

Abstract
The dilemma confronting many dentists today is that innovations and well-defined specializations have greatly enlarged the treatment realm for tooth preservation as well as tooth replacement. The objectives should be preservation of the remaining tooth structure, restoration of optimum function, esthetics with least invasive procedures, cost effective, and short treatment time. The number of remaining natural teeth is one of the most widely used method for evaluating oral health and the prosthetic treatment of patients with a mutilated dentition. Though the treatment of these patients can be complex, but there are some important principles applicable in most cases. This case report demonstrates a satisfying full mouth rehabilitation using the Hobo and Takayama twin-stage procedure for a patient with esthetically and functionally compromised dentition. The final prosthesis with this twin-stage technique ensured a restoration with a predictable posterior disclusion and anterior guidance in harmony with the condylar path.
Keywords: Canine-guided occlusion, cusp angle, diagnostic wax-up, twin stage
Introduction
Dentistry certainly must be an important part of an overall cosmetic upgrade, since improvements in the face and the smile play an important role in changing a person's appearance and improving self-esteem. The phrase full-mouth rehabilitation means different things to different people. Though the full-mouth rehabilitation and its philosophies are often intrigue in nature, but the esthetic and functional accomplishment of rehabilitation is always satisfying. Anterior guidance is crucial in human occlusion because it influences molar disclusion that controls horizontal forces. Molar disclusion is determined by a cusp-shape factor and an angle of hinge rotation. The Hobo–Takayama method for creating molar disclusion by using a twin-stage technique will be described. This technique develops anterior guidance to create a predetermined, harmonious disclusion with the condylar path. Condition 1 is used to incorporate a cusp-shape factor and Condition 2 is used for the angle of hinge rotation. This method does not require special equipment and is an uncomplicated procedure suitable for daily practice. The mystery of establishing the optimal anterior guidance is also clarified, including accurate development of a specific degree of disclusion desired by the dentist.
Case Report
A healthy 25-year-old male reported to the Department of Prosthodontics, Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, with a chief complaint of unsightly appearance due to generalized discolored and small-sized teeth since childhood, generalized sensitivity, and difficulty in chewing [Figure 1]. The patient gave a medical history of epilepsy 7 years back and was under medication for the same condition. The patient's dental history dated back to 10 years when he first noticed discoloration of his both upper and lower teeth. The patient didn’t report any symptoms of temporomandibular joint disorder or myofascial pain dysfunction.
Figure 1.

Pre-op views showing discolored and small teeth
Clinical findings
Extraoral: The patient had no facial asymmetry, or muscle tenderness. The mandibular range of motion was within normal limits. The TMJ, the muscles of mastication, and the facial expression were asymptomatic.
Intraoral: There was generalized discoloration of the upper and lower dentition with fair oral hygiene. The mandibular arch was fully dentate and the maxillary arch was having missing 18 and 28. No gross abnormalities were noted in the overall soft tissues of the lips, cheeks, tongue, oral mucosa, and pharynx. A generalized pitting defect was noted. Open contact was present in relation to upper and lower anterior teeth with a midline diastema.
Occlusal: The patient was having mild-to-moderate genralized attrition of dentition with moderate loss of vertical dimension. The patient presented with a bilateral class I molar and canine relationship. The patient demonstrated a slide from centric relation to maximum intercusption. The patient's lateral excursions showed bilateral balanced occlusion. The incisal edge glided along the palatal surfaces of maxillary anteriors during protrusion, along with posterior teeth interference. A freeway space of 2 mm was recorded.
Goals of rehabilitation
The goals were as follows:
To rehabilitate the entire hypoplastic dentition in functional harmony with the stomatognathic system
To rehabilitate using the twin-stage procedure to produce a definite amount of disocclusion during eccentric movements
To develop a canine-guided occlusion.
Treatment procedure
The rehabilitation was carried out as follows:
Maxillary and mandibular impressions were made in the alginate impression material and diagnostic casts were obtained.
Based on patient's moderate loss on vertical dimension, a hypothetical increase of 3 mm in the vertical dimension of occlusion was carried out using a Lucia jig and interocclusal record based on the evaluation of the mounted diagnostic cast in centric relation [Figure 2]. Then the maxillary cast was mounted using face-bow transfer onto a semi-adjustable articulator (Whip-mix) and the mandibular cast mounted was using the Lucia jig and centric relation record.
Diagnostic wax-up was done at the established new vertical to see the final outcomes [Figure 3]. Keeping in mind the following indications and objectives, we carried out diagnostic wax-up for our full-mouth rehabilitation case:
Figure 2.

