

Abstract
Background and Objective:
The objective of the study was to monitor Streptococcus mutans (SM) counts in saliva of children aged 5-7 years old over a period of 6 months with the subsequent use of Fuji IX, glass ionomer cement in atraumatic restorative technique (ART).
Materials and Methods:
One hundred children were selected to receive ART using Fuji IX glass ionomer cement. Caries status was recorded using DMFT index (WHO 1997) and revaluated after 6 months using DMFS index (WHO 1979). Saliva was collected for microbiological assessment of SM count on four occasions, baseline, 1 week, 1 month, and 6 months after ART approach. The results of the microbiological tests were statistically analyzed using the non-parametric Mann-Whitney rank test.
Results:
The results showed a significant reduction of SM levels in saliva immediately 1 week following the ART approach with mean SM counts of 1.5763 (106 CFU/ml) and 1.1286 (105 CFU/ml) pre- and 1 week post–ART, respectively. Reduction in the SM count was seen in 89.47% of children after 1 week of ART treatment. The mean SM count after 1 month and 6 months post-ART was 1.4814 (106 CFU/ml) and 1.4722(106 CFU/ml), respectively.
Conclusion:
It was concluded from the results that the ART technique was successful in reducing the SM counts in saliva significantly for a period of 1 week post treatment. Although the mean SM counts remained less than the baseline after 6 month evaluation, a trend toward re-establishment of SM to the baseline count was noticed.
Keywords: Colony forming units, glass-ionomer cement, non-parametric test, Streptococcus mutans
Introduction
The atraumatic restorative treatment (ART) approach is evolved in the response to the unavailability of the restorative treatment source in the population group.[1] FUJI IX, as a high strength posterior glass ionomer has been selected for the ART technique as it has been developed and intended to meet the requirements of conservation and minimal cavity design.[2] As FUJI IX glass ionomer has the property of continuing fluoride release, this material has the potential to alter the counts of salivary Streptococcus mutans (SM). With this background, this study has been conducted to evaluate the SM count in saliva of 5 to 7 years old children before and after ART.
Materials and Methods
The present study was conducted in the Department of Pedodontics and Preventive Dentistry. Ethical clearance for the study was obtained by local ethical committee. The children were selected from the outpatient clinic of Department of Pedodontics and Preventive Dentistry and the surrounding area in schools. Written informed consent was procured from parents of all participants prior to the participation in the study.
The following inclusion criteria were included to select the subjects.
Caries status of the children who depicted a baseline of minimum 3 DMFT.
Minimum of two decayed components present to receive the ART technique.
The primary molars having small clinically visible single surface dentinal lesions were included.
Healthy children without any systemic diseases were included in the study.
Children with sound permanent teeth were included in case of mixed dentition.
The examination was carried out by the single examiner and was assisted by alert and co-operative recorder who followed instructions explicitly and recorded the numerals clearly.
The examination of children between age group of 5 and 7 years (mean age 6.2600) for the baseline DMFT was carried out on dental unit and chair on the specially structured format by the criteria recommended by WHO (1997). The dental caries status was re-evaluated after 6 months of the ART technique for any increase in caries status by the DMFS index with code and criteria by WHO 1979.
The ART procedure for the restoration of single surface occlusal carious lesions on primary molars was performed according to manual for the ART approach to control dental caries, WHO 1997.
Materials for saliva collection
Sterile paraffin wax
Sterile bottles for saliva sample collection
Thioglycollate media (Himedia M 979, LOT No.YG2473.
Mitis Salivarius Agar Media (Himedia M259, Lot No: Y1100) with Potassium tillurite (FD 052) and Bacitracin.
Mitis Salivarius agar plate/ loop
Microbiological procedure
The saliva samples for counting SM was collected on four occasions i.e., baseline sample (before the procedure of ART), 1 week, 1 month, and 6 months after performing ART procedure.
