

Abstract
Background/Aim:
To determine the mortality rate in a cohort of hospitalized patients with cirrhosis and examine their resuscitation status at admission.
Materials and Methods:
A retrospective chart review was conducted of patients with cirrhosis who were admitted to a tertiary care hospital in Riyadh, Saudi Arabia, from January 1, 2009, to December 31, 2009.
Results:
We reviewed 226 cirrhotic patients during the study period. The hospital mortality rate was 35%. A univariate analysis revealed that worse outcomes were seen in patients with advanced age or who had worse child-turcotte-pugh (CPT) scores, worse model for end-stage liver disease (MELD) scores, low albumin and high serum creatinine. Using a multivariate analysis, we found that advanced age (P=0.004) and high MELD (P=0.001) scores were independent risk factors for the mortality of cirrhotic patients. The end-of-life decision were made in 34% of cirrhotic patients, and the majority of deceased patients were “no resuscitation” status (90% vs. 4%, P<0.001).
Conclusions:
The relatively high mortality in cirrhotic patients admitted for care in a tertiary hospital, Saudi Arabia was comparable to that reported in the literature. Furthermore, end-of-life discussions should be addressed early in the hospitalization of cirrhotic patients.
Keywords: Cirrhosis, MELD score, mortality
Cirrhosis is a major global health problem, especially in Saudi Arabia.[1] This is attributed to the relatively high prevalence of viral hepatitis in this country.[2–5] Cirrhosis is the leading cause of death in Asia.[6] In USA, cirrhosis ranks as the tenth most common cause of death.[1] An objective and reproducible scoring system for the severity of liver disease is important for predicting mortality in patients with cirrhosis in general or with specific complications of cirrhosis.[7]
The child–turcotte–pugh (CTP) scoring system was initially developed to evaluate the risk of surgical portosystemic shunt procedures and was subsequently found to predict the long-term survival of cirrhotic patients.[8] However, this classification was developed in the last century and may no longer be accurate, given advances in medical care and technology.[8] A more recently developed prognostic scoring system for patients with cirrhosis, the model for end-stage liver disease (MELD), was developed for selecting cirrhotic patients for shunting.[8,9] The MELD scoring system has been extended to prognosticate for patients with complications of cirrhosis.[7]
The objective of our study was to determine the in-hospital mortality rate among a cohort of hospitalized cirrhotic patients and to evaluate their end-of-life decision during hospital admission.
MATERIALS AND METHODS
Study population
A retrospective chart review was conducted for patients with discharge ICD-9 diagnosis codes corresponding to cirrhosis who were admitted to a tertiary care hospital in Riyadh, Saudi Arabia, from January 1, 2009, to December 31, 2009. These patients were adults 18 years or older who had a history and clinical presentation consistent with cirrhosis. The diagnosis of cirrhosis was based on clinical and laboratory evidence including the presence of portal hypertension, endoscopically proven esophageal varices, ascites or abnormal liver function and coagulopathy and/or a liver biopsy showing cirrhosis. The study was approved by the King Abdullah International Medical Research Center and the institutional review board (IRB) of the hospital. The approval allowed for a retrospective chart review without informed consent.
Data collection
The following information was collected from each chart: age, gender, admission creatinine, international normalized ratio (INR), bilirubin, albumin, platelet counts, etiology of cirrhosis (viral hepatitis, alcoholic, autoimmune or cryptogenic), CTP score, MELD score and outcomes were calculated. Patients were followed up until discharge from the hospital or until death, whichever was earlier.
Outcome measures
The outcomes evaluated were the hospital mortality and resuscitation status of hospitalized cirrhotic patients.
Statistical analysis
Continuous data were expressed as means ± standard deviations (SD) and were compared using student's t-test. Categorical data were expressed as percentages and compared using a Chi-square test. Statistical significance was defined as a P value less than 0.05. Statistical analysis was performed using Minitab for Windows (release 13.1).
RESULTS
Demographic and clinical characteristics
Over one year, 226 cirrhotic patients were hospitalized. One hundred and forty eight (65%) patients survived, and were discharged from the hospital. The mean age was significantly higher in the non-survivor group (64.4 vs. 59.9, P < 0.05). There was no significant difference in gender between survivors and non-survivors. There was a trend toward increased hospital length of stay (LOS) in the non-survivor group compared to survivors (11 days vs. 14.7 days, P < 0.06) [Table 1]. The main indication for hospitalization was infection, and there was no significant difference between the two groups regarding the reason for hospitalization [Table 2].