Mounted U/L diagnostic cast with lucia jig and centric record
Figure 3.
U/L diagnostic Wax-up
Indications
Anterior guidance requires alteration
Existing occlusal scheme requires alteration
Vertical dimension need to be changed
Mutilated dentition
Purpose
Arch shape and contour
To rehearse a proposed restorative plan
To explain the intended procedure to the patient
To establish the occlusion
Dentist can explore all the treatment alternatives before selecting a therapy
Provisional restoration
To provide additional information to the technician.
-
4.
Then an occlusal splint was provided to the patient as part of reversible interventional modalities to evaluate adaptation of the patient to altered VDO. The patient was kept in diagnostic and observational period of 6 weeks before the definitive restorative phase of rehabilitation was started.
-
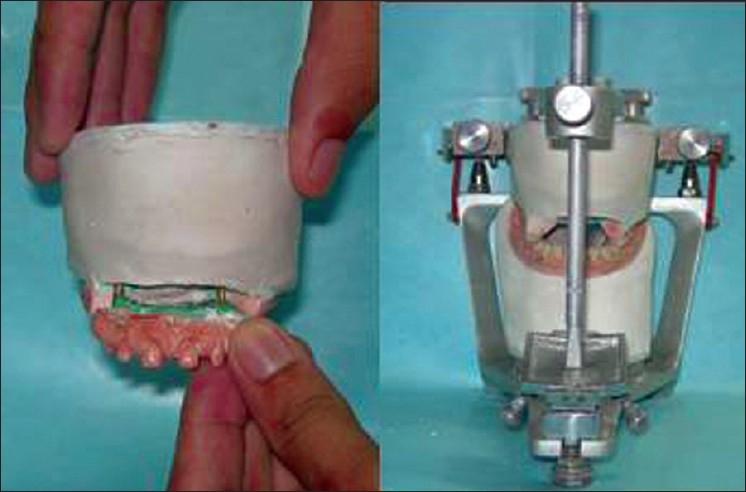
5.
The teeth were prepared and Stage I temporary restorations were fabricated chairside segment by segment during several appointments to minimize patient discomfort and efficiently use the appointment time [Figures 4 and 5]. The patient's vertical dimension of occlusion was maintained by using unprepared teeth as occlusal vertical stops. Minimal occlusal reduction is indicated for patients scheduled for rehabilitation at an altered vertical dimension of occlusion. The definitive phase for full coverage metal–ceramic tooth preparations was completed for the entire dentition with minimal occlusal reduction; Stage II temporaries were fabricated using the putty index of the diagnostic wax-up and cemented with ZnO noneugenol cement [Figure 6]. A final full arch impression for maxillary/mandibular teeth was made using heavy-body and light-body impression material in the custom tray and casts were poured in die stone. This assembly was mounted on Whip-mix articulator using the face-bow, Lucia jig, and centric record at the previously determined vertical dimension.
-
6.
All the wax patterns were cast, and all metal copings were tried in and adjusted as needed [Figure 7]. Definite restorations with PFM crowns exhibiting a vital and natural appearance with proper contour, shade, and optimal incisal translucency were fabricated [Figure 8].
-
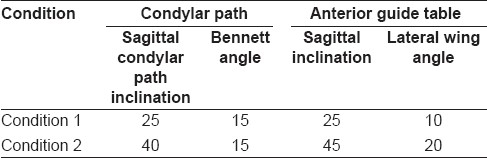
7.
The articulator was programmed to different conditions of the twin-stage procedure as in Table 1.
Figure 4.

U/L tooth preparation and retraction cord in place
Figure 5.

Stage I temporaries
Figure 6.

Stage II temporaries
Figure 7.

