

Abstract
Healthy sexual functioning plays an essential role in maintaining the harmony and happiness in marital life. It provides a media to express love, which is the base for all sorts of creative activities. The absence of this function hampers the marital relationship, leading to frustration and, sometimes, ending in divorce, and causes inadequacy in performing the routine duties. In this study, 53 patients having diabetes mellitus were surveyed to find out the incidence of erectile dysfunction (ED). Considering the high prevalence of the disease and the need to look for alternative medicine, a clinical trial on 44 patients of ED was carried out. These patients were divided into two main groups: diabetic and non-diabetic, and were further divided into two subgroups as trial group and placebo group. In the trial group, Ashvattha Kshirpaka prepared with 10 g powder of its root bark, stem bark, fruit and tender leaf buds was given twice a day. In both the diabetic and the non-diabetic subjects, Ashvattha provided encouraging results on ED as well as on seminal parameters in comparison to the placebo.
Keywords: Erectile dysfunction, Klaibya, Diabetes Mellitus, Madhumeha, Ashvattha, Ficus religiosa Linn
Introduction
Sex is a basic instinct, but sexual behavior is a learned ability. Dharma, Artha, Kama and Moksha are among the four Purusharthas – objectives of life – mentioned in Ayurveda. The achievement of each of these is the basic need of every individual. Among various phase of sexual response, the most essential is the achieving of normal erection with sufficient rigidity for penetrative intercourse, the absence of which ends in failure and dissatisfaction. This condition has been elaborately described as “Klaibya” in the Ayurvedic classics and as “Erectile dysfunction” (ED) in the modern texts. Traditionally, etiological factors of ED have been classified as organic, psychogenic or mixed. This way of classifying ED is relatively useful for organizing our intervention, although it is completely arbitrary. Strictly speaking, a penis that does not respond with an erection to an “effective” stimulation may be a consequence of what we call organic factors. However, every ED problem is “psycho-organic,” because it affects the man as a whole (both physically and psychologically) as well as his partner and the couple's relationship. The incidence of ED is increasing day by day with the increase in the incidence of diabetes, hypertension, peripheral vascular disorders, peripheral neuropathy, anxiety, stress, depression and their medications. However, no direct reference is available in the Ayurvedic classics to say that Madhumeha leads to Klaibya. Of course, Vagbhatta has mentioned Mushka Avadarana[1] and Vrishana Avadaranam and Bastimedhratoda[2] as complications of Prameha. Charaka has mentioned Daurbalya as a complication of Madhumeha.[3] Among the 10 dushyas of Prameha, Shukra is one, and its dushti ultimately leads to Klaibya. ED is also increasing due to the changes in the lifestyle and increased addictions, particularly smoking. Hence, it is the need of the hour to conduct researches in finding out safe, easily available, economic and potent medicines for the management of ED. Ashvattha (Ficus religiosa) is such a type of easily available herb that can be found throughout India. Sushruta has mentioned its aphrodisiac effect in men.[4] It is used as Pumsavana in Atharva Veda (A. V., 6/2/11/1). Here, Pumsavana does not mean only to get male child, rather it is related to get the desired sex in the baby. In that way, it may also strengthen the men's genital organs to have qualitative and quantitative development in the Shukra without which we cannot get a male child. It also has hypoglycemic[5,6] and hypolipidaemic[7] activity. Hence, the drug was selected to manage the ED in both diabetic and non-diabetic subjects.
Aims and Objectives
-
i)
Survey the patients of diabetes mellitus (DM) to see the incidence of ED (Klaibya).
-
ii)
Study the etiopathogenesis of the ED in DM.
-
iii)
evaluate the effect of Ashvattha on ED in diabetic and non-diabetic subjects.
Materials and Methods
A total of 44 patients fulfilling the diagnostic criteria of Klaibya (ED) as per the International Index of Erectile Function (IIEF)-15 questionnaire[8] with or without DM were selected from the OPD and IPD of I.P.G.T. and R.A. Hospital, Gujarat Ayurved University, Jamnagar, irrespective of religion, cast, occupation, etc.
Inclusion criteria
-
i)
Male married patients suffering from ED with or without DM.
-
ii)
Age between 21 and 60 years.
Exclusion criteria
-
i)
Age below 21 years and above 60 years.
-
ii)
Unmarried patients.