The saliva samples of all the patients were identified by a code number during the period of sample collection and processing. The same code number was used for the particular patient during subsequent saliva sample collection. The children were given a sterile paraffin wax to chew to stimulate sufficient salivation to pour. Approximately 1 ml of saliva was collected and put into the bottle containing 1 ml of thioglycollate transport media.
The sample was transported to the laboratory immediately after collection and processed on the same day. The sample was vortexed (15 sec, Cyclomixer, CM 101). The sample was inoculated on the dry Mitis Salivarius Agar with potassium tillurite medium and bacitacin. The plates were incubated at 37 °C in 5-10% CO2 jar for 48 h. After 48 h, colony characteristics were studied and the number of colony forming units of MS (CFU/ml) of saliva was determined. Results of microbiological counts were analyzed statistically by the Mann-Whitney rank test.
Results
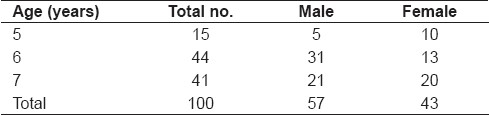
Among the total of 100 children included in the study, 57 were males and 43 were females [Table 1]. Detectable levels of SM were found in 98.96% children before the ART technique. The results demonstrated for the mean age 6.2600 with the mean baseline DMFT 3.5800 the baseline CFU/ml of SM was 1.5763(mean baseline 106 CFU/ml). However, the mean CFU/ml of SM post-treatment within a week significantly dropped down to 1.1286 (105 CFU/ml). The mean CFU/ml of SM evaluation at 1 month and 6 month period were almost similar giving the values of 1.4814 and 1.4722 (106 CFU/ml), respectively. Although the mean levels declined with the treatment within a week a trend of returning to values equivalent to the counts observed prior to the treatment were found. The standard deviation for the variables, namely age; baseline DMFT; CFU/ml baseline, 1 week, 1 month, and 6 months; DMFS were 0.7017; 0.6660; 0.4955; 0.4549; 0.5153; 0.5347, and 0.6660, respectively. Results within 6 months did not show increment in dental caries when subjects were evaluated for DMFS [W.H.O. (1979)] 6 months post-ART treatment. Differences in counts of salivary SM were analyzed for each test (namely baseline, 1 week, 1 month and 6 month post treatment) by the Mann-Whitney rank test.
Table 1.
Distribution of sample size
The counts of SM were highly significant with the value of test statistic 6.22544 between baseline and 1 week post-treatment. Following the ART technique carried out on the sample size between the period of baseline and 1 month post-treatment did not significantly change the counts, similar trend was found when baseline was compared with fourth or final salivary SM (CFU/ml), 6 month post-treatment, giving the value of test statistic (U): 1.36144 and 1.35897, respectively [Table 2]. The results for males and females did not show any significant difference [Table 3].
Table 2.
Results of statistical analysis for microbiological evaluation

Table 3.
Comparison of the results for four microbiological tests among males and females

However 1 week salivary counts of SM (CFU/ml) and the counts after 1 month were highly significant with the value of test statistic (U), 5.074374. Similar trend was found when 1 week and 6 month samples were compared giving high significance with value of test statistic (U) 5.290162. Between 1 month and 6 month post-treatment the value of test statistic (U) was 0.109905 which was not significant [Table 2].
Discussion
The ART technique one of the important component of oral health care has gained popularity as a minimal intervention procedure promoting oral health messages.
The ART technique basically was developed for under-developed countries in which basic resources like electricity are scarce and now this technique is gaining great acceptance. Removing carious tooth tissue with hand instruments alone and restoring the cavity by adhesive material in ART technique shall conserve as much as tooth structure as possible and will prevent further decay, tooth mortality.[1]
This study was carried out in Department of Pedodontics and Preventive Dentistry on the children aged between 5 and 7 years as similar to the study carried out by Honkala E, et al.[3] who concluded in their study that the ART approach is an appropriate treatment option for primary teeth in industrialized countries. It is not the only treatment option but could be used successfully in class I restorations of primary teeth. However, the principal objective to consider the ART technique in the context of other restorative procedures for dental caries was to ensure caries inhibition and to reduce tooth mortality.[4] Our data are in accordance with Franken JoE, Songpaisan Yupin, Phantumvanti P, Pitot Taco., 1996[5] who also confirmed success of the ART technique when used on single surface fillings. The results of post-ART treatment in our study did not show any failure in restoration.