Table 1.
Baseline characteristics of hospitalized cirrhotic patents
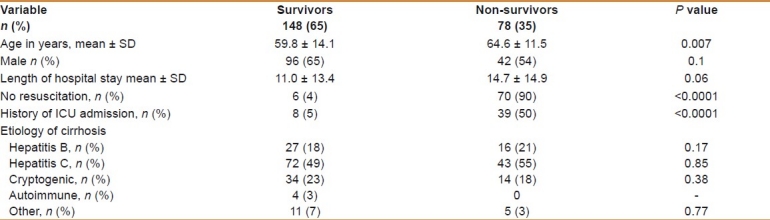
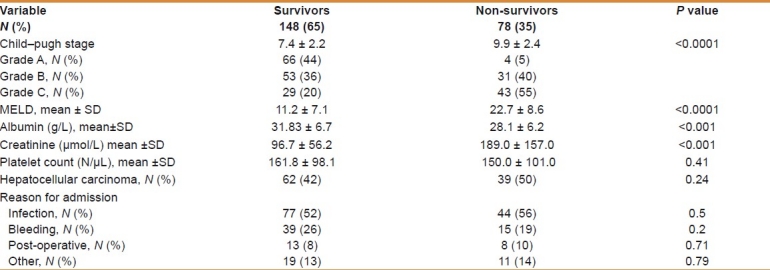
Table 2.
Univariate analyses of factors associated with hospital mortality
The hospital outcome
Out of 226 hospitalized patients, 78 (35%) died.
The predictors of outcome
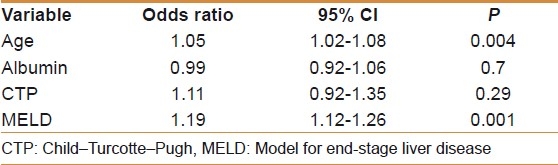
The ICU admission (50% vs. 5%, P < 0.001), MELD score (22.7 vs. 11.2%, P <0.001) CTP score (9.9 vs. 7.4, P < 0.001) and albumin (31.8 vs. 28.1%, P < 0.001) were all significantly higher in the non-survivor group. However, there was no significant difference between the two groups regarding platelet count or history of hepatocellular carcinoma. In a univariate analysis, worse outcomes were seen in patients with advanced age, worse CTP scores, worse MELD scores, low albumin and high serum creatinine [Table 2]. These factors were analyzed by multivariate analysis, which revealed that high MELD score and advanced age were independent risk factors for mortality [Table 3].
Table 3.
Multivariate logistic regression of variables of factors associated with hospital mortality
Resuscitation status
The majority of non-survivor had a “no resuscitation” status versus survival patients (90% vs. 4%, P < 0.001).
DISCUSSION
The present study showed that the hospital mortality rate of hospitalized cirrhotic patients was 35%. These results confirm the findings of a recent study from Tunisia where viral etiology, the most common underlying cause of cirrhosis, they found the hospital mortality was 20% and 48% during follow-up for a mean period of 22 months.[10] We found that high MELD score and advanced age were independent predictors of mortality. The MELD scoring system is based on the objective variables leading to a fine grading system.[7,11] The MELD score has limitations: it does not include indicators of poor prognosis in cirrhotic patients such as malnutrition and portal hypertension, and it fails to accurately predict mortality in 15 to 20% of patients with cirrhosis.[7] On the other hand, the CTP classification originated more than two decades ago and may no longer be accurate, given the marked advancements in management and medical technology since its introduction.[8] In addition to the three objective variables, the CTP score incorporates the two subjective variables of ascites and severity of encephalopathy, which leads to a coarse grading system. Advanced age was also found to be an independent risk factor for mortality; this may be due to factors that we did not consider, such as coronary artery disease, type of infection, diabetes mellitus and/or cerebrovascular hemorrhage. Actually these scores were initially developed to evaluate the risk of surgical portosystemic shunt procedures and predictor of mortality among patients on the waiting list for liver transplantation.[8] Based on the available data, none of the scoring systems were able to demonstrate satisfactory predictive accuracy.[8,12] In practice, no single tool is able to predict outcomes, and experienced physicians use their knowledge to make expert and informed clinical judgments.[13] In one study, the ICU mortality rate was 83%, and regardless of the reason for admission (related to cirrhosis or not), cirrhosis independently worsened the prognosis of patients admitted to the ICU.[14] The values of the liver disease-specific scores calculated at ICU admission were likely to be altered by concomitant extrahepatic organ failure.[14] Similar ICU findings were reported by Arabi et al, in a study conducted in the same institution, they found that there was no difference between predicted mortality and actual mortality.