-
iii)
Patients suffering from sexually transmitted diseases, carcinoma, acquired immunodeficiency syndrome, tuberculosis, congenital abnormalities of genital organs, other disease like phimosis, ulceration, hydrocele, spinal cord lesions, etc.
Investigations
-
i)
Routine hematological investigations: Hemoglobin %, Total Leucocyte count, Differential Leucocyte count,Erythrocyte Sedimentation Rate
-
ii)
Biochemical investigations: Fasting Blood Sugar, Post Prandial Blood Sugar, lipid profile, blood urea, serum creatinine.
-
iii)
Urine for routine and microscopic examination.
-
iv)
Semen analysis.
-
v)
Bio markers: serum testosterone, serum Dehydroepiandrosterone Sulfate (DHEA-S)
Concomitant medication
-
i)
Patients having DM were allowed to continue their anti-diabetic drugs during the course of treatment.
-
ii)
Psychological counseling therapy was given in all the patients.
Criteria for assessment
Subjective criteria:
-
a)
Relief in the subjective parameters of ED mainly.
-
b)
Relief in the subjective parameters as per the International Index of Erectile Function (IIEF) questionnaire.
-
c)
Relief in the subjective parameters of associated sexual dysfunctions and other symptoms were also considered to support the main finding and to assess the total effect of the therapy.
Objective criteria
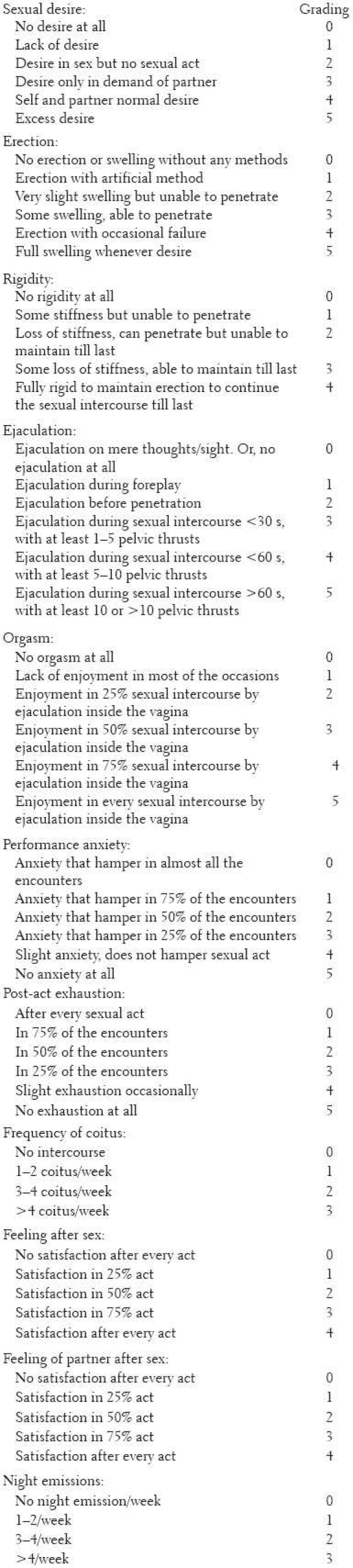
The special scoring system for sexual parameters in male,[9] used in the Vajikarana Lab I.P.G.T. and R.A., with some modifications, was adopted for the statistical analysis of the overall effect of the therapy on different sexual parameters as under;
Drug and Schedule of Administration
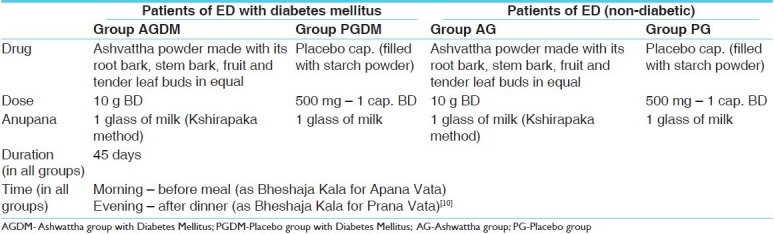
The drug and dose schedule is shown in Table 1.
Table 1.
Drug, Dose schedule and grouping
Total effect of the therapies
The total effect of the therapies was assessed on the basis of relief in the major symptoms. The score of each and every symptom before and after the treatment was calculated for grading followed by the overall percentage of improvement of each patient by the formula:

The equation is Total BT - Total AT upon Total BT into 100
The obtained results were measured according to the grades given below:
Complete remission: 100 % relief in major complaints.
