

Abstract
Free-end saddles are liable to be displaced under occlusal pressure. This is as a result of the displaceability of the mucosa. The altered cast technique is employed to try and prevent this by making an impression of the mucosa under controlled pressure. The metal framework was constructed on a cast produced by a mucostatic impression material. Base plates were then constructed in self-cured acrylics on the framework in the saddle areas, and these are close fitting. Border molding was carried out; impression was made with zinc oxide eugenol impression paste.
In the laboratory, the free-end saddle areas on the master cast are sectioned off. The denture is then positioned on the model and the new saddle areas are poured. The resulting model represents the free-end saddle areas under conditions, which mimic functional load. Denture construction then continues as normal. The distribution of loading of the free-end saddles is improved and denture is more stable.
Keywords: Free end saddles, altered cast technique, stable denture
Introduction
The most important consideration in designing a free-end saddles/distal extension removable partial denture, or CPD, for optimum function is as DeVan stated “the perpetual preservation of that which remains, and not the meticulous replacement of that which has been lost.”
Cast partial denture made using the altered cast impression technique helps create an environment in which the teeth and the edentulous tissues support the base as compatibly as possible. The result is a potentially more stable RPD that improves the support for the occlusal relationship of the opposing dentition and the RPD restoration.[1] The partially edentulous mouth may respond well to any number of treatment modalities and philosophies.
However, this technique has the potential benefits of reducing the number of postoperative visits, preserving the residual ridges, improving stress distribution, decreasing food impaction and decreasing the torquing of abutment teeth. All of which lead to increased patient satisfaction.[2]
Becker and colleagues critically reviewed the evolution of RPD and outlined six principles of RPD design.[3]