The ability of streptococcus mutans to cause dental caries is well documented. However, in the context of effective treatment to combat this confounding factor either from the carious lesions or entire oral cavity has always been a challenge for the dental profession, as no form of effective treatment to remove the same entirely from the oral cavity is available. The presence of streptococcus mutans is strongly associated with carious lesions that occur on occlusal, interproximal, buccolingual surface of human teeth, and less strongly associated with the sound tooth surface.[6]
In the prevention of the dental caries, reducing salivary levels of cariogenic bacteria could be considered as a secondary consequence of using the ART technique, but it is not definitely without any importance.[7] In this study the sample included 100 children with 358 restorations with Fuji IX glass ionomer cement. The sampling method was standardized for the inclusion criteria and for the quantity of specimen saliva collected showed adequate recovery of SM. When compared with the caries status it showed positive association. Of the 100 children, SM was recovered in 98.96% of saliva sample. A correlation was established between the salivary levels of SM and dental caries which is in accordance with Kohler B, et al[8] Songpaisan E, et al.[9]
According to our data using the ART technique on the primary dentition with glass-ionomer cement Fuji IX on children with three to five DMFT has definitely contributed in reducing salivary levels of SM when other parameters such as diet, fluoride application, pit and fissure sealant, oral hygiene practices were not considered.
ART must be considered in context of other restorative procedures for dental caries for two significant reasons observed in this study. The mean values of SM in saliva at the baseline were 1.5763 (106 CFU/ml) which dropped down significantly to 1.1286(105 CFU/ml) after treatment. Moreover, it is acceptable to the patient in the study group as the ART technique uses hand instrument alone which is in accordance with other similar studies.[10–12] Pretreatment counts of salivary SM in the sample size of 100 children showed high reflection of severity of disease which was in accordance with the other studies.[9,13,14]
SM is known to colonize the teeth in a localized way and the site-specific evaluation has proved its prognostic value in initiating dental caries. Many investigators have used salivary levels of SM as the diagnostic aid to select individuals at risk as well as to evaluate any predictive value of preventive measures used as prophylactic treatment to combat the disease.[8]
In this study the results showed that the levels of SM reduced significantly immediately 1 week after the ART technique in 89.47% of children, which continued to be at lower level at least 6 months as similar to other microbiological studies.[15–17] Currently it is possible to conduct laboratory and chair side analysis of samples of saliva to determine the number of salivary SM. The concept of using microbiology in caries diagnosis and thereby reducing or eliminating these odontopathogens along with the ART as a means of controlling and preventing disease activity was one of the principle aim of this study.
