

Abstract
BACKGROUND AND OBJECTIVES:
Several polymorphisms of the β2-adrenergic receptor (β2-AR) gene have been identified, including the amino acid substitution from arginine (Arg) to glycine (Gly) at codon 16 and from glutamine (Gln) to glutamic acid (Glu) at codon 27. These substitutions affect receptor function and show significantly more agonist-promoted receptor down-regulation than cells expressing the Arg 16/Gln 27 variants. Although the ethnic dependency of this polymorphism has been described in other populations, no studies investigating its relationship to asthma have been conducted in the Saudi population . Therefore, our main objective was to determine the prevalence of these two mutations among patients with asthma in the Eastern Province and in matched healthy controls.
DESIGN AND SETTING:
A case-control study conducted at a university hospital among Saudi patients
PATIENTS AND METHODS:
Blood samples were collected from 73 asthmatic patients and from 85 controls, and the β2-AR gene polymorphisms at codon 16 and codon 27 were assessed by restriction fragment length polymorphism.
RESULTS:
Although a significant difference was observed in genotype frequencies at codon 16 (Arg/Gly) between the asthmatic and normal control subjects (P<.05), no statistically significant difference was observed in allele frequencies between the two groups. In addition, no statistically significant differences were observed in genotype and allele frequencies at codon 27 (Gln/Glu) between the normal (control) and asthmatic groups (β2=0.75, P>.68). Using the THESIAS statistical program, no significant association of any haplotype with asthma was found.
CONCLUSIONS:
Our findings indicate a poor association of individual single-nucleotide polymorphisms with asthma. However, further study is required to ascertain the interactions of different haplotypes and the response of patients with different haplotypes to various treatments.
Asthma is a chronic disease that affects over 100 million people worldwide.1,2 Understanding the genetic basis of asthma may contribute toward identifying better targets for innovative asthma drugs.3,4 Reports have been available suggesting that a defective β2-adrenergic receptor (β2-AR) plays a significant role in bronchial asthma.5 Moreover, ethnic differences in β2-AR density have been reported in one study.6 A number of single-nucleotide polymorphisms (SNPs) in the β2-AR gene have been detected in many populations.7–9 Although these polymorphisms are not deemed to be susceptibility genes for asthma, they have been reported to be associated with functional changes in the β2-AR in the respiratory system.10 The most common SNPs are due to two missense mutations, which occur in the coding region of the intronless β2-AR gene. The first SNP is at nucleotide 46, which causes the substitution of glycine (Gly) for arginine (Arg) at codon 16. The second SNP is at nucleotide 79, which results in the substitution of glutamic acid (Glu) for glutamine (Gln) at codon 27. In vitro studies of these two nonsynonymous SNPs have shown that they alter receptor function. Many studies on the association between asthma severity and the β2-AR polymorphisms have produced conflicting results.11–13 The Arg/Arg polymorphism at position 16 of the β2-AR has been reported to be associated with enhanced agonist-mediated desensitization, whereas a meta-analysis that included several thousand individuals suggested an important role for the Glu/Gln polymorphism in protection against asthma.14 Another meta-analysis study that was also composed of several thousand individuals suggested that Arg/Arg polymorphism could possibly contribute to nocturnal symptoms;15 whereas another study concluded that there was no significant association between polymorphisms and asthma or asthma severity.16
Asthma is prevalent in Saudi Arabia, with the Eastern Province being reported as having one of the highest incidences.17 A study confirmed that asthma, coronary obstructive pulmonary disorder and pneumonia are the leading causes of hospitalization of patients with respiratory disorders.18 Although the allele frequencies of these two polymorphic sites have been reported for the normal Saudi population,19 there is no report of whether β2-AR polymorphisms are associated with asthma in this population. This prompted us to carry out the present study to determine the prevalence of these polymorphic sites in normal Saudi individuals and in asthmatic patients.