[13] The majority of cirrhotic patients admitted to the hospital were “full resuscitation.” A subanalysis of the SUPPORT study found that more than two-thirds of cirrhotic patients preferred full resuscitation, but the number of DNR orders increased near death.[15] A prospective cohort study found that one-third of hospitalized cirrhotic patients had severe functional limitations two months after hospitalization.[16] Moreover, the outcomes of hospitalized cirrhotic patients were found to be poor[17–19] and should encourage the use of various new antiviral agents and the advent of liver transplantation, both of which increase the possibility of long-term survival.[8] Decision making is frequently limited by the nature of the disease, the availability of treatment and the prognosis. Despite similar prognoses, patients with cirrhosis have been shown to be less likely to have a “no resuscitation” order than patients with lung cancer or AIDS, and this could be due to misunderstandings between the clinician, the patient and the family.[20] In the oncology literature reports that patients often have optimistic misperceptions of their prognosis and frequently request medical therapies that most physicians would consider futile.[21,22] These findings suggest that the discrepancy between patients and physicians regarding the issue of prognosis may be related to physician nondisclosure or optimistic disclosure.[22] In recent years, increased attention has been given to medical decisions at the end of life.[23] We should integrate the goals of care discussions and documentation into our practices and medical school curricula.[23]
The present study had several limitations, including that it was conducted at a single center; the nature of a retrospective study may have influenced the interpretation of our result and could not assess some potentially significant predictors of outcome (e.g. reversible processes such as pneumonia) because no standard protocol was followed in treating the patients. In addition, most importantly, the sample size was not large.
CONCLUSION
Our findings show that the hospital mortality of cirrhotic patients is high and comparable to that reported in the literature. Discussions regarding resuscitation status and end-of-life decisions should occur early in the hospitalization of cirrhotic patients
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Mansoor I. Experience of liver disease at a University Hospital in Western Saudi Arabia. Saudi Medical J. 2002;23:1070–3. [PubMed] [Google Scholar]
- 2.El Beltagy KE, Al Balawi IA, Almuneef M, Memish ZA. Prevalence of hepatitis B virus markers among blood donors in a tertiary hospital in Tabuk, northwestern Saudi Arabia. Int J Infect Dis. 2008;12:495–9. doi: 10.1016/j.ijid.2008.01.010. [DOI] [PubMed] [Google Scholar]
- 3.Madani TA. Hepatitis C virus infections reported over 11 years of surveillance in Saudi Arabia. Trans R Soc Trop Med Hyg. 2009;103:132–6. doi: 10.1016/j.trstmh.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 4.Memish ZA, Knawy BA, El-Saed A. Incidence trends of viral hepatitis A, B, and C seropositivity over eight years of surveillance in Saudi Arabia. Int J Infect Dis. 14:e115–20. doi: 10.1016/j.ijid.2009.03.027. [DOI] [PubMed] [Google Scholar]
- 5.Shobokshi OA, Serebour FE, Al-Drees AZ, Mitwalli AH, Qahtani A, Skakni LI. Hepatitis C virus seroprevalence rate among Saudis. Saudi Med J. 2003;24(Suppl 2):S81–6. [PubMed] [Google Scholar]
- 6.Fashir B, Sivasubramaniam V, Al Momen S, Assaf H. Pattern of liver disease in a Saudi patient population: A decade of experience at security forces hospital, Riyadh, KSA. Saudi J Gastroenterol. 1996;2:50–2. [PubMed] [Google Scholar]
- 7.Al Sibae MR, Cappell MS. Accuracy of MELD scores in predicting mortality in decompensated cirrhosis from variceal bleeding, hepatorenal syndrome, alcoholic hepatitis, or acute liver failure as well as mortality after non-transplant surgery or TIPS. Dig Dis Sci. 2011;56:977–87. doi: 10.1007/s10620-010-1390-3. [DOI] [PubMed] [Google Scholar]
