 62, | -14, | 8 |
Coordinates in MNI152 standard space; x, y, z refer to right/left (x: positive = right), anterior/posterior (y: positive = anterior), dorsal/ventral (y: positive = dorsal).
COMMENT
Nicotine-dependent smokers treated with bupropion report significantly greater reductions in craving and exhibited reduced activation in the ventral striatum, medial orbitofrontal cortex, and anterior cingulate cortex when resisting craving compared with smokers treated with placebo. When assessing these specific regions, activation changes correlated positively with changes in craving from before to after treatment. The bupropion-treated group alone exhibited reduced activation in the anterior cingulate cortex and in secondary visual processing centers while resisting craving. While no craving or activation differences were observed between treatment groups before treatment, bupropion-treated participants reported significantly less craving and exhibited less ventral striatum and anterior cingulate cortex activation than placebo-treated participants when resisting craving after treatment. These results demonstrate that treatment with bupropion is associated with an improved ability to resist cue-induced craving and a reduction in cue-induced activation of limbic and prefrontal brain regions.
Our findings complement previous research demonstrating that nicotine-dependent smokers exhibit activation in the anterior cingulate cortex and ventral striatum as well as other brain regions that integrate information regarding executive function (prefrontal cortex), prior experience (hippocampus), emotion (amygdala), and reward (ventral tegmental area) while viewing smoking-related cues.40-45 Bupropion treatment attenuates cue-induced metabolism in the anterior cingulate cortex58 and, as demonstrated here, cue-induced activation of this region and other brain regions (ventral striatum and medial orbitofrontal cortex) known to be involved in drug craving and addiction.81,82 Activation changes in these brain regions correlated with a reduction in craving, suggesting that modulation of limbic and prefrontal function associated with bupropion treatment may directly influence subjective craving.
The association between craving and brain activation observed during the crave-resist condition, irrespective of treatment, parallels previous research demonstrating a relationship between drug craving and activation of brain regions that are responsible for emotional and cognitive appraisal (anterior cingulate cortex) and conditioned reinforcement (medial orbitofrontal cortex).40,70,82 Bupropion-treated participants exhibited reduced activation in these specific regions while resisting craving compared with placebo-treated participants. These findings further support the role of prefrontal regions in mediating cue-induced craving and support the primary finding of this study that bupropion treatment modulates activation in the anterior cingulate and medial orbitofrontal cortices.
Bupropion is reported to enhance smoking cessation by altering basal levels of dopamine though inhibition of dopamine reuptake while simultaneously modulating phasic dopamine release in the ventral striatum in response to smoking or smoking-related cues.9,16,17,21,33,83-85 Although fMRI data remain difficult to interpret in the context of specific neurotransmitters, our results demonstrate that bupropion treatment induced changes in the dopamine-rich ventral striatum and functionally related anterior cingulate cortex86 and medial orbitofrontal cortex. The anterior cingulate cortex collects information from limbic and prefrontal regions to assess the salience of emotional and motivational information, while the ventral striatum works in concert to mediate reward, particularly for drugs,87,88 as well as predict and act on the presence of reward.25,89 Research combining positron emission tomography and fMRI imaging has verified this functional association and revealed a positive correlation between dopamine synthesis capacity in the ventral striatum and blood oxygen level–dependent signal increases in the anterior cingulate cortex elicited by rewarding stimuli.90 Hence, modulation of dopamine signaling in the ventral striatum via bupropion may alter reward signaling to the anterior cingulate cortex and associated prefrontal regions, attenuating affective appraisal of smoking cues and relative reward salience, thereby leading to a reduction in craving.
Although no treatment-induced changes were seen in regions previously shown to differ when untreated smokers allow or resist craving,70 the associations between craving and brain activation observed under these 2 conditions varied considerably. During the crave-allow condition, placebo-treated participants exhibited an association between changes in craving and activation in default mode networks (posterior cingulate cortex, precuneus)91 and brain regions associated with imitation (frontal lobe, premotor cortex, superior parietal lobe, inferior frontal cortex92). This finding suggests that placebo- treated participants who reported less craving during the crave-allow condition were less engaged by the smoking-related cues. This effect was not observed in the bupropion-treated smokers or the combined sample (both treatment groups). Considering these findings, instructing smokers to allow cue-induced craving elicits brain activation associated with mentally mimicking or imagining smoking behavior while encouraging them to resisting craving influences brain regions that relate to conditioned reward and affective appraisal, providing amore relevant state for assessing smoking cessation therapies.
