

Abstract
Dyskeratosis congenita (DC) is a rare disease characterized by hyperpigmentation, nail dystrophy and mucous membrane abnormality. Commonly occurring in males, the patients die young usually due to bone marrow suppression. Malignancies of various descriptions have been reported in this disease, the commonest being solid tumors of head/neck (squamous cell carcinoma). We report the case of a female patient with DC, who presented to us with severe wasting and primary amenorrhea and died of carcinoma stomach in our hospital 3 weeks later.
Keywords: Adenocarcinoma of stomach, dyskeratosis congenita, primary amenorrhea
Introduction
Dyskeratosis congenita (DC) is a rare inherited disorder characterized by premature aging, bone marrow failure and predisposition to malignancies.
In its classical form, there is skin pigmentation, nail dystrophy and mucous membrane leukoplakia. The major form of DC is X-linked and, therefore, there is an abundance of male patients. However, carrier females may have complete clinical manifestation.[1] We report the case of a female patient, who presented to us with hyperpigmentation, significant weight loss and primary amenorrhea. She expired within 3 weeks of hospital admission.
Case Report
Our patient was a 21-year-old woman with progressive weight loss, loss of appetite and extreme weakness for the last 6 months. She also had history of gradually increasing pigmentation in various parts of the body along with marked hair loss for the last 8 years. The patient had not experienced menarche till then. There was no history of fever, diarrhea, sexual exposure, polyuria/polyphagia or palpitations.
On examination, the patient was 140 cm tall, with a weight of 20 kg [body mass index (BMI) 10.8 kg/m2] and had an emaciated build. She had moderate pallor with normal pulse rate and rhythm. Her BP was 100/60 mm of Hg without any significant postural drop. Secondary sexual characters were infantile. There was no edema, clubbing, icterus, lymphadenopathy or sternal tenderness. Thyroid gland was normal. Skin examination revealed reticulate hyperpigmentation, telangiectasia and some depigmented macules on neck, chest as well as all the flexural surfaces [Figure 1]. Examination of the oral cavity revealed swollen gums, white patches over the tongue [Figure 2], hard palate [Figure 3] and buccal mucosa. The patient had diffuse alopecia over the scalp. The nails were brittle with vertical ridges [Figure 4]. There was no abdominal organomegaly or free fluid. Respiratory, central nervous system and cardiovascular system examination was noncontributory.
Figure 1.

Reticulate hyperpigmentation, telangiectasia and depigmented macule on neck and periorbital areas
Figure 2.

Leukoplakia of tongue and dental malalignment
Figure 3.
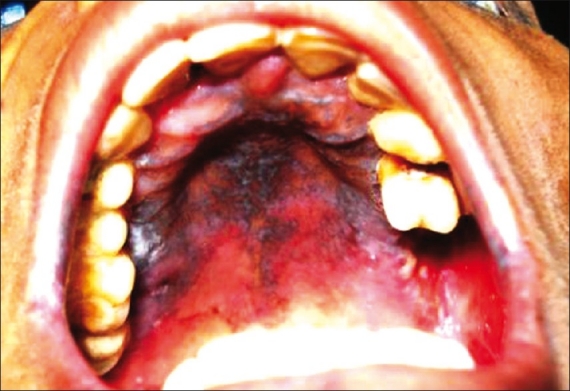
Network of leukoplakia on hard palate
Figure 4.

