

Abstract
Introduction:
Sterilization of the root canal is a prime aim of successful endodontics. The cleaning and shaping of the canal is directed as achieving this goal. The extrusion of apical debris has a deleterious effect on the prognosis of root canal treatment. Several instrument designs and instrumentation techniques have been developed to prevent this.
Materials and Methods:
Forty caries free single rooted human mandibular premolar teeth were divided in four groups of ten teeth each. Teeth in each group were instrumented until the working length with rotary ProTaper, K3, Mtwo systems, and hand K-type stainless steel files. Debris and irrigant extruded from the apical foramen were collected into vials and the amounts were quantitatively determined. The data obtained were analyzed using Kruskal-Wallis one-way analysis of variance and Mann-Whitney U tests.
Results:
The results show that all instrumentation techniques produced significant amount of extruded debris and irrigant. The engine-driven nickel-titanium systems showed less apical extrusion of debris and irrigant than manual technique. No statistically significant difference was found between the groups at [P > 0.05]. Maximum apical debris and irrigant extrusion was seen with K-file group and least in the Mtwo group.
Conclusions:
The use of rotary files and techniques to perform instrumentation does show less extrusion of the debris and irrigant from the apex. This can contribute to more successful endodontic therapy.
Keywords: Debris, hand files, irrigant, rotary endodontics
Introduction
Complete preparation of the root canal space is one of the most important stages in endodontic treatment. During preparation, irrigant and debris such as bacteria, dentin fillings, and necrotic tissue may be extruded into the periradicular region leading to periapical inflammation and postoperative flare-ups.[1] Tissue reactions following instrumentation short of the apex are milder than those reactions that follow instrumentation beyond the apex.[2] It is also known that inflammatory reactions can cause bone resorption, edema, and pain.[3] Therefore, it is logical to assume that minimizing the amount of apically extruded material should minimize postoperative reactions.
All preparation techniques and instruments have been reported to be associated with extrusion of infected debris, even when preparation is maintained short of the apical terminus.[4] Vande Visse and Brilliant first quantified the amount of debris apically extruded during instrumentation. They found that instrumentation with irrigant produced extrusion, whereas instrumentation without irrigant produced no collectible debris. Martin and Cunningham[5] reported that less debris was extruded when the intracanal preparation was accomplished with and ultrasonic instrument. Al-Omari and Dummer[6] verified that techniques involving a linear filing motion, such as the step back techniques, create a greater mass of debris than those involving some sort of rotational action. Reddy and Hicks[7] were the first to compare apical debris extrusion between manual instrumentation and engine-driven techniques. When comparing the mean weights of apically extruded debris, they noted that the step back technique produced significantly more debris than the engine-driven techniques and the balanced force tech-nique. They suggested that rotation during instrumenta-tion, in both the engine-driven techniques and the balanced force technique, tended to pack the dentinal debris into the flutes of the instruments and directed them toward the orifice
Engine-driven nickel-titanium instruments have been shown to prepare the root canal rapidly, and maintain the canal shape and working length with few aberrations during root canal preparation. They are available in various designs that differ in tip and taper design, rake angles, helical angles, pitch, and presence of radial lands.[8]
The distinguishing feature of the ProTaper System is the progressively variable tapers of each instrument that develop a “progressive preparation” in both vertical and horizontal directions. The ProTaper cross-sectional design resembles that of a reamer, with three machined cutting edges and convex core.[9] K3 instruments (Sybron Endo, West Collins, CA) are reported to have a slightly positive rake angle in combination with so-called radial land relief and asymmetrical cross-sectional design.[9,10] The M two cross-sectional design resembles that of the S-file, no radial lands, progressive blade chamber (pitch) in the apical-coronal direction and a non-cutting tip.[11]
The purpose of this study was to compare in vitro the amount of debris and irrigant extruded apically from extracted teeth, using manual technique and crown-down pressure less technique by ProTaper, K3, and Mtwo instruments.