While published articles demonstrate roughly 35% to 40% short-term abstinence rates with bupropion treatment,3,4 we expected a quit rate of approximately 20% in our bupropion-treated smokers because we did not provide concomitant behavioral intervention along with the medication administration as in prior studies. We did not include behavioral intervention in order to isolate the effects of bupropion treatment on regional brain activation. Although the bupropion-treated participants exhibited significantly greater reductions in FTND scores and exhaled carbon monoxide from before to after treatment and lower FTND scores after treatment (Table 1), no significant between-group difference was observed in cigarettes per day (though bupropion- treated smokers did, on average, have a greater reduction in this measure). The discrepancies between objective (exhaled carbon monoxide) and self-reported (cigarettes per day) smoking measures reported in placebo- treated smokers may reflect the desire of research participants to please study researchers. In addition to controlling for nicotine consumption in our primary analysis, we also replicated the primary finding of this study, excluding participants who quit smoking during treatment (bupropion, n = 3; placebo, n = 1) to ensure that the unbalanced number of quitters in each group did not unintentionally influence our findings (eFigure; http://www.archgenpsychiatry.com).
In summary, a standard course of treatment with bupropion enhances the ability of smokers to resist cueinduced craving, measured as reductions in self-reported craving and reduced activation in the ventral striatum, anterior cingulate, and medial orbitofrontal cortex.
Acknowledgments
Funding/Support: This study was supported by grants R01 DA20872 (Dr Brody) and DA245482 (Mr Culbertson) from the National Institute on Drug Abuse; grant 16RT-0098 from the Tobacco-Related Disease Research Program, a Veterans Affairs Type I Merit Review Award, and endowments from the Richard Metzner Chair in Clinical Neuropharmacology (Dr Brody); and endowments from the Thomas P. and Katherine K. Pike Chair in Addiction Studies and the Marjorie M. Greene Trust (Dr London).
Footnotes
Author Contributions: Drs Culbertson, Brody, Bramen, and Cohen had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors contributed substantially to the scientific process leading to the writing of the manuscript.
Financial Disclosure: None reported.
Online-Only Material: The eFigure is available at http://www.archgenpsychiatry.com.
References
- 1.Raw M, Regan S, Rigotti NA, McNeill A. A survey of tobacco dependence treatment guidelines in 31 countries. Addiction. 2009;104(7):1243–1250. doi: 10.1111/j.1360-0443.2009.02584.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Holmes S, Zwar N, Jiménez-Ruiz CA, Ryan PJ, Browning D, Bergmann L, Johnston JA. Bupropion as an aid to smoking cessation: a review of real-life effectiveness. Int J Clin Pract. 2004;58(3):285–291. doi: 10.1111/j.1368-5031.2004.00153.x. [DOI] [PubMed] [Google Scholar]
- 3.Hurt RD, Sachs DP, Glover ED, Offord KP, Johnston JA, Dale LC, Khayrallah MA, Schroeder DR, Glover PN, Sullivan CR, Croghan IT, Sullivan PM. A comparison of sustained-release bupropion and placebo for smoking cessation. N Engl J Med. 1997;337(17):1195–1202. doi: 10.1056/NEJM199710233371703. [DOI] [PubMed] [Google Scholar]
- 4.Jorenby DE, Leischow SJ, Nides MA, Rennard SI, Johnston JA, Hughes AR, Smith SS, Muramoto ML, Daughton DM, Doan K, Fiore MC, Baker TB. A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N Engl J Med. 1999;340(9):685–691. doi: 10.1056/NEJM199903043400903. [DOI] [PubMed] [Google Scholar]