Finger nails showing vertical ridges and broken edges
Blood examination showed 7.5 g/dl of hemoglobin, WBC count of 3500/mm3 and platelet count of 100,000/mm3. Blood biochemistry was essentially normal, including electrolytes and albumin. Chest X-ray was noncontributory. USG abdomen revealed hypoplastic uterus with infantile ovaries. Anti nuclear antibody was negative and test for HIV was nonreactive. In view of the weight loss, hypotension and pigmentation, a cosyntropin test was done and 1 hour serum cortisol was normal. Thyroid profile was noncontributory. Other hormones like luteinizing hormone (LH), follicle stimulating hormone (FSH) as well as estrogen and progestogen gave low values depicting a hypogonadotropic hypogonadism. A skin biopsy was taken for characterization of the pigmentation.
Meanwhile, the patient started going downhill with onset of melena, poor intake and increasing pallor. Blood transfusions were given and upper GI endoscopy was done. The endoscopy revealed a proliferative growth at the antral region of stomach. Biopsy proclaimed an adenocarcinoma of stomach. The skin biopsy was consistent with DC. Unfortunately, we lost the patient before further evaluation was possible.
Discussion
The differential diagnosis, when the patient was first encountered, included Addison's disease, polyglandular autoimmune syndromes, internal malignancy, malabsorption syndrome with pellagra and even anorexia nervosa. However, as the preliminary reports arrived, most of these were excluded.
Characteristic reticulate pigmentation interspersed with areas of depigmentation in the flexural zones was suggestive of disorders of reticulate pigmentation like Dowling Degos disease, reticulate acropigmentation of Kitamura, Revescz Syndrome and DC.
Apart from pigmentation, this patient had alopecia, nail dystrophy and leukoplakia of the tongue. She had moderate anemia and mild leukopenia and suffered an untimely death due to carcinoma stomach at the age of 22 years. The conglomeration of features pointed toward DC.
DC is a rare disease with around 500 cases reported from 1910 to 2008.[2] The number of male cases is three times that of female ones. This is because of an X-linked transmission in most cases. In 1995, a DC Registry was established, which showed 76 out of 83 patients as males. Heterozygous females show variable expression depending on tissue-specific patterns of random X-inactivation. However, autosomal dominant and autosomal recessive inheritances have been reported. The gene responsible for X-linked DC encodes for a protein “dyskerin” that is essential for ribosomal biosynthesis and telomerase RNP assembly. Autosomal dominant form has mutations in the RNA component of the telomerase human telomerase RNA component (hTERC). Defects in these mechanisms lead to diminished telomere lengths.[3]
The clinical manifestations start appearing at the second decade of life. Apart from skin and appendicular abnormalities, the patient eventually develops bone marrow depression, which is the commonest cause of mortality. Some atypical features include pulmonary fibrosis and renal agenesis.[4,5] These patients are also predisposed to various types of malignancies like squamous cell carcinomas of skin and mucous membranes, adenocarcinomas of anorectum, esophagus, stomach, CA pancreas, Hodgkin's disease and many more. The exact incidence of CA stomach in DC is not known. Available literature is in the form of anecdotal case reports, one from India as well.[6,7]
This patient had another interesting aspect, i.e., primary amenorrhea. Hormonal assay revealed hypogonadotrophic hypogonadism. This patient may not have attained the critical body weight required for menarche. She had always been frail in comparison to her siblings.
Hypogonadism and hyposthenic build have been documented in DC but no specific data are available regarding primary amenorrhea for females.[8,9]
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Knight S, Vulliamy T, Copplestone A, Gluckman E, Mason P, Dokal I. Dyskeratosis Congenita (DC) Registry: Identification of new features of DC. Br J Haematol. 1998;103:990–6. doi: 10.1046/j.1365-2141.1998.01103.x. [DOI] [PubMed] [Google Scholar]
- 2.Alter BP, Giri N, Savage SA, Rosenburg PS. Cancer in dyskeratosis congenita. Blood. 2009;113:6502–3. doi: 10.1182/blood-2008-12-192880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bessler M, Wilson DB, Mason PJ. Dyskeratosis congenita and telomerase. Curr Opin Pediatr. 2004;16:23–8. doi: 10.1097/00008480-200402000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Balci S, Engiz O, Erekul A, Gozdasoglu S, Vulliamy T. An atypical form of dyskeratosis congenita with renal agenesis and no mutation in DKC1, TERC and TERT genes. J Eur Acad Dermatol Venereol. 2009;23:607–8. doi: 10.1111/j.1468-3083.2008.02985.x. [DOI] [PubMed] [Google Scholar]
- 5.Hermann M. Idiopathic pulmonary fibrosis - telomerase mutation in familial form. Pneumologie. 2008;62:121. doi: 10.1055/s-2008-1075045. [DOI] [PubMed] [Google Scholar]
- 6.Chatura KR, Nadar S, Pulimood S, Mathai D, Mathan MM. Gastric carcinoma as a complication of dyskeratosis congenita in an adolescent boy. Digest Dis Sci. 1996;41:2340–2. doi: 10.1007/BF02100124. [DOI] [PubMed] [Google Scholar]
- 7.Baykal C, Kavak A, Gukan P, Buyukbabani N. Dyskeratosis congenita associated with three malignancies. J Eur Acad Dermatol Venereol. 2003;17:216–8. doi: 10.1046/j.1468-3083.2003.00585.x. [DOI] [PubMed] [Google Scholar]
- 8.Sorrow JM, Jr, Hitch JM. Dyskeratosis congenita.First report of its occurrence in a female and a review of literature. Arch Dermatol. 1963;88:340–7. doi: 10.1001/archderm.1963.01590210098015. [DOI] [PubMed] [Google Scholar]
- 9.Kalb ER, Grossman ME, Hutt C. Avascular necrosis of bone in dyskeratosis congenita. Am J Med. 1986;80:511–3. doi: 10.1016/0002-9343(86)90730-8. [DOI] [PubMed] [Google Scholar]