PATIENTS AND METHODS
A case-control study was conducted among 73 patients clinically diagnosed with asthma who were visiting King Fahad Hospital of the University, Al-Khobar, Saudi Arabia. All those who participated in the study were of Saudi origin residing in the Eastern Province. Normal (control) subjects (n=85) matched with case patients for age and gender were recruited from the general population. The sole exclusion criterion for control subjects was a past, present, or family history of asthma. Informed written consent was obtained from both the patient and control groups prior to participation in the study, which was approved by the University of Dammam Medical Ethics Committee. Blood samples were collected in EDTA tubes and were frozen until analysis. Genomic DNA was obtained from 300 μL whole blood using QIAamp Blood Kit (Qiagen, Hilden, Germany) according to the manufacturer's protocol. Genotypes were determined by restriction fragment length polymorphism, as previously described.15 Briefly, a 308-bp region of the β2-AR spanning both polymorphic sites was amplified. Primers 5’ CCT TCT TGC TGG CAC CCC AT-3’ (sense) and 5’ GGA AGT CCA AAA CTC GCA CCA-3’ (antisense) were used. The PCR reaction volume of 25μL contained 100-250ng of DNA, 1.5mM MgCl 2, 200μM dNTP and 0.25 U Tag polymerase in a standard PCR buffer. PCR cycles involved initial 5 minutes at 94°C followed by 30 cycles at 94°C for 30 seconds, 58°C for 30 seconds, and a final extension at 72°C for 10 minutes. The PCR product was then digested with restriction enzyme NcoI for Arg 16-Gly and BbvI for the Glu 27-Gln polymorphism at 45°C for 1 hour. Restriction products were separated on 3% agarose and visualized under UV illumination following ethidium bromide staining.
Genotype and allele frequencies were estimated by gene counting and expressed as percentages of the total. The β2 test was used to compare differences between groups. A difference was considered statistically significant when P was <.05. The association of haplotypes with asthma was analyzed using THESIAS statistical software (http://genecanvas.ecgene.net/).
RESULTS
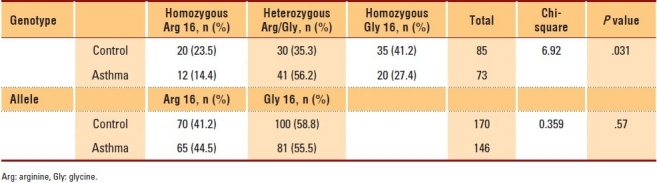
A total of 158 subjects (73 patients and 85 controls) were analyzed. The baseline characteristics of the two study groups are shown in Table 1. The two groups were similar in age and gender. The genotype distribution of all SNPs for both groups was consistent with the Hardy-Weinberg equilibrium. The genotype and allele frequencies of β2-AR polymorphism at codon 16 (Arg 16-Gly) in normal (control) and asthmatic subjects are presented in Table 2. Although a significant difference was observed in genotype frequencies between the asthmatic and normal control subjects (P<.05), no statistically significant difference was observed in allele frequencies between the two groups. However, the data showed that asthmatic patients were twice as likely to carry the Arg 16-Gly genotype when compared to homozygous Gly 16 (odds ratio=2.39; 95% Cl, 1.16-4.931)
Table 1.
Baseline characteristics of asthmatic patients and control subjects
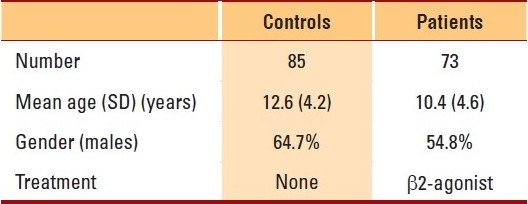
Table 2.
Distribution of genotype and allele frequencies of β-adrenergic receptor at codon 16 (Arg/Gly) in the control and asthmatic subjects
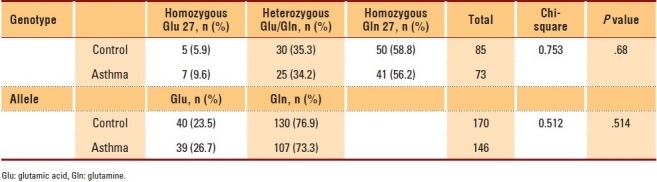
The genotype and allele frequencies of β2-AR polymorphism at codon 27 (Glu 27-Gln) in control and asthmatic subjects are summarized in Table 3. No statistically significant differences were observed in genotype and allele frequencies between the control and asthmatic groups (β2=0.75, P>.68).
Table 3.
Distribution of genotype and allele frequencies of β-adrenergic receptor at codon 27 (Glu/Gln) in control and asthmatic subjects
The results also indicate that linkage disequilibrium existed between the β2-AR codon 16 and β2-AR codon 27 polymorphisms (|D’|=0.57). The estimated frequencies for various haplotypes in both the control and patient groups and the significance of association with asthma are presented in Table 4. The data for all haplotypes failed to show a significant association.
Table 4.