- 5.Hays JT, Hurt RD, Rigotti NA, Niaura R, Gonzales D, Durcan MJ, Sachs DP, Wolter TD, Buist AS, Johnston JA, White JD. Sustained-release bupropion for pharmacologic relapse prevention after smoking cessation: a randomized, controlled trial. Ann Intern Med. 2001;135(6):423–433. doi: 10.7326/0003-4819-135-6-200109180-00011. [DOI] [PubMed] [Google Scholar]
- 6.Durcan MJ, Deener G, White J, Johnston JA, Gonzales D, Niaura R, Rigotti N, Sachs DP. The effect of bupropion sustained-release on cigarette craving after smoking cessation. Clin Ther. 2002;24(4):540–551. doi: 10.1016/s0149-2918(02)85130-x. [DOI] [PubMed] [Google Scholar]
- 7.Paluck EC, McCormack JP, Ensom MH, Levine M, Soon JA, Fielding DW. Outcomes of bupropion therapy for smoking cessation during routine clinical use. Ann Pharmacother. 2006;40(2):185–190. doi: 10.1345/aph.1G324. [DOI] [PubMed] [Google Scholar]
- 8.Simon JA, Duncan C, Carmody TP, Hudes ES. Bupropion for smoking cessation: a randomized trial. Arch Intern Med. 2004;164(16):1797–1803. doi: 10.1001/archinte.164.16.1797. [DOI] [PubMed] [Google Scholar]
- 9.Shiffman S, Johnston JA, Khayrallah M, Elash CA, Gwaltney CJ, Paty JA, Gnys M, Evoniuk G, DeVeaugh-Geiss J. The effect of bupropion on nicotine craving and withdrawal. Psychopharmacology (Berl) 2000;148(1):33–40. doi: 10.1007/s002130050022. [DOI] [PubMed] [Google Scholar]
- 10.Strong DR, Kahler CW, Leventhal AM, Abrantes AM, Lloyd-Richardson E, Niaura R, Brown RA. Impact of bupropion and cognitive-behavioral treatment for depression on positive affect, negative affect, and urges to smoke during cessation treatment. Nicotine Tob Res. 2009;11(10):1142–1153. doi: 10.1093/ntr/ntp111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ahluwalia JS, Harris KJ, Catley D, Okuyemi KS, Mayo MS. Sustained-release bupropion for smoking cessation in African Americans: a randomized controlled trial. JAMA. 2002;288(4):468–474. doi: 10.1001/jama.288.4.468. [DOI] [PubMed] [Google Scholar]
- 12.Aubin HJ, Lebargy F, Berlin I, Bidaut-Mazel C, Chemali-Hudry J, Lagrue G. Efficacy of bupropion and predictors of successful outcome in a sample of French smokers: a randomized placebo-controlled trial. Addiction. 2004;99(9):1206–1218. doi: 10.1111/j.1360-0443.2004.00814.x. [DOI] [PubMed] [Google Scholar]
- 13.Killen JD, Robinson TN, Ammerman S, Hayward C, Rogers J, Stone C, Samuels D, Levin SK, Green S, Schatzberg AF. Randomized clinical trial of the efficacy of bupropion combined with nicotine patch in the treatment of adolescent smokers. J Consult Clin Psychol. 2004;72(4):729–735. doi: 10.1037/0022-006X.72.4.729. [DOI] [PubMed] [Google Scholar]
- 14.Swan GE, McAfee T, Curry SJ, Jack LM, Javitz H, Dacey S, Bergman K. Effectiveness of bupropion sustained release for smoking cessation in a health care setting: a randomized trial. Arch Intern Med. 2003;163(19):2337–2344. doi: 10.1001/archinte.163.19.2337. [DOI] [PubMed] [Google Scholar]
- 15.Tønnesen P, Tonstad S, Hjalmarson A, Lebargy F, Van Spiegel PI, Hider A, Sweet R, Townsend J. A multicentre, randomized, double-blind, placebo-controlled, 1-year study of bupropion SR for smoking cessation. J Intern Med. 2003;254(2):184–192. doi: 10.1046/j.1365-2796.2003.01185.x. [DOI] [PubMed] [Google Scholar]
- 16.Ascher JA, Cole JO, Colin JN, Feighner JP, Ferris RM, Fibiger HC, Golden RN, Martin P, Potter WZ, Richelson E, et al. Bupropion: a review of its mechanism of antidepressant activity. J Clin Psychiatry. 1995;56(9):395–401. [PubMed] [Google Scholar]
- 17.Balfour DJ. The pharmacology underlying pharmacotherapy for tobacco dependence: a focus on bupropion. Int J Clin Pract. 2001;55(1):53–57. [PubMed] [Google Scholar]