Markedly improved: 75–99% relief in major complaints.
Moderately improved: 50–74% relief in major complaints.
Mildly improved:25–49% relief in major complaints.
Unchanged: <25% or no relief in major complaints.
Statistical analysis
The information gathered on the basis of observation made about various parameters was subjected to statistical analysis in terms of mean, standard deviation (SD) and standard error (SE). Students paired “t”-test was applied for the statistical significance. The results were interpreted at P <0.05, P <0.01 and P <0.001 significance levels. The obtained results were interpreted as: insignificant – P >0.05; significant – P <0.05; highly significant – P <0.01.
Observations and Results
Survey study
The survey of 53 diabetic males showed that 69.81% of the patients had ED, with 24.53% having severe ED, 22.64% having moderate ED and 11.32% each having mild to moderate and mild ED. It revealed that age and chronicity of DM were directly related to the severity of ED.
Clinical study
A majority of the Klaibya patients (52.27%) were in the age group of 41–50 years. 75.9% of the patients belonged to the Hindu religion, 61.36% were educated up to the higher secondary, 34.09% were from the employee community, 43.18% belonged to the middle class and 90.91% were living in urban areas. Cardinal symptoms include lack of rigidity (84.09%), lack of erection (77.27%), lack of rigidity till completion of sexual act (15.91%), lack of erection till the completion of sexual act (11.36%) and no erection at all (9.09%). Among them, 27.27% had chronicity above 3 years, 81.82% had gradual onset of disease, 81.82% had secondary, 75% had progressive type of disease and 79.55% had nocturnal penile tumescence positive. The associated sexual complaints were post-act exhaustion (93.18%), performance anxiety (70.45%), early ejaculation (54.55%), lack of orgasm (45.45%), lack of desire (34.09%) and no orgasm at all (29.55%). Clinical interpretation of IIEF-15 shows that mild to moderate ED was reported in 40.91% of the patients, mild dysfunction in 27.27%, moderate dysfunction in 20.45% and severe dysfunction in 11.36% of the patients. Associated symptoms observed were anxiety (75%), stress (52.27%), depression (34.09%), Agnimandya (29.55%), Swedadhikya and Atidaurbalya (20.45% each), Bhrama and sleeplessness (18.18% each), Tamodarshana (15.91%), Trishnadhikya, Hastapada Daha and Tachypnoea (13.64% each), Shiroruk (11.36%), palpitation (9.09%), Tandra, Avila Mutrata, Kshudha Adhikya and bodyache (6.82% each), Aruchi, Kampa and Vaivarnya (4.55% each) and Tikta Amlodgara and backache (2.27% each).
Nidanarthakara Rogas like hyperlipidemia (47.73%) DM (34.09%), Karshya (27.27%), hypertension (22.73%), Sthaulya (15.91%), psychological disorders (13.64%), Pandu (9.09%), peripheral neuropathy (6.82%), Ischemic heart disease (4.55%) and peripheral vascular disease and Grahani (2.27% each) were found, in which ED was seen as a complication. Maximum patients possessed Samagni (52.27%), Madhyama Kostha (70.45%), regular bowel habit (81.82%), normal micturition (68.18%), consuming vegetarian diet (77.27%) with Madhyama quantity (81.82%), having proper sleep (72.73%), addicted to tobacco chewing (36.36%), did not perform any sort of exercise (68.18%), having anxious mood (45.45%), happy home-life (56.82%), good relation with wife (59.09%), had attained normal puberty (70.45%), less knowledge of sex (61.36%), masturbatory history before marriage (81.82%), weakness and fatigue due to masturbation (56.82%), believed that masturbation leads to sexual dysfunction (52.27%), having no premarital affairs (77.27%), interact with their partner lovingly (63.64%), had good mutual attraction (90.90%), successful result of first night after marriage (79.55%), indulged positively in sexual intercourse (61.36%), understanding (90.91%) and cooperative (84.09%) type of attitude of the partner, mild contribution toward present illness (38.64%) and sexual goal of satisfaction of self as well as of partner (43.18%). The maximum number of patients had Vata-Pitta Sharira Prakriti (38.64%), Satva-Tamas Manasa Prakriti (38.64%), Madhyama Sara (72.73%), Madhyama Samhanana (90.91%), Madhyama Pramana (54.55%), Madhyama Satmya (56.82%), Madhyama Sattva (54.55%) and Avara Vyayama Shakti (61.36%).