Comparison of haplotypes frequencies between patients and controls

DISCUSSION
Studies have shown that genetic polymorphisms may play an important role in the susceptibility to, or severity of, diseases. With the conclusion of the human genome project, a tremendous amount of clinical and basic research has been carried out that focused on this relationship. Asthma is a chronic disease with both environmental and genetic factors. The The results also indicate that β2-AR receptor gene polymorphism has been implicated in the severity of asthma or drug responsiveness of asthmatic patients.16,20 A single amino acid substitution in the structural domains critical for receptor function has been shown to result in significant changes in the receptor activity.7
Nine polymorphisms in the The results also indicate that β2-AR gene have been identified, two of which (Arg 16-Gly and Glu 27-Gln) were more frequently found in different populations with different frequencies. Many studies have been carried out to investigate the possible relationship between these two polymorphisms and susceptibility to asthma. Although some studies have shown that there is a weak association between Arg 16-Gly polymorphism and asthma, other studies did not show such an association.14 Moreover, previous studies have also shown contradictory results concerning Glu 27-Gln polymorphism and its association with the development of asthma.
The genotype frequencies for both polymorphic sites determined in this study in normal subjects were slightly different from those previously reported.19 This is probably due to differences in Saudi populations residing in different areas of the Kingdom. Although a significant difference was observed in genotype frequencies at codon 16 (Arg 16-Gly) between the asthmatic and control subjects (P<.05), no statistically significant difference was observed in allele frequencies between the two groups (P>.05). Our results of allelic frequencies of Arg 16-Gly polymorphism are in line with those of Reihsaus et al. (1993), who examined the frequency of this polymorphic site of the β2-AR gene in different population groups.9 Reihsaus et al (1993) found no significant difference in the frequency of the Arg 16-Gly polymorphism between a group of 51 moderate-to-severe asthmatics and 56 normal (control) subjects. While comparing the genotype and allele frequencies of Glu 27-Gln, no significant differences were observed between the asthmatic group and the control group (P>.05). Our data appears to agree with the accepted hypothesis, which states that the Arg 16-Gly polymorphism does not appear to be associated with the development of asthma per se, but it may play a secondary role in the pathogenesis of certain forms of asthma.9
Previous reports have indicated an ethnic difference in the frequency of different haplotypes. It has also been reported that the unique interactions of multiple SNPs within a haplotype affect phenotype more prominently than individual SNPs.20 We examined the association of both SNPs and haplotypes with asthma and concluded that there was no significant association.
To summarize, we have presented the genotype and allele frequencies of β2-AR gene polymorphisms in normal Saudi subjects and in asthmatic patients. Our findings indicate that there was no significant association of individual SNPs with asthma. However, further study is required to ascertain the interactions of different haplotypes and the response of patients with different haplotypes to various treatments.
Acknowledgments
The author would like to extend his thanks and gratitude to the University of Dammam for the financial support for this project.
REFERENCES
- 1.Fuhlbrigge AL, Adams RJ, Guilbert TW, Grant E, Lozano P, Janson SL, et al. The burden of asthma in the United States level and distribution are dependent on interpretation of the national asthma education and prevention program guidelines. Am J Respir Crit Care Med. 2002;166:1044–9. doi: 10.1164/rccm.2107057. [DOI] [PubMed] [Google Scholar]
- 2.Deen JL, Vos T, Huttly SR, Tulloch J. Injuries and non-communicable diseases: Emerging health problems of children in developing countries. Bull World Health Organ. 1999;77:518–24. [PMC free article] [PubMed] [Google Scholar]