- 18.Bondarev ML, Bondareva TS, Young R, Glennon RA. Behavioral and biochemical investigations of bupropion metabolites. Eur J Pharmacol. 2003;474(1):85–93. doi: 10.1016/s0014-2999(03)02010-7. [DOI] [PubMed] [Google Scholar]
- 19.Cooper BR, Wang CM, Cox RF, Norton R, Shea V, Ferris RM. Evidence that the acute behavioral and electrophysiological effects of bupropion (Wellbutrin) are mediated by a noradrenergic mechanism. Neuropsychopharmacology. 1994;11(2):133–141. doi: 10.1038/npp.1994.43. [DOI] [PubMed] [Google Scholar]
- 20.Damaj MI, Carroll FI, Eaton JB, Navarro HA, Blough BE, Mirza S, Lukas RJ, Martin BR. Enantioselective effects of hydroxy metabolites of bupropion on behavior and on function of monoamine transporters and nicotinic receptors. Mol Pharmacol. 2004;66(3):675–682. doi: 10.1124/mol.104.001313. [DOI] [PubMed] [Google Scholar]
- 21.Foley KF, DeSanty KP, Kast RE. Bupropion: pharmacology and therapeutic applications. Expert Rev Neurother. 2006;6(9):1249–1265. doi: 10.1586/14737175.6.9.1249. [DOI] [PubMed] [Google Scholar]
- 22.Nomikos GG, Damsma G, Wenkstern D, Fibiger HC. Acute effects of bupropion on extracellular dopamine concentrations in rat striatum and nucleus accumbens studied by in vivo microdialysis. Neuropsychopharmacology. 1989;2(4):273–279. doi: 10.1016/0893-133x(89)90031-6. [DOI] [PubMed] [Google Scholar]
- 23.Stahl SM, Pradko JF, Haight BR, Modell JG, Rockett CB, Learned-Coughlin S. A review of the neuropharmacology of bupropion, a dual norepinephrine and dopamine reuptake inhibitor. Prim Care Companion J Clin Psychiatry. 2004;6(4):159–166. doi: 10.4088/pcc.v06n0403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Learned-Coughlin SM, Bergström M, Savitcheva I, Ascher J, Schmith VD, Långstrom B. In vivo activity of bupropion at the human dopamine transporter as measured by positron emission tomography. Biol Psychiatry. 2003;54(8):800–805. doi: 10.1016/s0006-3223(02)01834-6. [DOI] [PubMed] [Google Scholar]
- 25.Mansvelder HD, Mertz M, Role LW. Nicotinic modulation of synaptic transmission and plasticity in cortico-limbic circuits. Semin Cell Dev Biol. 2009;20(4):432–440. doi: 10.1016/j.semcdb.2009.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Markou A. Neurobiology of nicotine dependence. Philos Trans R Soc Lond B Biol Sci. 2008;363(1507):3159–3168. doi: 10.1098/rstb.2008.0095. review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Alkondon M, Albuquerque EX. Nicotinic receptor subtypes in rat hippocampal slices are differentially sensitive to desensitization and early in vivo functional up-regulation by nicotine and to block by bupropion. J Pharmacol Exp Ther. 2005;313(2):740–750. doi: 10.1124/jpet.104.081232. [DOI] [PubMed] [Google Scholar]
- 28.Arias HR. Is the inhibition of nicotinic acetylcholine receptors by bupropion involved in its clinical actions? Int J Biochem Cell Biol. 2009;41(11):2098–2108. doi: 10.1016/j.biocel.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 29.Dwoskin LP, Smith AM, Wooters TE, Zhang Z, Crooks PA, Bardo MT. Nicotinic receptor-based therapeutics and candidates for smoking cessation. Biochem Pharmacol. 2009;78(7):732–743. doi: 10.1016/j.bcp.2009.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Fryer JD, Lukas RJ. Noncompetitive functional inhibition at diverse, human nicotinic acetylcholine receptor subtypes by bupropion, phencyclidine, and ibogaine. J Pharmacol Exp Ther. 1999;288(1):88–92. [PubMed] [Google Scholar]
- 31.Slemmer JE, Martin BR, Damaj MI. Bupropion is a nicotinic antagonist. J Pharmacol Exp Ther. 2000;295(1):321–327. [PubMed] [Google Scholar]