Metal copings try-in
Figure 8.
PFM crowns
Table 1.
Articulator adjustment values
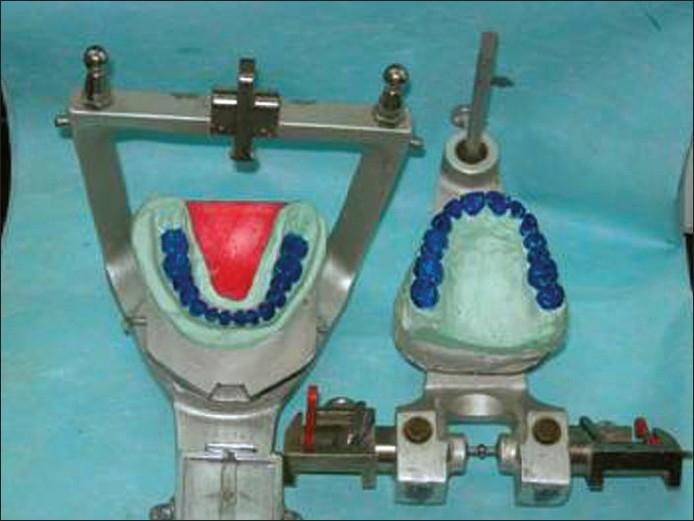
Fabrication of the cusp angle
For this, a standard effective cusp angle of 25° was set to Condition 1 of the twin-stage procedure [Table 1] and the maxillary and/or mandibular anterior segment was removed [Figure 9]. Then the occlusal morphology of the posterior PFM crown build-ups was completed and balanced articulation was obtained [Figure 10].
Figure 9.
Condition 1 (25° Cusp angle)
Figure 10.

Establishment of balanced articulation
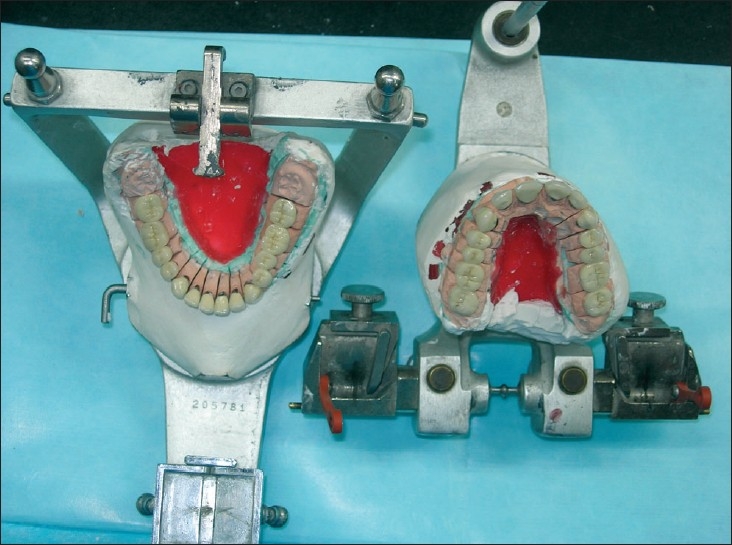
Fabrication of anterior teeth
The anterior segment of the cast was reassembled. Then, anterior PFM crown build-ups were completed after the values had been adjusted to Condition 2 of the twin-stage procedure [Table 1] to achieve an incisal guidance of 40°;, which produced a standard amount of disocclusion. The anterior teeth produced contact on anterior teeth during protrusion and contact on canines during lateral movement [Figure 11].
Figure 11.

Condition 2 with canine guided occlusion (On articulator and intra oral view)
-
8.
Permanent cementation was done with GIC type I luting cement.
-
9.
Oral hygiene instructions were reviewed, emphasizing brushing habits and the use of floss threaders and dental floss.
-
10.
Follow-up was carried out at regular intervals and the patient's post-operative condition was satisfactory [Figures 12 and 13].
Figure 12.

Post-op intraloral views
Figure 13.