- 8.Cho HC, Jung HY, Sinn DH, Choi MS, Koh KC, Paik SW, et al. Mortality after surgery in patients with cirrhosis: Comparison of Child-Turcotte-Pugh, MELD and MELDNa score. Eur J Gastroenterol Hepatol. 2011;23:51–9. doi: 10.1097/MEG.0b013e3283407158. [DOI] [PubMed] [Google Scholar]
- 9.Malinchoc M, Kamath PS, Gordon FD, Peine CJ, Rank J, ter Borg PC. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology. 2000;31:864–71. doi: 10.1053/he.2000.5852. [DOI] [PubMed] [Google Scholar]
- 10.Ouakaa-Kchaou A, Belhadj N, Abdelli N, Azzouz M, Ben Mami N, Dougui MH, et al. Survival in cirrhosis. Tunis Med. 2010;88:804–8. [PubMed] [Google Scholar]
- 11.Child CG, Turcotte JG. Surgery and portal hypertension. Major Probl Clin Surg. 1964;1:1–85. [PubMed] [Google Scholar]
- 12.Boursier J, Cesbron E, Tropet AL, Pilette C. Comparison and improvement of MELD and Child-Pugh score accuracies for the prediction of 6-month mortality in cirrhotic patients. J Clin Gastroenterol. 2009;43:580–5. doi: 10.1097/MCG.0b013e3181889468. [DOI] [PubMed] [Google Scholar]
- 13.Arabi Y, Ahmed QA, Haddad S, Aljumah A, Al-Shimemeri A. Outcome predictors of cirrhosis patients admitted to the intensive care unit. Eur J Gastroenterol Hepatol. 2004;16:333–9. doi: 10.1097/00042737-200403000-00014. [DOI] [PubMed] [Google Scholar]
- 14.Das V, Boelle PY, Galbois A, Guidet B, Maury E, Carbonell N, et al. Cirrhotic patients in the medical intensive care unit: Early prognosis and long-term survival. Crit Care Med. 38:2108–16. doi: 10.1097/CCM.0b013e3181f3dea9. [DOI] [PubMed] [Google Scholar]
- 15.Roth K, Lynn J, Zhong Z, Borum M, Dawson NV. Dying with end stage liver disease with cirrhosis: insights from SUPPORT.Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. J Am Geriatr Soc. 2000;48(5 Suppl):S122–30. [PubMed] [Google Scholar]
- 16.Wu AW, Damiano AM, Lynn J, Alzola C, Teno J, Landefeld CS, et al. Predicting future functional status for seriously ill hospitalized adults. The SUPPORT prognostic model. Ann Intern Med. 1995;122:342–50. doi: 10.7326/0003-4819-122-5-199503010-00004. [DOI] [PubMed] [Google Scholar]
- 17.Saunders JB, Walters JR, Davies AP, Paton A. A 20-year prospective study of cirrhosis. Br Med J (Clin Res Ed) 1981;282:263–6. doi: 10.1136/bmj.282.6260.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Propst A, Propst T, Zangerl G, Ofner D, Judmaier G, Vogel W. Prognosis and life expectancy in chronic liver disease. Dig Dis Sci. 1995;40:1805–15. doi: 10.1007/BF02212706. [DOI] [PubMed] [Google Scholar]
- 19.Durand F, Valla D. Assessment of prognosis of cirrhosis. Semin Liver Dis. 2008;28:110–22. doi: 10.1055/s-2008-1040325. [DOI] [PubMed] [Google Scholar]
- 20.Wachter RM, Luce JM, Hearst N, Lo B. Decisions about resuscitation: inequities among patients with different diseases but similar prognoses. Ann Intern Med. 1989;111:525–32. doi: 10.7326/0003-4819-111-6-525. [DOI] [PubMed] [Google Scholar]
- 21.Weeks JC, Cook EF, O’Day SJ, Peterson LM, Wenger N, Reding D, et al. Relationship between cancer patients’ predictions of prognosis and their treatment preferences. JAMA. 1998;279:1709–14. doi: 10.1001/jama.279.21.1709. [DOI] [PubMed] [Google Scholar]
- 22.Lamont EB, Christakis NA. Prognostic disclosure to patients with cancer near the end of life. Ann Intern Med. 2001;134:1096–105. doi: 10.7326/0003-4819-134-12-200106190-00009. [DOI] [PubMed] [Google Scholar]
- 23.Parker MH, Cartwright CM, Williams GM. Impact of specialty on attitudes of Australian medical practitioners to end-of-life decisions. Med J Aust. 2008;188:450–6. doi: 10.5694/j.1326-5377.2008.tb01714.x. [DOI] [PubMed] [Google Scholar]