- 32.Mansvelder HD, Fagen ZM, Chang B, Mitchum R, McGehee DS. Bupropion inhibits the cellular effects of nicotine in the ventral tegmental area. Biochem Pharmacol. 2007;74(8):1283–1291. doi: 10.1016/j.bcp.2007.07.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Warner C, Shoaib M. How does bupropion work as a smoking cessation aid? Addict Biol. 2005;10(3):219–231. doi: 10.1080/13556210500222670. [DOI] [PubMed] [Google Scholar]
- 34.Chiamulera C, Borgo C, Falchetto S, Valerio E, Tessari M. Nicotine reinstatement of nicotine self-administration after long-term extinction. Psychopharmacology (Berl) 1996;127(2):102–107. doi: 10.1007/BF02805981. [DOI] [PubMed] [Google Scholar]
- 35.Rose JE, Behm FM. Extinguishing the rewarding value of smoke cues: pharmacological and behavioral treatments. Nicotine Tob Res. 2004;6(3):523–532. doi: 10.1080/14622200410001696501. [DOI] [PubMed] [Google Scholar]
- 36.Rose JE, Behm FM, Westman EC, Kukovich P. Precessation treatment with nicotine skin patch facilitates smoking cessation. Nicotine Tob Res. 2006;8(1):89–101. doi: 10.1080/14622200500431866. [DOI] [PubMed] [Google Scholar]
- 37.Abrams DB, Monti PM, Carey KB, Pinto RP, Jacobus SI. Reactivity to smoking cues and relapse: two studies of discriminant validity. Behav Res Ther. 1988;26(3):225–233. doi: 10.1016/0005-7967(88)90003-4. [DOI] [PubMed] [Google Scholar]
- 38.Caggiula AR, Donny EC, White AR, Chaudhri N, Booth S, Gharib MA, Hoffman A, Perkins KA, Sved AF. Cue dependency of nicotine self-administration and smoking. Pharmacol Biochem Behav. 2001;70(4):515–530. doi: 10.1016/s0091-3057(01)00676-1. [DOI] [PubMed] [Google Scholar]
- 39.Caggiula AR, Donny EC, Palmatier MI, Liu X, Chaudhri N, Sved AF. The role of nicotine in smoking: a dual-reinforcement model. Nebr Symp Motiv. 2009;55:91–109. doi: 10.1007/978-0-387-78748-0_6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Brody AL, Mandelkern MA, London ED, Childress AR, Lee GS, Bota RG, Ho ML, Saxena S, Baxter LR, Jr, Madsen D, Jarvik ME. Brain metabolic changes during cigarette craving. Arch Gen Psychiatry. 2002;59(12):1162–1172. doi: 10.1001/archpsyc.59.12.1162. [DOI] [PubMed] [Google Scholar]
- 41.Due DL, Huettel SA, Hall WG, Rubin DC. Activation in mesolimbic and visuospatial neural circuits elicited by smoking cues: evidence from functional magnetic resonance imaging. Am J Psychiatry. 2002;159(6):954–960. doi: 10.1176/appi.ajp.159.6.954. [DOI] [PubMed] [Google Scholar]
- 42.Lee JH, Lim Y, Wiederhold BK, Graham SJ. A functional magnetic resonance imaging (FMRI) study of cue-induced smoking craving in virtual environments. Appl Psychophysiol Biofeedback. 2005;30(3):195–204. doi: 10.1007/s10484-005-6377-z. [DOI] [PubMed] [Google Scholar]
- 43.Wang Z, Faith M, Patterson F, Tang K, Kerrin K, Wileyto EP, Detre JA, Lerman C. Neural substrates of abstinence-induced cigarette cravings in chronic smokers. J Neurosci. 2007;27(51):14035–14040. doi: 10.1523/JNEUROSCI.2966-07.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.David SP, Munafò MR, Johansen-Berg H, Smith SM, Rogers RD, Matthews PM, Walton RT. Ventral striatum/nucleus accumbens activation to smoking-related pictorial cues in smokers and nonsmokers: a functional magnetic resonance imaging study. Biol Psychiatry. 2005;58(6):488–494. doi: 10.1016/j.biopsych.2005.04.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Franklin TR, Wang Z, Wang J, Sciortino N, Harper D, Li Y, Ehrman R, Kampman K, O’Brien CP, Detre JA, Childress AR. Limbic activation to cigarette smoking cues independent of nicotine withdrawal: a perfusion fMRI study. Neuropsychopharmacology. 2007;32(11):2301–2309. doi: 10.1038/sj.npp.1301371. [DOI] [PubMed] [Google Scholar]
- 46.McClernon FJ, Kozink RV, Rose JE. Individual differences in nicotine dependence, withdrawal symptoms, and sex predict transient fMRI-BOLD responses to smoking cues. Neuropsychopharmacology. 2008;33(9):2148–2157. doi: 10.1038/sj.npp.1301618. [DOI] [PubMed] [Google Scholar]