Materials and Methods
Forty freshly extracted human single-rooted mandibular premolar teeth with mature apices were selected. All teeth were radiographed in bucco-lingual and proximal directions to check for a single canal and single apex. Teeth with calcification and open apices were excluded. Endodontic access cavities were prepared (Endo Access Bur, Dentsply Maillefer, Switzerland) in a high-speed handpiece and pulpal remnants were extirpated using a broach.
Test apparatus
Glass vials with rubber stoppers were adjusted for use using a heated instrument to create a hole through the centre of each. A tooth was inserted under pressure into a rubber stopper up to the cemento-enamel junction. The apical part of the root was suspended within the vial; which acted as a collecting container for apical material evacuated through the apical foramen. A bent 19-gauge needle was forced alongside the rubber stopper to use as a drainage cannula and balance between the air pressure inside and outside the vials. Two coats of nail varnish were applied to the external surface of all roots. A hole was created in the nail varnish that covered the apical foramen using a size 15 K-file. During this procedure, only 1 mm of instrument was extruded. The rubber stopper with the tooth was then fitted into the mouth of the vial. Glass vials were entirely filled with 0.9% saline solution.
Root canal preparation
After working length determination, the vials were divided in 4 groups of 10 each. Then the rotary NiTi instrument groups were prepared with an Endomate endodontic handpiece at low speed (300 rpm) and automatic reverse function mode.
Group 1: ProTaper rotary files were used in a crown down manner according to manufacturer's recommendations. (Sequence – S1-Sx-S2-F1-F2)
Group 2: K3 instruments were used in a crown down manner according to the manufacturer's instructions. (Sequence – 35-30-25)
Group 3: Mtwo rotary files were used according to manufacturer's recommendation (Sequence – 10/0.04-15/0.05-20/0.06-25/0.06)
Group 4: K-file instruments were used in a step back manner. Apical preparation was done up to size 30 and the step back technique was used with a reduction of 1 mm in working length for an increment in each file size until size 45. Recapitulation was done to working length with 30 size file.
A total volume of 7 mL of 3.1% Sodium Hypochlorite was used in each root canal for irrigation because of the different numbers of the files in groups. The irrigant was delivered by disposable plastic syringe with an attached 27-gauge stainless steel needle that had been placed down the canal until slight resistance was felt. Extruded irrigant was collected from the needle into a disposable plastic insulin syringe attached to the Canula [Table 1]. The volume of the extruded irrigant was determined using the 0.1-mL increment on the syringe.
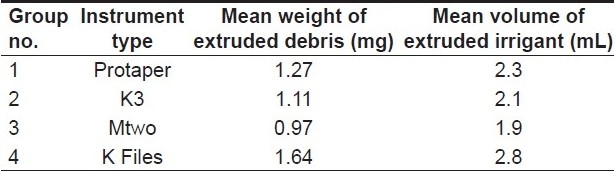
Table 1.
Mean weight of extruded debris and mean volume of extruded irrigant in all groups.
After determining the volume of the extruded irrigant, the rubber stopper-tooth-needle unit was removed along the collecting vial and volume of the extruded irrigant was added to the vials. Vials were stored at 37°C for 15 days to evaporate the fluid. After 15 days, salt deposits and dry debris with vials were weighed to 10-5 precision. This is the first weight measurement.
Vials were cleaned with distilled water, dried, and entirely filled with 0.9% saline solution and the rubber stopper-tooth-needle unit was fitted into the mouth of the saline-filled vial. Excess saline solution was drained out through the needle and then the rubber stopper unit was removed. Saline solution (0.9%) of volume identical to collected irrigant from the preparation was added and the vials were stored at 37°C for 15 days to evaporate the fluid again. Salt deposits and vials were again weighed to 10-5 precision. This is the second weight measurement.