Our results confirm that the use of microbiology in pediatric practice should not be dismissed as being of little value because microbiological values do not provide panacea though not appropriate in all cases. There is no doubt that the pre-ART and 1 week post-ART treatment have shown considerable reduction in CFU/ml of SM in saliva in this study. However results can be compared with other studies of bacterial changes after restoration. In this study the microbial levels declined with ART treatment but they seem to return to the values equivalent to the counts observed prior to the treatment by 1 month later. This finding has been substantiated by other researchers with similar study.[6,15,16] The outcome of our findings describes that the relationship between the caries and counts of SM though may not be absolute in all the hundred cases evaluated, the tests for this bacteria remains true as one of the predictors of future caries, as mentioned similarly by Bowden GH, 1996.[18]
It is important to realize, though our results have shown, that reductions of SM by treating the excavable cavities by the ART technique may not be synonymous with elimination of SM but with post-treatment clinical examination and estimation by DMFS index (WHO 1979) it was established that for a particular individual DMFT and DMFS have remained same. Glass ionomer cement is known to release the fluoride which may help to maintain the lower level of microorganisms under examination. This salient feature of glass ionomer cement (Fuji IX) is due to its potential to recharge fluoride, making it to certain extent cariostatic over a period of 6 months.[19–21]
The bacterial reduction may have resulted from the removal of diseased tissue, although the individuals after receiving ART therapy showed the significant reductions of SM in first week. Making direct comparisons with the similar studies is difficult. This investigation also reported trend toward reestablishment of SM over the period of 6 months after the initial reduction at 1 week post-ART. However, one of the explanations for resurgence of SM may be the organism's ability to readily colonize the restored surfaces.[20,22,23]
The return of the oral bacteria (SM) to pre-restorative levels in many individuals, as seen in this study, may imply that this restorative treatment alone would be a questionable modality for altering the oral flora with any permanence. In the future it will be interesting to obtain corresponding data with the relationship between SM and the success of different minimal intervention techniques in the larger population with the consideration of all possible parameters which are involved in the development of dental caries.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Groningen: WHO collaboration center for oral health services research; 1997. World Health Organization. Manual for the Atraumatic Restorative Treatment approach to control dental caries. [Google Scholar]
- 2.Tyas MJ, Anusavice KJ, Frenken Jo E, Mount GJ. Minimal intervention dentistry--a review.FDI Commission Project 1-97. Int Dent J. 2000;50:1–12. doi: 10.1111/j.1875-595x.2000.tb00540.x. [DOI] [PubMed] [Google Scholar]
- 3.Honkola E, Behbehani J, Ibricevic H, Kerosuo E, Al-Jame G. The atraumatic restorative treatment (ART) approach to restoring primary teeth in a standard dental clinic. Int J Paediatr Dent. 2003;13:172–9. doi: 10.1046/j.1365-263x.2003.00455.x. [DOI] [PubMed] [Google Scholar]
- 4.Frencken Jo E, Pilot Taco, Songpaisan Y, Phanpumvanit P. Atraumatic Restorative Treatment (ART): Rationale, technique, and development. J Public Health Dent. 1996;56:135–40. doi: 10.1111/j.1752-7325.1996.tb02423.x. [DOI] [PubMed] [Google Scholar]
- 5.Frencken Jo E, Songpaisan Yupin, Phantumvanit P, Pilot Taco. An atraumatic restorative treatment(ART) technique: Evaluation after one year. Int Dent J. 1994;44:460–4. [PubMed] [Google Scholar]