- 47.Smolka MN, Bühler M, Klein S, Zimmermann U, Mann K, Heinz A, Braus DF. Severity of nicotine dependence modulates cue-induced brain activity in regions involved in motor preparation and imagery. Psychopharmacology (Berl) 2006;184(3-4):577–588. doi: 10.1007/s00213-005-0080-x. [DOI] [PubMed] [Google Scholar]
- 48.Yalachkov Y, Kaiser J, Naumer MJ. Brain regions related to tool use and action knowledge reflect nicotine dependence. J Neurosci. 2009;29(15):4922–4929. doi: 10.1523/JNEUROSCI.4891-08.2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Gloria R, Angelos L, Schaefer HS, Davis JM, Majeskie M, Richmond BS, Curtin JJ, Davidson RJ, Baker TB. An fMRI investigation of the impact of withdrawal on regional brain activity during nicotine anticipation. Psychophysiology. 2009;46(4):681–693. doi: 10.1111/j.1469-8986.2009.00823.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.McClernon FJ, Hiott FB, Huettel SA, Rose JE. Abstinence-induced changes in self-report craving correlate with event-related FMRI responses to smoking cues. Neuropsychopharmacology. 2005;30(10):1940–1947. doi: 10.1038/sj.npp.1300780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.McClernon FJ, Kozink RV, Lutz AM, Rose JE. 24-h smoking abstinence potentiates fMRI-BOLD activation to smoking cues in cerebral cortex and dorsal striatum. Psychopharmacology (Berl) 2009;204(1):25–35. doi: 10.1007/s00213-008-1436-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.McBride D, Barrett SP, Kelly JT, Aw A, Dagher A. Effects of expectancy and abstinence on the neural response to smoking cues in cigarette smokers: an fMRI study. Neuropsychopharmacology. 2006;31(12):2728–2738. doi: 10.1038/sj.npp.1301075. [DOI] [PubMed] [Google Scholar]
- 53.Wilson SJ, Sayette MA, Delgado MR, Fiez JA. Instructed smoking expectancy modulates cue-elicited neural activity: a preliminary study. Nicotine Tob Res. 2005;7(4):637–645. doi: 10.1080/14622200500185520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Franklin TR, Lohoff FW, Wang Z, Sciortino N, Harper D, Li Y, Jens W, Cruz J, Kampman K, Ehrman R, Berrettini W, Detre JA, O’Brien CP, Childress AR. DAT genotype modulates brain and behavioral responses elicited by cigarette cues. Neuropsychopharmacology. 2009;34(3):717–728. doi: 10.1038/npp.2008.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Azizian A, Monterosso J, O’Neill J, London ED. Magnetic resonance imaging studies of cigarette smoking. Handb Exp Pharmacol. 2009;(192):113–143. doi: 10.1007/978-3-540-69248-5_5. [DOI] [PubMed] [Google Scholar]
- 56.Le Foll B, Goldberg SR. Nicotine as a typical drug of abuse in experimental animals and humans. Psychopharmacology (Berl) 2006;184(3-4):367–381. doi: 10.1007/s00213-005-0155-8. [DOI] [PubMed] [Google Scholar]
- 57.Shoaib M, Sidhpura N, Shafait S. Investigating the actions of bupropion on dependence- related effects of nicotine in rats. Psychopharmacology (Berl) 2003;165(4):405–412. doi: 10.1007/s00213-002-1277-x. [DOI] [PubMed] [Google Scholar]
- 58.Brody AL, Mandelkern MA, Lee G, Smith E, Sadeghi M, Saxena S, Jarvik ME, London ED. Attenuation of cue-induced cigarette craving and anterior cingulate cortex activation in bupropion-treated smokers: a preliminary study. Psychiatry Res. 2004;130(3):269–281. doi: 10.1016/j.pscychresns.2003.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Costello MR, Mandelkern MA, Shoptaw S, et al. Effects of treatment for tobacco dependence on resting cerebral glucose metabolism. Neuropsychopharmacology. 2009;35(3):605–612. doi: 10.1038/npp.2009.165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Weinstein A, Greif J, Yemini Z, Lerman H, Weizman A, Even-Sapir E. Attenuation of cue-induced smoking urges and brain reward activity in smokers treated successfully with bupropion. J Psychopharmacol. doi: 10.1177/0269881109105456. published online July 31, 2009. [DOI] [PubMed] [Google Scholar]