These principles include a rigid major connector, multiple positive rest seats, mesial rests, parallel guide planes, the I-bar clasp design and the altered cast technique.
This presentation describes the original concept of the altered cast impression technique as described by Applegate[4] review studies of the technique and the clinical and laboratory phases required for distal extension RPD fabrication.
Case Report
A female patient aged about 50 years came with the complaint of missing upper and lower teeth. The patient presented with missing 13,15,16, 24, 27, 36, 37, 46, 47 and mandibular anterior 4 unit fixed partial denture [Figures 1 and 2].
Figure 1.
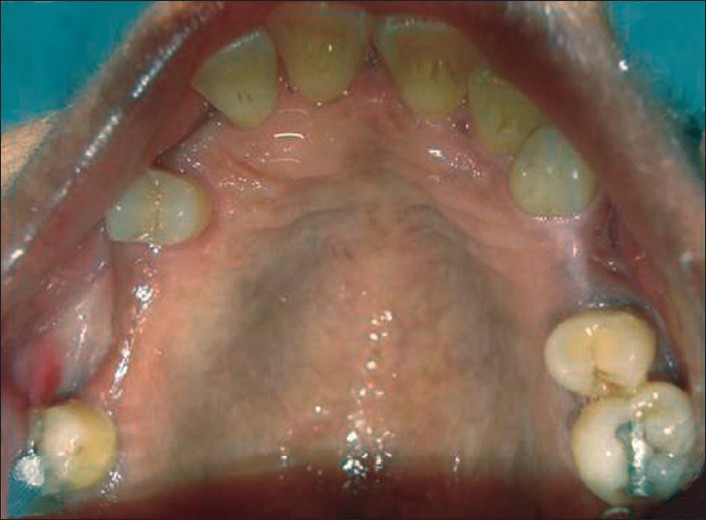
Maxillary edentulous arch with partial missing teeth
Figure 2.
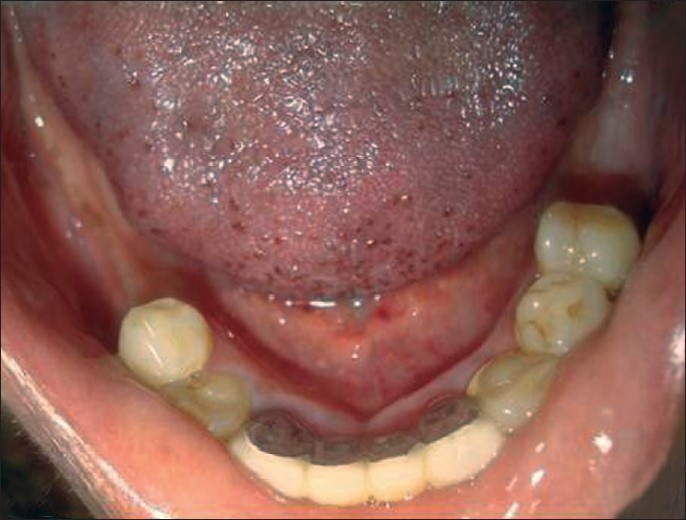
Mandibular edentulous arch with distal extension
The patient with maxillary and mandibular edentulism was examined in the usual fashion for diagnosis and treatment plan. Maxillary preliminary impressions were made with irreversible hydrocolloid and study casts were obtained.
The study casts were placed on a surveyor for examination and design of the cast framework. Mouth preparation was done and final impression of maxillary and mandibular arch were made with medium bodied elastomeric impression material. Secondary casts obtained were placed on a surveyor for examination and design of the cast framework
Master casts were duplicated, refractory cast were obtained, and the design was transferred from the master cast to the refractory cast. Investing and casting was completed. The completed framework was examined to ensure that it fits the cast accurately [Figures 3 and 4].
Figure 3.
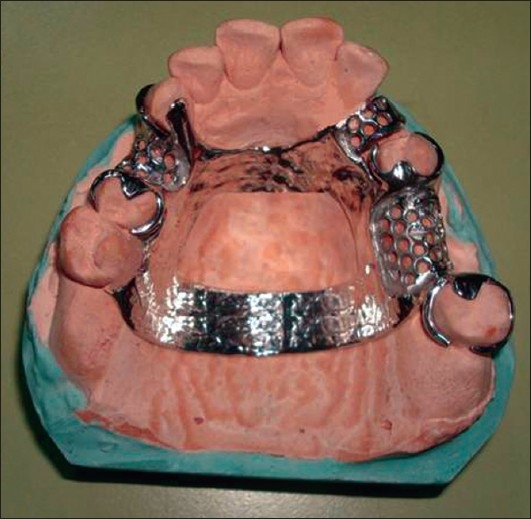
Maxillary metal framework
Figure 4.
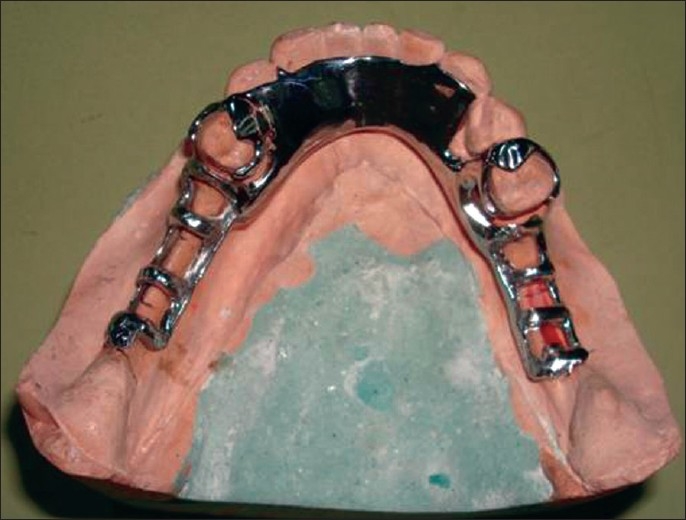
Mandibular metal framework
Once the cast framework was verified for acceptable fit orally [Figures 5 and 6], an acrylic resin custom tray was attached to the mandibular metal framework [Figure 7]. This tray was then border molded in the usual fashion for the desired extension, the fit of the metal framework to the teeth and soft tissues were checked [Figure 8].
Figure 5.