- 6.Keene Harris J, Shklair IL, Hoerman KC. Partial elimination of Streptococcus mutans from selected tooth surfaces after restoration of carious lesions and SnF2 prophylaxis. J Am Dent Assoc. 1976;93:328–33. doi: 10.14219/jada.archive.1976.0528. [DOI] [PubMed] [Google Scholar]
- 7.Toi CS, Bonecker M, Cleaton-Jones PE. Mutans Streptococcus strains prevalence before and after cavity preparation during Atraumatic Restorative Treatment. Oral Microbiol Immunol. 2003;18:160–4. doi: 10.1034/j.1399-302x.2003.00051.x. [DOI] [PubMed] [Google Scholar]
- 8.KÖhler B, Bjarnason S. Mutans Streptococcus, lactobacilli and caries prevalence in 11- and 12-year old Icelandic children. Community Dent Oral Epidemiol. 1987;15:332–5. doi: 10.1111/j.1600-0528.1987.tb01747.x. [DOI] [PubMed] [Google Scholar]
- 9.Songpaisan E, Serinirach B, Kuvatanasuchati J, Bratthall D. Mutans Streptococcus in Thai population: Relation to caries and changes in prevalence after application of fissure sealants. Caries Res. 1994;28:161–8. doi: 10.1159/000261639. [DOI] [PubMed] [Google Scholar]
- 10.Van Amerongen WE, Rahimtoola Salim. Is ART really atraumatic? Community Dent Oral Epidemiol. 1999;27:431–5. doi: 10.1111/j.1600-0528.1999.tb02044.x. [DOI] [PubMed] [Google Scholar]
- 11.Frencken Jo E, Holmgren CJ. How effective is ART in the management of dental caries? Community Dent Oral Epidemiol. 1999;27:423–30. doi: 10.1111/j.1600-0528.1999.tb02043.x. [DOI] [PubMed] [Google Scholar]
- 12.Schriks MC, Van Amerongen WE. Atraumatic perspectives of ART: Psychological and physiological aspects of treatment with and without rotary instruments. Community Dent Oral Epidemiol. 2003;31:15–20. doi: 10.1034/j.1600-0528.2003.00021.x. [DOI] [PubMed] [Google Scholar]
- 13.Shi Yang, Barmes D, Bratthall D, Leclercq MH. WHO pathfinder caries survey in Beijing extended with data for prevalence of mutans streptotocci. Int Dent J. 1992;42:31–6. [PubMed] [Google Scholar]
- 14.Beighton D, Manji F, Baelum V, Fejerskov O, Johnson NW, Wilton JM. Associations between salivary levels of streptococcus mutans, streptococcus sobrinus, lactobacilli, and caries experience in Kenyan adolescents. J Dent Res. 1989;68:1242–6. doi: 10.1177/00220345890680080601. [DOI] [PubMed] [Google Scholar]
- 15.Carvalho CK, Bezerra AC. Micribiological assessment of saliva from children subsequent to Atraumatic Restorative Treatment (ART) Int J Paediatr Dent. 2003;13:186–92. doi: 10.1046/j.1365-263x.2003.00432.x. [DOI] [PubMed] [Google Scholar]
- 16.Peretz B, Sarit F, Eidelman E, Steinberg D. Mutans streptococcus counts following treatment for early childhood caries. J Dent Child. 2003;70:111–4. [PubMed] [Google Scholar]
- 17.Twetman S, Fritzon B, Jensen B, Hallberg U, Stahl B. Pre- and post-treatment levels of salivary mutans streptococcus and lactobacilli in pre-school children. Int J Paediatr Dent. 1999;9:93–8. doi: 10.1046/j.1365-263x.1999.00108.x. [DOI] [PubMed] [Google Scholar]
- 18.Bowden GH. Mutans streptococcus caries and chlorhexidine. J Am Dent Assoc. 1996;62:700–7. [PubMed] [Google Scholar]
- 19.Scherer W, Lippman N, Kaim J. Antimicrobial properties of glass-ionomer cements and other restorative materials. Oper Dent. 1989;14:77–81. [PubMed] [Google Scholar]
- 20.Berg JH, Farrell JE, Brown LR. Class II glass ionomer/silver cermet restorations and their effect on interproximal growth of mutans streptococcus. Pediatr Dent. 1990;12:20–3. [PubMed] [Google Scholar]
- 21.Rodriguez Loyola JP, Garcia-Godoy F, Lindquist Renicko. Growth inhibition of glass ionomer cements on mutans streptococcus. Pediatr Dent. 1994;16:346–9. [PubMed] [Google Scholar]
- 22.Van Dijken J, Persson S, Sjostrom S. Presence of Streptococcus mutans and lactobacilli in saliva and on enamel, glass ionomer cement, and composite resin surfaces. Scand J Dent Res. 1991;99:13–9. doi: 10.1111/j.1600-0722.1991.tb01017.x. [DOI] [PubMed] [Google Scholar]
- 23.Wright JT, Cutter GR, Dasanayake AP, Stiles HM, Caufield PW. Effect of conventional dental restorative treatment on bacteria in saliva. Community Dent Oral Epidemiol. 1992;20:138–43. doi: 10.1111/j.1600-0528.1992.tb01548.x. [DOI] [PubMed] [Google Scholar]