- 61.First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Edition (SCID-I/P, version 2.0) New York, NY: New York State Psychiatric Institute; 1995. [Google Scholar]
- 62.Fagerström KO. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict Behav. 1978;3(3-4):235–241. doi: 10.1016/0306-4603(78)90024-2. [DOI] [PubMed] [Google Scholar]
- 63.Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for nicotine dependence: a revision of the Fagerström tolerance questionnaire. Br J Addict. 1991;86(9):1119–1127. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 64.Jarvik ME, Madsen DC, Olmstead RE, Iwamoto-Schaap PN, Elins JL, Benowitz NL. Nicotine blood levels and subjective craving for cigarettes. Pharmacol Biochem Behav. 2000;66(3):553–558. doi: 10.1016/s0091-3057(00)00261-6. [DOI] [PubMed] [Google Scholar]
- 65.Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. 1967;6(4):278–296. doi: 10.1111/j.2044-8260.1967.tb00530.x. [DOI] [PubMed] [Google Scholar]
- 66.Snaith RP, Bridge GW, Hamilton M. The Leeds scales for the self-assessment of anxiety and depression. Br J Psychiatry. 1976;128:156–165. doi: 10.1192/bjp.128.2.156. [DOI] [PubMed] [Google Scholar]
- 67.Marrone GF, Paulpillai M, Evans RJ, Singleton EG, Heishman SJ. Breath carbon monoxide and semiquantitative saliva cotinine as biomarkers for smoking. Hum Psychopharmacol. 2010;25(1):80–83. doi: 10.1002/hup.1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Wald NJ, Idle M, Boreham J, Bailey A. Carbon monoxide in breath in relation to smoking and carboxyhaemoglobin levels. Thorax. 1981;36(5):366–369. doi: 10.1136/thx.36.5.366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Schuh KJ, Stitzer ML. Desire to smoke during spaced smoking intervals. Psychopharmacology (Berl) 1995;120(3):289–295. doi: 10.1007/BF02311176. [DOI] [PubMed] [Google Scholar]
- 70.Brody AL, Mandelkern MA, Olmstead RE, Jou J, Tiongson E, Allen V, Scheibal D, London ED, Monterosso JR, Tiffany ST, Korb A, Gan JJ, Cohen MS. Neural substrates of resisting craving during cigarette cue exposure. Biol Psychiatry. 2007;62(6):642–651. doi: 10.1016/j.biopsych.2006.10.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Conklin CA, Tiffany ST. The impact of imagining personalized versus standardized urge scenarios on cigarette craving and autonomic reactivity. Exp Clin Psychopharmacol. 2001;9(4):399–408. doi: 10.1037//1064-1297.9.4.399. [DOI] [PubMed] [Google Scholar]
- 72.Rosenberg H. Clinical and laboratory assessment of the subjective experience of drug craving. Clin Psychol Rev. 2009;29(6):519–534. doi: 10.1016/j.cpr.2009.06.002. [DOI] [PubMed] [Google Scholar]
- 73.Jenkinson M, Smith S. A global optimisation method for robust affine registration of brain images. Med Image Anal. 2001;5(2):143–156. doi: 10.1016/s1361-8415(01)00036-6. [DOI] [PubMed] [Google Scholar]
- 74.Smith SM. Fast robust automated brain extraction. Hum Brain Mapp. 2002;7(3):143–155. doi: 10.1002/hbm.10062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Woolrich MW, Ripley BD, Brady M, Smith SM. Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimage. 2001;14(6):1370–1386. doi: 10.1006/nimg.2001.0931. [DOI] [PubMed] [Google Scholar]
- 76.Jenkinson M, Bannister P, Brady M, Smith S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage. 2002;17(2):825–841. doi: 10.1016/s1053-8119(02)91132-8. [DOI] [PubMed] [Google Scholar]