- 3.Hall IP. The future of asthma. Br Med J. 1997;314:45–9. doi: 10.1136/bmj.314.7073.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hogg JC. The pathology of asthma. APMIS. 1997;105:735–45. doi: 10.1111/j.1699-0463.1997.tb05079.x. [DOI] [PubMed] [Google Scholar]
- 5.Bai TR. Beta2-adrenergic receptors in asthma: A current perspective. Lung. 1992;170:125–41. doi: 10.1007/BF00174316. [DOI] [PubMed] [Google Scholar]
- 6.Suarez EC, Saab PG, Llabre MM, Kuhn CM, Zimmerman E. Ethnicity, gender and age affects an adrenoceptors and physiological responses to emotional stress. Psychophysiology. 2004;41:450–60. doi: 10.1111/j.1469-8986.00161.x. [DOI] [PubMed] [Google Scholar]
- 7.Green SA, Cole G, Jacinto M, Innis M, Liggett SB. A polymorphism of the human beta 2-adrenegic receptor within the fourth transmembrane domain alters ligand binding and functional properties of the receptor. J Biol Chem. 1993;268:23116–21. [PubMed] [Google Scholar]
- 8.Green SA, Turki J, Innis M, Liggett SB. Amino-terminal polymorphisms of the human beta 2-adrenergic receptor impart distinct agonist-promoted regulatory properties. Biochemistry. 1994;33:9414–9. doi: 10.1021/bi00198a006. [DOI] [PubMed] [Google Scholar]
- 9.Reihsaus E, Innis M, MacIntyre N, Liggett SB. Mutations in the gene encoding for the beta 2-adrenergic receptor in normal and asthmatic subjects. Am J Respir Cell Mol Biol. 1993;8:334–9. doi: 10.1165/ajrcmb/8.3.334. [DOI] [PubMed] [Google Scholar]
- 10.Green SA, Turki J, Bejarna P, Hall IP, Ligget SB. Influence of b2-adrenergic receptor genotypes on signal transduction in human airway smooth muscle cells. Am J Respir Cell Mol Biol. 1995;13:25–33. doi: 10.1165/ajrcmb.13.1.7598936. [DOI] [PubMed] [Google Scholar]
- 11.Dewar JC, Wilkinson J, Wheatley A, Thomas NS, Doull I, Morton N, et al. The glutamine 27 b2 adrenoceptor polymorphism is associated with elevated IgE levels in Asthmatic families. J Allergy Clin Immunol. 1997;100:261–5. doi: 10.1016/s0091-6749(97)70234-3. [DOI] [PubMed] [Google Scholar]
- 12.Dewar JC, Wheatley T, Venn A, Morrison JFJ, Britton J, Hall IP. β2 adrenoceptor polymorphism are in linkage disequilibrium, but are not associated with asthma in adult population. Clin Exp Allergy. 1998;28:442–8. doi: 10.1046/j.1365-2222.1998.00245.x. [DOI] [PubMed] [Google Scholar]
- 13.Weir TD, Mallek N, Sandford AJ, Bai TR, Awadh N, Fitzgerald JM, et al. Beta 2 adrenergic receptor haplotypes in mild, moderate and fatal/near fatal asthma. Am J Respir Crit Care Med. 1998;158:787–91. doi: 10.1164/ajrccm.158.3.9801035. [DOI] [PubMed] [Google Scholar]
- 14.Thakkinstian A, McEvoy M, Minelli C, Gibson P, Hancox B, Duffy D, et al. Systematic review and meta-analysis of the association between β2-adrenoceptor polymorphisms and asthma: A HuGE review. Am J Epidemiol. 2005;62:201–11. doi: 10.1093/aje/kwi184. [DOI] [PubMed] [Google Scholar]
- 15.Contopoulos-loannidis DG, Manoli EN, Ioannidis JP. Meta-analysis of the association of beta-adrenergic receptor polymorphisms with asthma phenotypes. J Allergy Clin Immunol. 2005;115:963–72. doi: 10.1016/j.jaci.2004.12.1119. [DOI] [PubMed] [Google Scholar]
- 16.Holloway JW, Dunbar PR, Riley GA, Sawyer GM, Fitzharris PF, Pearce N, et al. Association of b-2 adrenergic receptor polymorphisms with severe asthma. Clin Exp Allergy. 2002;30:1097–103. doi: 10.1046/j.1365-2222.2000.00929.x. [DOI] [PubMed] [Google Scholar]
- 17.Al-Frayh A, Benar AB, Al-Jawadi TQ. Prevalence of asthma among Saudi children. Saudi Med J. 1992;13:521–4. [Google Scholar]
- 18.Alamoudi OS. Prevalence of respiratory diseases in hospitalized patients in Saudi Arabia: A 5 years study 1996-2000. Ann Thorac Med. 2008;1:76–80. [Google Scholar]
- 19.Maxwell TJ, Ameyaw MM, Pritchard S. Beta2-adrenergic receptor genotypes and haplotypes in different ethnic groups. Int J Mol Med. 2005;16:573–80. [PubMed] [Google Scholar]
- 20.Carroll CL, Stoltz P, Schramm CM, Zucker AR. β2-adrenergic receptor polymorphisms affect response to treatment in children with severe asthma exacerbations. Chest. 2009;135:1186–92. doi: 10.1378/chest.08-2041. [DOI] [PubMed] [Google Scholar]