Maxillary metal try in
Figure 6.

Mandibular metal try in
Figure 7.
An acrylic resin custom tray attached to the mandibular metal framework
Figure 8.

Border molded tray for the desired extension
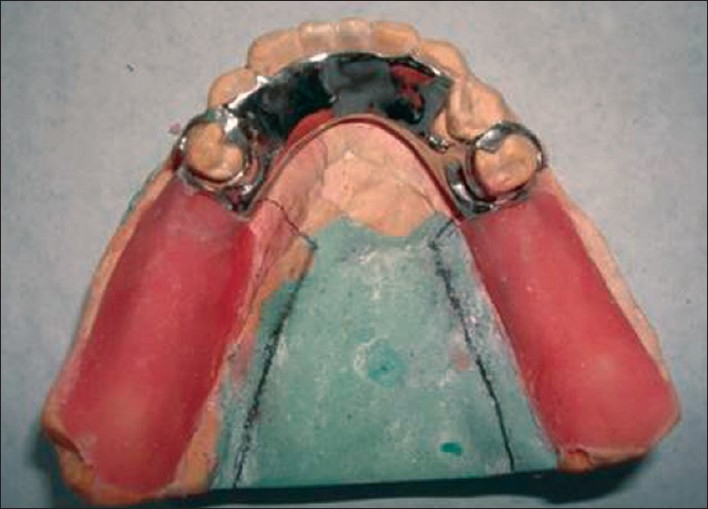
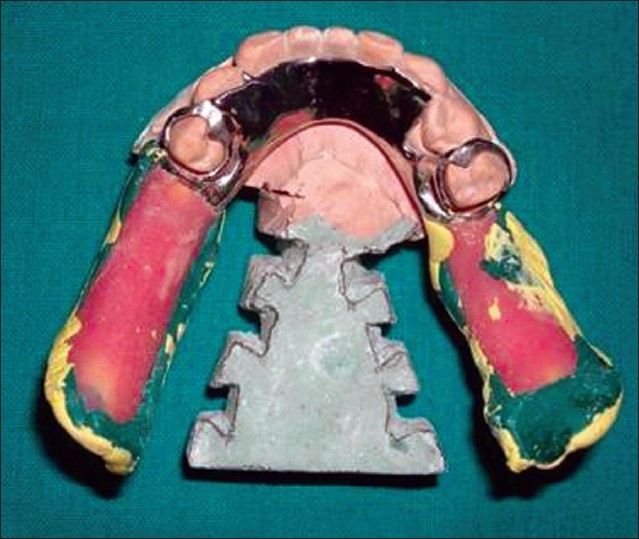
The final impression was made using zinc oxide eugenol impression paste [Figure 9]. While making impression, finger pressure was applied only to the parts of the framework that comes in contact with the teeth. The cast was altered in the laboratory. Two saw cuts were made perpendicular to each other. The first cut was made 0.5 mm to 1.0 mm distal to the most distal remaining tooth and perpendicular to the edentulous ridge. This cut was carried from the outer edge of the cast to 6.0 to 7.0 mm medial to the lingual vestibule. The second cut was made parallel and medial to the edentulous ridge, extending from the most posterior aspect of the cast to the most medial aspect of the first cut [Figure 10]. The cut surface of the cast was then grooves placed to aid in the retention of the newly poured stone [Figure 11]. Complete seating of the framework on the cast was essential before it is fixed in place with sticky wax [Figure 12]. The final impression was beaded and boxed in the usual manner and poured with die stone [Figure 13]. Working altered cast after beading and boxing was removed [Figure 14]. Finally usual remaining steps in the fabrication of removable partial dentures were carried out (jaw relation and try in procedures), denture delivery was done and post delivery instructions were given [Figures 15 and 16].
Figure 9.

Final impression made using zinc oxide eugenol. impression paste
Figure 10.

Cast with two saw cuts perpendicular to each other on either side of saddle
Figure 11.

The cut surface of the cast with grooves
Figure 12.
Seating of the framework on the cast with sticky wax
Figure 13.
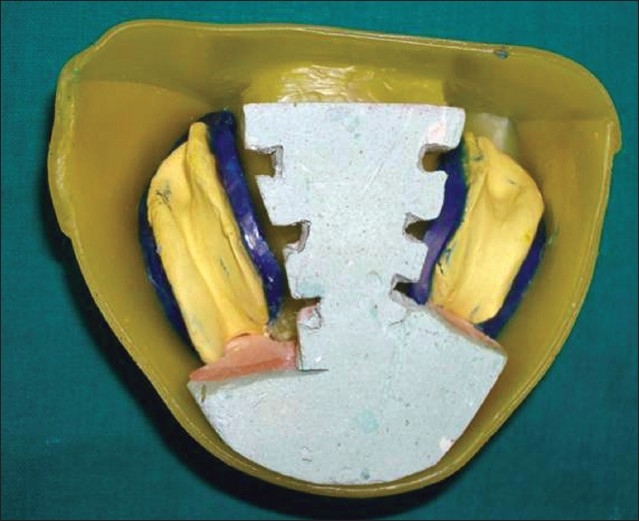
Final impression with beading and boxing
Figure 14.

An altered cast
Figure 15.

Anterior view of cast partial denture
Figure 16.

Occlusal view of mandibular cast partial denture
Conclusion
A favorably extended base will provide stimulation to the underlying bone and distribute forces uniformly. The altered cast technique allows the ridge, recorded in functional form, to be related to the teeth so that when the prosthesis is seated, it derives support simultaneously from the teeth and the denture base.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Leupold RJ, Kratochvil FJ. An altered cast procedure to improve tissue support for removable partial dentures. J Prosthet Dent. 1965;15:672–8. doi: 10.1016/0022-3913(65)90038-7. [DOI] [PubMed] [Google Scholar]
- 2.Feit DB. The altered cast impression technique revisited. J Am Dent Assoc. 1999;130:1476–81. doi: 10.14219/jada.archive.1999.0059. [DOI] [PubMed] [Google Scholar]
- 3.Becker CM, Kaiser DA, Goldfogel MH. Evolution of removable partial denture design. J Prosthodont. 1994;3:158–66. doi: 10.1111/j.1532-849x.1994.tb00147.x. [DOI] [PubMed] [Google Scholar]
- 4.Applegate OC. The cast saddle partial denture. J Am Dent Assoc. 1937;27:1280–91. [Google Scholar]