- 77.Beckmann CF, Jenkinson M, Smith SM. General multilevel linear modeling for group analysis in FMRI. Neuroimage. 2003;20(2):1052–1063. doi: 10.1016/S1053-8119(03)00435-X. [DOI] [PubMed] [Google Scholar]
- 78.Woolrich MW, Behrens TE, Beckmann CF, Jenkinson M, Smith SM. Multilevel linear modelling for FMRI group analysis using Bayesian inference. Neuroimage. 2004;21(4):1732–1747. doi: 10.1016/j.neuroimage.2003.12.023. [DOI] [PubMed] [Google Scholar]
- 79.Woolrich MW, Jbabdi S, Patenaude B, Chappell M, Makni S, Behrens T, Beckmann C, Jenkinson M, Smith SM. Bayesian analysis of neuroimaging data in FSL. Neuroimage. 2009;45(1 suppl):S173–S186. doi: 10.1016/j.neuroimage.2008.10.055. [DOI] [PubMed] [Google Scholar]
- 80.Worsley KJ, Evans AC, Marrett S, Neelin P. A three-dimensional statistical analysis for CBF activation studies in human brain. J Cereb Blood Flow Metab. 1992;12(6):900–918. doi: 10.1038/jcbfm.1992.127. [DOI] [PubMed] [Google Scholar]
- 81.Everitt BJ, Robbins TW. Neural systems of reinforcement for drug addiction: from actions to habits to compulsion. Nat Neurosci. 2005;8(11):1481–1489. doi: 10.1038/nn1579. [DOI] [PubMed] [Google Scholar]
- 82.Everitt BJ, Hutcheson DM, Ersche KD, Pelloux Y, Dalley JW, Robbins TW. The orbital prefrontal cortex and drug addiction in laboratory animals and humans. Ann N Y Acad Sci. 2007;1121:576–597. doi: 10.1196/annals.1401.022. [DOI] [PubMed] [Google Scholar]
- 83.Ferguson SG, Shiffman S. The relevance and treatment of cue-induced cravings in tobacco dependence. J Subst Abuse Treat. 2009;36(3):235–243. doi: 10.1016/j.jsat.2008.06.005. [DOI] [PubMed] [Google Scholar]
- 84.Holm KJ, Spencer CM. Bupropion: a review of its use in the management of smoking cessation. Drugs. 2000;59(4):1007–1024. doi: 10.2165/00003495-200059040-00019. [DOI] [PubMed] [Google Scholar]
- 85.Hughes J, Stead L, Lancaster T. Antidepressants for smoking cessation. Cochrane Database Syst Rev. 2004;(4) doi: 10.1002/14651858.CD000031.pub2. CD000031. [DOI] [PubMed] [Google Scholar]
- 86.Bush G, Luu P, Posner MI. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci. 2000;4(6):215–222. doi: 10.1016/s1364-6613(00)01483-2. [DOI] [PubMed] [Google Scholar]
- 87.Everitt BJ, Robbins TW. Second-order schedules of drug reinforcement in rats andmonkeys: measurement of reinforcing efficacy and drug-seeking behaviour. Psychopharmacology (Berl) 2000;153(1):17–30. doi: 10.1007/s002130000566. [DOI] [PubMed] [Google Scholar]
- 88.Phillips PE, Stuber GD, Heien ML, Wightman RM, Carelli RM. Subsecond dopamine release promotes cocaine seeking. Nature. 2003;422(6932):614–618. doi: 10.1038/nature01476. [DOI] [PubMed] [Google Scholar]
- 89.Schultz W. Predictive reward signal of dopamine neurons. J Neurophysiol. 1998;80(1):1–27. doi: 10.1152/jn.1998.80.1.1. [DOI] [PubMed] [Google Scholar]
- 90.Siessmeier T, Kienast T, Wrase J, Larsen JL, Braus DF, Smolka MN, Buchholz HG, Schreckenberger M, Rösch F, Cumming P, Mann K, Bartenstein P, Heinz A. Net influx of plasma 6-[18F]fluoro-L-DOPA (FDOPA) to the ventral striatum correlates with prefrontal processing of affective stimuli. Eur J Neurosci. 2006;24(1):305–313. doi: 10.1111/j.1460-9568.2006.04903.x. [DOI] [PubMed] [Google Scholar]
- 91.Fransson P, Marrelec G. The precuneus/posterior cingulate cortex plays a pivotal role in the default mode network: Evidence from a partial correlation network analysis. Neuroimage. 2008;42(3):1178–1184. doi: 10.1016/j.neuroimage.2008.05.059. [DOI] [PubMed] [Google Scholar]
- 92.Molenberghs P, Cunnington R, Mattingley JB. Is the mirror neuron system involved in imitation? a short review and meta-analysis. Neurosci Biobehav Rev. 2009;33(7):975–980. doi: 10.1016/j.neubiorev.2009.03.010. [DOI] [PubMed] [Google Scholar]