Enquiring about the dietary habits as a causative factor, it was revealed that maximum patients (54.55%) consumed an incompatible diet, Katu Rasa (50%), Lavana Rasa in excess (45.45%), Kshara (43.18%), Shita Guna dominance (38.64%), Amla Rasa (36.36%), Ruksha Bhojana (34.09%), Asatmya Ahara (31.82%), Ajirna Bhojana (25%), Vishamasana (20.45%), Alpa Bhojana (13.64%), late meal in the night (11.36%) and Anasana (2.27%). Among the lifestyle-related factors, Shrama (25%), Ati Vyavaya (22.73%), Abhichara (20.45%) and Shukra Vega Nirodha (6.82%) were commonly found. Mental health disturbance includes anxiety (75%), fear (70.45 %), worry (54.55%), Ksubdhamana (34.09%), Moha (Agyana) (15.91%), anger (13.64%), Traasa (13.64%), Istasya Alabhata (6.82%), no interest in his wife (4.55%) and Utkantha (2.27%). Among the other causes, in Dosha Dushti, the maximum number of patients had symptoms of Vata Prakopa (77.27%), Dhatu Vaishamya (all patients having Shukra Kshaya, Rasa Kshaya; 70.45%), Majja Kshaya (20.45%), Mamsa Kshaya (13.64%), Rakta Kshaya (11.36%), Meda Kshaya (11.36%), Meda Vriddhi (54.55%), Rasa Vriddhi (27.27%) and Majja Vriddhi (18.18%). In Ojas Vaishamya, Vishramsa (70.45%), Vyapat (31.82%) and Kshaya (2.27%) were found. Sroto Dushti involves the impairment of the function of Shukravaha (100%), Rasavaha (97.73%), Medovaha (52.27%), Mutravaha (31.82%), Majjavaha (20.45%), Swedavaha (20.45%), Pranavaha (15.91%), Udakavaha (15.91%), Annavaha (9.09%), Purishavaha (9.09%) and Raktavaha (6.82%) Srotas.
Effect of Therapy
ED in non-diabetics
A total of 21 patients were treated with Ashvattha and eight patients were studied on placebo as under:
Penile erection
Statistically highly significant (P < 0.001) increase (17.86%) was observed in test drug group with non-significant (P > 0.1) increase (3.85%) by placebo in the penile erection.
Penile rigidity
Ashvattha increased the penile rigidity by 48.65%, which was statistically highly significant (P < 0.001), while in the placebo group the penile rigidity increased only by 5.56%, which was insignificant (P > 0.1).
Sexual desire
Placebo failed to show any effect on the sexual desire while a statistically insignificant effect (P > 0.1) was exhibited in the Ashvattha-treated group, which increased the sexual desire by 10%. Here, both the groups showed insignificant results.
Early ejaculation
Ashvattha showed a highly significant (P < 0.001) improvement (21.15%) while the placebo had only 3.71% relief, which was significant (P > 0.1). Thus, the test drug has a better effect on the ejaculation score.
Orgasm
Highly significant (P < 0.001) improvement (133.33%) was found in orgasm (sexual enjoyment) by Ashvattha while the placebo had only 16.67% relief, which was statistically insignificant (P > 0.1).
Performance anxiety
Ashvattha reduced the performance anxiety by 33.33%, which was statistically highly significant (P < 0.001), while placebo reduced the performance anxiety only by 5.58%, which was insignificant (P > 0.1).
Post-act exhaustion
In the Ashvattha-treated group, there was a highly significant (P < 0.001) improvement (33.33%), while in the placebo group, the improvement was insignificant (11.11%). The test drug had a superior effect on the post-act exhaustion.
Self-satisfaction
Self-satisfaction was improved (207.69%) in the Ashvattha-treated group, which was statistically highly significant (P < 0.001), while with the placebo, non-significant (P > 0.1) improvement (66.67%) was reported.
Partner's satisfaction: Satisfaction of the partner after sex was improved (150%) in the Ashvattha-treated group, which was statistically highly significant (P < 0.001), while with placebo, non-significant (P > 0.1) improvement (66.67%) was reported. Here, the test drug has shown better improvement on self and partner's satisfaction after intercourse.