Mean first weights were compared with the mean second weights and their difference was recorded as the weight of the extruded debris. The volume of the extruded irrigant was directly measured from the syringe attached to the cannula. Statistical analysis of the data was performed using Kruskal-Wallis one-way analysis of variance and Mann-Whitney U tests.
Results
The results indicated that all instruments tested had a measurable apical extrusion of debris and irrigant. No statistically significant difference was observed among all groups in terms of debris extrusion (P > 0.05). Most apical debris and irrigant extruded was seen in the manual technique group and least in the Mtwo group.
Discussion
The main objective of the present study was to assess the apical extrusion of dentin debris and irrigant as a result of canal shaping by different preparation; molar teeth were carefully selected according to tooth type, canal size, working length, and canal curvature. The teeth were digitally radiographed from clinical and proximal views to ensure that they had single canals and orifices. In previous studies, Reddy and Hicks[7] used single-rooted mandibular premolar teeth. Myers and Montgomery[12] used single-rooted maxillary lateral incisors and mandibular premolars, Ferraz et al,[13] used maxillary and mandibular central and lateral incisors with single canals, and Lambrianidis et al, used maxillary central and lateral incisors.
In this study, the canal working length was 1 mm short of the apical foramen. Martin and Cunningham[5] demonstrated greater debris extrusion when canals were instrumented at a length where the file was observed to just protrude through the apical foramen versus 1 mm short of the apical foramen. Myers and Montgomerz[12] clearly showed that a working length 1 mm short of canal length contributed to significantly less debris extrusion. Beeson et al,[14] reported that, when the instrumentation was performed to the apical foramen, significantly more debris was forced apically than when instrumen-tation was 1 mm short.
In this study, using engine-driven Nickel-Titanium instruments for the canal shaping extruded less debris and irrigant than K-files. In case of engine-driven instruments early flaring of the coronal part of the preparation may improve instrument control during preparation of the apical third of the canal. The rotary motion tends to direct debris towards the orifice, avoiding its compaction in the root canal.[15]
In case of K-files, the reason for more apical extrusion of debris is that the file acting apical third acts as a piston that tends to push the debris through the foramen and less space is available to flush it out coronally.
In this study, group I (Protaper) produced more apical debris than group II (K3) because K3 has unique helical angle and pitch than protaper. Group III (M two) produced less debris than group I (Protaper), Group II (K3) and Group IV (K-files) because the distance between the cutting blades increases from the instrument tip to the shaft,and the pitch is progressive. The space for dentin removal is deeper at the back of the blade. This reduces the risk of apical extrusion of debris.
Zarrabi et al,[16] compared Profile, RaCe, and Flex-Master instruments with the step-back technique and reported that the step-back technique extruded greater debris than rotary instruments. Ferraz et al,[13] reported that the Profile instruments induced less extruded debris and irrigant than manual technique. Our results were similar to previous studies that showed that engine-driven instruments extruded less debris and irrigant than manual technique.