Extraoral pre-op and post-op views
Discussion
Full-mouth reconstructions involving full arch preparations, impressions, provisional restorations, and master casts are regarded as simultaneous reconstructions. A variety of techniques may be used in simultaneous constructions to obtain complete arch dies and mounted casts. These techniques assist in concomitant laboratory construction of the units. When all of the prepared teeth are on a single articulator, there is flexibility in developing the occlusal plane, occlusal theme, embrasures, crown contour, and esthetics. The chairside disadvantages include[1] arduous, unpredictable patient visits,[2] full arch anesthesia,[3] full arch chairside treatment restorations,[4] multiple occlusal records, and[5,6] possible loss of the vertical dimension of occlusion. Miscellaneous disadvantages are (1) the need for accurate cross-arch multiple tooth impressions and/or (2) the need for transfer techniques to fabricate full arch working casts.[7,8] An alternative approach to the full-mouth simultaneous reconstruction is to complete one quadrant before beginning another. The advantages of this approach are that it is primarily chairside and includes preparation and final impressions of select teeth, maintenance of vertical dimension, quadrant anesthesia, and shorter, predictable appointments. The disadvantages of the quadrant reconstruction include restrictions for achieving ideal occlusion when altering the vertical dimension, occlusal plane, and embrasure development. The existing opposing dentition limits the reconstruction of an isolated quadrant. Esthetic consistency can be compromised because the porcelain restorations are made in stages. The advantages of the simultaneous and quadrant full-mouth reconstruction are combined in the present technique. The heat-processed treatment restorations are the key factors in providing both clinical and laboratory advantages. They closely resemble the final restorations while maintaining vertical and centric relation, minimizing the need for multiple and complicated occlusal records. Treatment restorations also provide a stable and esthetic interim prosthesis during the fabrication of the final restoration and allow appraisal of an altered vertical dimension of occlusion. The cost and laboratory time involved in fabricating the processed acrylic resin temporary restorations are a limitation but the complexity of the patient's treatment warrants the extra effort.[8] The mechanism of anterior guidance was reviewed from recent mandibular movement studies to provide a basis for understanding the twin-stage technique, which is a practical method for establishing anterior guidance from the condylar path.[9,10] Anterior guidance and the condylar path previously were considered independent factors. It is an established fact that anterior guidance influences the working condylar path and even changes when the lateral incisal path deviates from the optimal orbit. This supports the hypothesis that anterior guidance and the condylar path are dependent factors. In setting anterior guidance, it is recommended to set the working condyle so that it moves straight outward along the transverse horizontal axis. The angle of hinge rotation produced by the angular difference between anterior guidance and the condylar path assists posterior disclusion but is not solely responsible. The anatomy of the cusps is created by establishing the appropriate form of the posterior cusps aligned to the condylar path; thus it also contributes to posterior disclusion. Posterior disclusion is crucial in controlling harmful lateral forces but the factors that determine the precise amount of disclusion have not been established. The disclusions recorded in healthy adults were 1.1 ± 0.6 mm in protrusive movement and 0.5 ± 0.3 mm on the working side and 1.0 ± 0.6 mm on the nonworking side during lateral movement. These numbers correlated with the deviation in the condylar path.[10] The molars must disclude slightly more than the deviation in the condylar path to avoid occlusal interferences.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Kazis H. Complete mouth rehabilitation through restoration of lost vertical dimension. J Am Dent Assoc. 1948;37:19–39. doi: 10.14219/jada.archive.1948.0175. [DOI] [PubMed] [Google Scholar]
- 2.Hausman M, Hobo S. Occlusal reconstruction using transitional crowns. J Prosthet Dent. 1961;11:278–87. [Google Scholar]
- 3.Braly BV. A preliminary wax-up as a diagnostic aid in occlusal rehabilitation. J Prosthet Dent. 1966;16:728–30. [Google Scholar]
- 4.Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system: Part II: A study of the Bennett movement. J Prosthet Dent. 1984;51:642–6. doi: 10.1016/0022-3913(84)90409-8. [DOI] [PubMed] [Google Scholar]
- 5.Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system: Part III: Rotation center of lateral movement. J Prosthet Dent. 1984;52:66–72. doi: 10.1016/0022-3913(84)90184-7. [DOI] [PubMed] [Google Scholar]
- 6.Hobo S. Formula for adjusting the horizontal condylar path of the semiadjustable articulator with interocclusal records: Part I: Correlation between the immediate side shift, the progressive side shift, and the Bennett angle. J Prosthet Dent. 1986;55:422–6. doi: 10.1016/0022-3913(86)90167-8. [DOI] [PubMed] [Google Scholar]
- 7.Hobo S. Formula for adjusting the horizontal condylar path of the semiadjustable articulator with interocclusal records: Part II: Practical evaluations. J Prosthet Dent. 1986;55:582–8. doi: 10.1016/0022-3913(86)90036-3. [DOI] [PubMed] [Google Scholar]
- 8.Binkley TK, Binkley CJ. A practical approach to full mouth rehabilitation. J Prosthet Dent. 1987;57:261–6. doi: 10.1016/0022-3913(87)90293-9. [DOI] [PubMed] [Google Scholar]
- 9.Hobo S, Takayama H. Effect of canine guidance on the working condylar path. Int J Prosthodont. 1989;2:73–9. [PubMed] [Google Scholar]
- 10.Hobo S. Twin-tables technique for occlusal rehabilitation: Part I: Mechanism of anterior guidance. J Prosthet Dent. 1991;66:299–303. doi: 10.1016/0022-3913(91)90253-s. [DOI] [PubMed] [Google Scholar]