IIEF parameters
In IIEF scoring, Ashvattha showed a highly significant (P < 0.001) improvement in erectile function (28.86%) and intercourse satisfaction (53.61%), significant (P < 0.05) improvement in orgasm function (12.5%) and non-significant (P > 0.1) improvement in the overall satisfaction (6.06%), while there was no change in sexual desire. On the other hand, with placebo, non-significant improvement was observed in erectile function (1.42%, P > 0.1) and intercourse satisfaction (11.91%, P > 0.05) and there was no improvement in orgasm, sexual desire and overall satisfaction. Thus, Ashvattha has a better effect on IIEF scoring in comparison to placebo due to its Vrishya properties.
Biochemical parameters
The changes in all biochemical parameters after taking Ashvattha (AG) and placebo (PG) were statistically insignificant (P > 0.1), as below:
FBS (AG: 0.79%↑, PG: 7.18%↓), PPBS (AG: 5.05%↓, PG: 12.89%↓), serum cholesterol (AG: 0.91%↑, PG: 3.33%↑), serum triglycerides (AG: 10.26%↓, PG: 1.3%↓), HDL (AG: 6.22%↑, PG: 1.86%↑), blood urea (AG: 4.09%↑, PG: 21.43%↑), serum creatinine (AG: 1.61%↑, PG: 3.28%↓), serum testosterone (AG: 22.12%↑, PG: 7.54%↑), serum Dehyderoepiandrosterone-sulphate (DHEA-S) (AG: 0.53%↑, PG: 1.16%↑).
Hematological parameters: Statistically insignificant (P > 0.1) changes were found in all the hematological parameters, viz. TC, DC, Hb% and ESR after taking Ashvattha and placebo.
Effect on semen analysis
In both the groups, the liquefaction time was increased but was within normal limits after a course of therapy. No significant changes were found in the semen volume.
Sperm count
The patients treated with placebo showed a decrease in the sperm count (6.77%), which was statistically non-significant (P > 0.1), while the Ashvattha-treated group showed an increase in the sperm count (21.22%) when compared with the initial, which was statistically highly significant (< 0.001).
Sperm motility
The Ashvattha-treated group showed an increase in the total motility (24.46%), which was statistically highly significant (P < 0.001), while in the placebo-treated group, the increase in total motility was only 4.93%, which was statistically non-significant (P > 0.1). In the Ashvattha-treated group, an increase was seen in Rapid linear progressive (RLP) motility (17.85%), while in the placebo-treated group the increase in RLP motility was only 6.67%. Subsequently, Ashvattha decreased the sluggish linear progressive (SLP) and non-progressive (NP) motility. This shows that Ashvattha has a positive effect on the motility parameter of the sperms. The abnormal forms were decreased, but the finding was statistically insignificant.
Effect of therapy in diabetics
A total of 13 patients of ED with DM divided into two groups were treated with Ashvattha (n = 7) and placebo (n = 6). The results obtained on various parameters are as below:
Penile erection
Only 8.7% and 7.14% improvement was found with Ashvattha and placebo, respectively, which was statistically insignificant (P > 0.1). Here, a somewhat better result was found in the Ashvattha group than in the placebo group, but the improvement was very less.
Penile rigidity
In the Ashvattha-treated group, a highly significant (P < 0.001) increase was found in penile rigidity (42.86%), while with the placebo, it was only 9.09% and was not significant (P > 0.1). Here, Ashvattha gave superior result in rigidity.
Sexual desire
No change was found in the sexual desire (n = 2) with placebo while no patients with desire problems were found in the Ashvattha group.
Early ejaculation
Only 8.33% and 5.26% improvement was found with Ashvattha and placebo, respectively, which was statistically insignificant (P > 0.1). Here, somewhat better result was found in the Ashvattha group than in the placebo group.
Orgasm
Statistically significant (P < 0.05) improvement (100%) was found in the Ashvattha-treated group. Placebo provided a similar but statistically insignificant (P > 0.1) result in orgasm dysfunction.
Performance anxiety
Ashvattha provided 17.65% relief in performance anxiety while placebo had 16.67% relief, but both were statistically insignificant (P > 0.05 and P > 0.1).
Post-act exhaustion
In the Ashvattha-treated group, 22.22% relief was found in the post-act exhaustion, while with placebo it was 50%, but both were statistically insignificant (P > 0.1).