Based on the results, all instrumentation techniques produced extruded debris and irrigant. However, the engine-driven nickel-titanium systems were associated with less apical extrusion and irrigant.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Seltzer S, Naidorf IJ. Flare-ups in endodontics: I. etiological factors. J Endod. 1985;11:472–8. doi: 10.1016/S0099-2399(85)80220-X. [DOI] [PubMed] [Google Scholar]
- 2.Seltzer S, Soltanoff W, Sinai I, Goldenberg A, Bender IB. Biologic aspects of endodontics. Part III. Periapical tissue reac-tions to root canal instrumentation. Oral Surg Oral Med Oral Pathol. 1968;26:694–705. doi: 10.1016/0030-4220(68)90442-8. [DOI] [PubMed] [Google Scholar]
- 3.Naidorf IJ. Endodontic flare-ups: Bacteriological and immuno-logical mechanisms. J Endod. 1985;11:462–4. doi: 10.1016/S0099-2399(85)80218-1. [DOI] [PubMed] [Google Scholar]
- 4.Vande Visse JE, Brilliant JD. Effect of the irrigation on the production of extruded material at the root apex during instrue mentation. J Endod. 1975;1:243–6. doi: 10.1016/s0099-2399(75)80227-5. [DOI] [PubMed] [Google Scholar]
- 5.Martin H, Cunningham WT. The effect of endosonic and hand : Manuplation on the amount of root canal material extruded. Oral Surg Oral Med Oral Pathol. 1982;53:611–3. doi: 10.1016/0030-4220(82)90350-4. [DOI] [PubMed] [Google Scholar]
- 6.Al-Omari MA. Dummer PMH/Canal blockage and debris extrun with eight preparation techniques. J Endod. 1995;21:154–8. doi: 10.1016/s0099-2399(06)80443-7. [DOI] [PubMed] [Google Scholar]
- 7.Reddy SA, Hicks ML. Apical extrusion of debris using two hand and two rotary instrumentation technique. J Endod. 1998;24:108–3. doi: 10.1016/S0099-2399(98)80179-9. [DOI] [PubMed] [Google Scholar]
- 8.Thompson SA, Dummer PM. Shaping ability of ProFile.04 Taper Series 29 rotary nickel-titanium instruments in simulated root canals. Part 1. Int Endod J. 1997;30:1–7. doi: 10.1111/j.1365-2591.1997.tb01093.x. [DOI] [PubMed] [Google Scholar]
- 9.Schafer E, Florek H. Efficiency of rotary nickel-titanium K3 instruments compared with Pro Taper. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2003;36:199–207. doi: 10.1046/j.1365-2591.2003.00643.x. [DOI] [PubMed] [Google Scholar]
- 10.Bergmans E, Van Cleynenbreugel J, Wevers M, Lambrechts P. Mechanical root canal preparation with Ni-Ti rotary instruments: Rationale, performance and safety.Status report for the American Journal of Dentistry. Am J Dent. 2001;14:324–33. [PubMed] [Google Scholar]
- 11.Tinaz AC, Alacam T, Uzun O, Maden M, Kayaoglu G. The effect of disruption of apical constriction on periapical extrusion. J Endod. 2005;31:533–5. doi: 10.1097/01.don.0000152294.35507.35. [DOI] [PubMed] [Google Scholar]
- 12.Myers GL, Montgomery S. A comparison of weights of debris extrudedlapically by conventional filing and canal master techniques. Endod. 1991;17:275–9. doi: 10.1016/S0099-2399(06)81866-2. [DOI] [PubMed] [Google Scholar]
- 13.Ferraz CC, Gomes NV, Gomes BP, Zaia AA, Teixeira FB, Souza-Filho FJ. Apical extrusion of debris and irrigants using two hand three engine-driven instrumentation techniques. Endod J. 2001;34:354–8. doi: 10.1046/j.1365-2591.2001.00394.x. [DOI] [PubMed] [Google Scholar]
- 14.Beeson T, Hartwell G, Thornton J, Gunsoiley J. Comparison of debris extruded apicaliy in straight canals: Conventional filing versus Profile. 04 Taper series 29. J Endod. 1998;24:18–22. doi: 10.1016/S0099-2399(98)80206-9. [DOI] [PubMed] [Google Scholar]
- 15.Goering AC, Michelich RJ, Schultz HH. Instrumentation of root canals in molars using the step-down technique. J Endod. 1982;8:550–4. doi: 10.1016/S0099-2399(82)80015-0. [DOI] [PubMed] [Google Scholar]
- 16.Zarrabi MH, Bidai M, Jafarzadeh H. An in vitro comparative tudy of apicaliy extruded debris resulting from conventional and three rotary (ProFile, RaCe, FlexMaster) instrumentation tech-niques. J Oral Sci. 2006;48:85–8. doi: 10.2334/josnusd.48.85. [DOI] [PubMed] [Google Scholar]