Self-satisfaction
Self-satisfaction was better improved (400%) in the Ashvattha-treated group, which was statistically significant (P < 0.05), while with the placebo, a non-significant (P > 0.1) improvement (100%) was reported.
Partner's satisfaction
Satisfaction of partner after sex was improved (350%) in the Ashvattha-treated group, which was statistically significant (P < 0.05), while with the placebo, a non-significant (P > 0.1) improvement (100%) was reported.
IIEF parameters
In IIEF scoring, Ashvattha showed a highly significant (P < 0.01) improvement in intercourse satisfaction (45.45%), significant (P <0 .05) improvement in erectile function (19.35%) and non-significant (P > 0.1) improvement in orgasm function (7.69%), sexual desire function (1.85%) and overall satisfaction (5%). On the other hand, with placebo treatment, a non-significant (P > 0.1) improvement was observed in erectile function (8.57%), intercourse satisfaction (21.74%), orgasm function (2.33%), sexual desire (2.38%) and overall satisfaction (3.33%). In summary, it can be said that Ashvattha has a better effect on IIEF scoring in comparison with the placebo.
Biochemical parameters
The changes found in all the biochemical parameters performed after taking Ashvattha and placebo when compared with its initial mean were statistically non-significant (P > 0.1), which are as below:
FBS
With placebo treatment, FBS was reduced by 5.79% (10.5 mg/dl), while after Ashvattha treatment, it was reduced by 3.8% (6.86 mg/dl).
PPBS
With Ashvattha treatment, PPBS was reduced by 5.10% (11.71 mg/dl), while after placebo treatment, it was reduced by 9.45% (23.5 mg/dl).
Serum cholesterol
Serum cholesterol was reduced by 6.84% (13.57 mg/dl) with Ashvattha treatment while it was reduced by only 0.98% (1.83 mg/dl) with placebo.
Serum triglycerides
With Ashvattha treatment, only 0.9% (1.57 mg/dl) increase in serum triglycerides was reported, while it was increased by 30.01% (42.17 mg/dl) with placebo.
HDL
With Ashvattha treatment, 1.87% increase in HDL was reported, while after taking placebo, it was decreased by 3.52%. By this finding, it may be said hypothetically that Ashvattha reduces bad fat and increases the good fat. However, the findings were insignificant statistically.
Serum testosterone and serum DHEA-S were decreased in the Ashvattha-treated group and were increased in the placebo group. Here again, due to the small sample size nothing, can be said conclusively. However, the increase in the placebo group was insignificant.
Hematological parameters
Regarding hemoglobin and total and differential leucocyte counts, there were no significant changes in both the groups. However, ESR in the placebo group was increased significantly; this was because only one patient showed a significant increase in ESR after treatment.
Semen analysis
No significant changes were noted in liquefaction time and semen volume after the treatment in both the groups. Even though the sperm count increased in the placebo group and decreased in the Ashvattha group, it was not statistically significant, and the sample size was also very small. Total and RLP motility were increased in both the groups. However, the SLP motility, NP motility and total abnormal forms placebo groups showed better results than the Ashvattha group.
It may be noted that one of the non-diabetic patients suffering from ED who was treated with Ashvattha had secondary infertility since 4 years due to oligozoospermia (sperm count: 12 millions/ml). After the treatment, his sperm count increased to 25 millions/ml and his wife conceived.
Untoward effect
One non-diabetic, 50-year-old patient of Kapha Prakriti having past H/o Ca-tongue and having taken chemotherapy reported itching all over body after taking Ashvattha. After its withdrawal, itching disappeared and again reappeared after taking the drug. This is important from the pharmacovigilence point of view. None of the other patients showed any untoward effect of the drug.
Overall effect of therapy
Non-diabetic subjects: In Ashvattha-treated group, 61.11% of the patients were mildly improved, 5.56% were moderately improved and the remaining 33.33% remained unchanged, whereas with the placebo, all the patients showed no change. Diabetic subjects: By Ashvattha, 57.14% of the patients had mild improvement and the remaining 42.86% remained unchanged, whereas by placebo, 16.67% of the patients had mild improvement and the remaining 83.33% remained unchanged[Figure 1].
Figure 1.
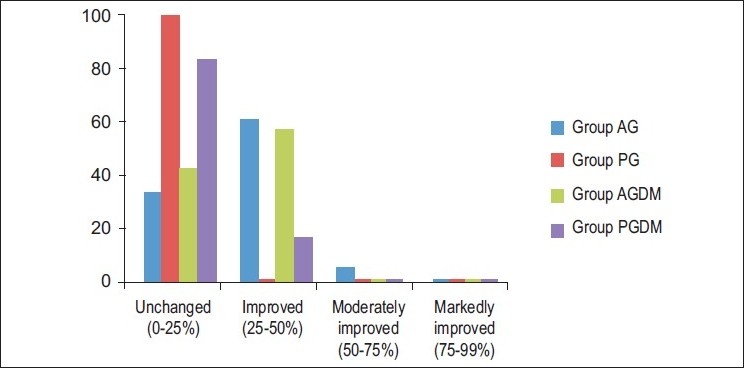
Overall effect of therapy
Discussion
Ashvattha is said to possess Kashaya Rasa, Madhura Anurasa, Guru, Shita, Ruksha and Durjara Guna, Katu Vipaka and Shita Virya. The effect of Ashvattha in the improvement of erection and rigidity may be because of its Vrishya property by the virtue of Guru Guna. The Guru Guna has been mentioned as one among the six qualities of Vrishya Dravya by Charaka (Cha. Chi. 2/4/36). The aphrodisiac effect of Ashvattha is also described in the texts. The better effect on ejaculation score may be because of Stambhaka effect due to its Shita Guna and Kashaya Rasa. This acts as Shukra Stambhana and prevents premature ejaculation. The results found in orgasm and performance anxiety score may be due to its Shita Virya, cooling property and because of good performance by improvement in erection and ejaculation and by psychological counseling. The effect on post-act exhaustion may be due to the Guru Guna and Balya property of the test drug. Improvement on self and partner's satisfaction after intercourse may be because of improvement in erection, rigidity and the time of ejaculation. Moreover, the psychotherapy provided by the counseling also plays an important role in the satisfaction. The percentage-wise improvement in serum testosterone and serum DHEA-S may be due to its Shukra Vriddhikara Vrishya property, as these male androgens are being correlated with Sarva Shariragata Shukra. However, these results were statistically insignificant. Here, Guru and Shita Guna are similar to the properties of Shukra (Cha. Chi. 2/4/50). Here, the Shukra Vriddhikara Vrishya effect due to its Guru Guna and Shita Virya might have increased the sperm count. Ashvattha had caused mild increase in serum testosterone and DHEA-S levels, and testosterone stimulates sertoli cells to secrete paracrine agents that stimulate sperm proliferation and differentiation.[11] The effect of Ashvattha on total motility and RLP motility may be due to its zinc content. Zinc is one of the contents in seminal plasma[12,13] and its role in increasing the motility is proven by modern researches.[14] It is an important micronutrient in many enzyme systems in the body and takes part in metabolism of protein, fat and carbohydrate. It is also a component of insulin, growth hormone and antioxidant enzymes.[15] The results found in diabetics were lower than those in non-diabetics because of the complex etiology of neurogenic, vasculogenic and endocrinal factors of diabetes. No encouraging result was found in the post-act exhaustion, which may be because of the additional debility due to diabetes in these patients. It cannot be concluded that placebo has a better effect than Ashvattha in reducing the blood sugar level because of a smaller sample size. Moreover, one patient among the six patients of the placebo group was a newly diagnosed case of DM, with high blood sugar levels. He was advised strict diet restriction due to which the post-treatment blood sample showed drastic reduction in the blood sugar levels. This single patient's result contributed to the overall better effect of the placebo group than in the treated group. Serum cholesterol and serum triglycerides were both reduced with Ashvattha, which may be due to its hypolipidemic effect, Kashaya Rasa, Ruksha Guna and Medohara properties. Other minerals and trace elements found in Ashvattha, like calcium, iron, copper and manganese are very much constructive for a healthy state. From these, it is clear that in both the diabetic and the non-diabetic patients, Ashvattha provided better improvement in comparison with the placebo.
Conclusion
Diabetes is one of the most common physical causes of ED associated with reduced quality of life among those affected. The etiology of diabetic impotence is complex, with neurogenic, vasculogenic and disordered local neuroeffector regulatory mechanisms contributing to the pathology of ED. A survey study reveals that ED is more common in DM, and with advancement of age and chronicity of the disease, the severity of ED increases. Socioenvironmental factors like distressed relationships, adverse life experiences, major financial crisis, bereavement and psychological stress have a profound influence on the mind and are capable of causing psychogenic ED. It seems that ED in diabetics is more difficult to cure in comparison with ED in non-diabetic subjects. Ashvattha showed a highly significant increase in total sperm count and total motility in non-diabetic subjects. Thus, it is a new addition in the list of Shukra Vriddhikara Vrishya drugs. It can be used in treating Oligoasthenozoospermia. On the basis of the results obtained, it can be concluded that Ashvattha is far better in comparison with the placebo in providing better cure to the patients of ED (Klaibya).
References
- 1.23. Vol. 10. Chaukhambha publication; 2000. Ashtanga Hridaya with Ayurveda Rasayana and Sarvanga Sundari Comm, Nidana Sthana; p. 504. [Google Scholar]
- 2.17. Vol. 10. Nidana Sthana: 1980. Ashtanga samgraha, Athavale AD with Indu commentary published by Athvale MA. [Google Scholar]
- 3.Trikamji Yadavji., editor. 48. Vol. 4. Varanasi,Nidana Sthana: Chaukhambha publication; 2005. Charaka Samhita comm. Chakrapani; p. 215. [Google Scholar]
- 4.Susruta Samhita Nibandha Samgraha commentary by Dalhan, Chaukhambha Sanskrit Sansthan, Varanasi Chikitsa sthana. 26(27):498. [Google Scholar]
- 5.Ambike S H, Rao MRR. Studies on a phytosterolin from the bark of Ficus reliogosa. Indian J Pharm. 1967;29:91–4. [Google Scholar]
- 6.Brahmachari HD, Augasti KT. Orally effective hypoglycemic agents. J Pharmacy Pharmaco. 1962;14:254. doi: 10.1111/j.2042-7158.1962.tb11089.x. [DOI] [PubMed] [Google Scholar]
- 7.Agarwal V, Chauhan BM. A study on composition and hypolipidemic effect of dietary fibres from some plant foods. Plant foods and Human Nutrition. 1988;38:189. doi: 10.1007/BF01091723. [DOI] [PubMed] [Google Scholar]
- 8.Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF) a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–30. doi: 10.1016/s0090-4295(97)00238-0. [DOI] [PubMed] [Google Scholar]
- 9.Mehra BL, Skandhan KP, Singh G. studies on Klaibya (male sexual dysfunctions) and its management with Vajikarana. 1995. In: Bhatted S, Singh G, Thakar A, editors. Acomparative study of the role of Vajikarana drugs administered orally and by Basti in the management of Klaibya with reference to Erectile Dysfunction, Sp. Panchkarma, Department Kayachikitsa, Gujarat Ayurvedic Uni. Jamnagar. 2002. [Google Scholar]
- 10.Tripathi B, editor. 2nd. Varanasi: Samskarana, Chaukhambha Surabharati Prakasana; 2004. Sharangadhara. Dipika Hindi Vyakhya Sahita, Anjananidana Sahita. [Google Scholar]
- 11.Vander . Human Physiology: The Mechanism of Body Function. In: Vander A, Sherman J, Luciano D, editors. 8th ed. Columbus, OH, USA: McGraw-Hill; 2001. p. 644. ISBN: 0072908017. [Google Scholar]
- 12.Andrews JC, Noland JP, Hammerstedt RH, Bavister BD. Role of zinc in hamster sperm capacitation. Biol Reprod. 1994;51:1238–47. doi: 10.1095/biolreprod51.6.1238. [DOI] [PubMed] [Google Scholar]
- 13.De Lamirande E, Leclerc P, Gagnon C. Capacitation as a regulatory event that primes spermatozoa for the acrosome reaction and fertilization. Mol Human Reprod. 1997;3:175–94. doi: 10.1093/molehr/3.3.175. [DOI] [PubMed] [Google Scholar]
- 14.Henkel RR. Estimate of oxygen consumption and intracellular zinc concentration of human spermatozoa in relation to motility. Asian J Androl. 2003;5:3–8. [PubMed] [Google Scholar]
- 15.Vaughan JG, Judd PA, editors. Oxford: Oxford University Press; 2003. The Oxford Book of Health Foods. [Google Scholar]