

Abstract
The famous castrato singer Farinelli (1705–1782) was exhumed by our research group in July 2006 for the purpose of gaining some insight into his biological profile through a study of his skeletal remains. Farinelli was castrated before puberty to preserve the treble pitch of the boy's voice into adult life. His powerful and sweet voice became legendary. In spite of its bad preservation state, the skeleton displayed some interesting characteristics that are probably related to the effects of castration, including long limb-bones, persistence of epiphyseal lines and osteoporosis. In particular, the frontal bone was affected by severe hyperostosis frontalis interna (HFI). This condition consists in a symmetrical thickening of the inner table of the bone. The epidemiology of HFI shows that it is relatively common in postmenopausal women but very rare in men. Men affected by this pathology suffer from diseases, syndromes or treatments causing androgen deficiency. In the case of Farinelli, castration was probably responsible for the onset and development of this lesion.
Keywords: castration, Farinelli, hyperostosis frontalis interna, osteoporosis
Introduction
The remains of the famous castrato Carlo Broschi, better known as Farinelli (Andria, 1705– Bologna, 1782), were exhumed in July 2006 for research purposes. The event was promoted by a group of music enthusiasts at the Centro Studi Farinelli, and by scientists of the Universities of Bologna and Pisa. The former hoped that Farinelli's skeletal remains would disclose the secret of his legendarily sweet, powerful, voice. The latter were especially interested in reconstructing the biological profile of this male singer who underwent castration before puberty. In fact this operation, depriving the individual of his testes and hence of their testosterone secretions, must have had consequences for the development of the male secondary sexual characteristics such as laryngeal development and skeletal growth, and may have caused some hormone-related pathologies. The poor preservation state of the remains made any insight into the secret of the legendary voice impossible to obtain, but revealed interesting information on the second aspect. The aim of this paper is to describe the most striking of the osteological features of Farinelli that are likely to be attributable to castration.
Life history of Farinelli
Carlo Broschi, destined by his family to have a singing career, was castrated before puberty to preserve his exceptional boy's treble voice into adult life. The castrato voice was appreciated throughout Western Europe from the 16th century, and especially in the 18th century, with the increasing popularity of opera. Pre-pubertal castration was practised especially in Italy (Jenkins, 1998). Farinelli was considered by his contemporaries to be the most outstanding singer of his time. His voice could span over three octaves and his thoracic development allowed him to hold a note for a whole minute without taking breath (Jenkins, 1998). He performed with great success in theatres throughout Western Europe. At the height of his career, at the age of 32, he was invited to the Spanish court, where he spent the following 23 years, also holding institutional responsibilities. He then retired to Bologna, where he lived until his death. In 1784 Sacchi wrote: ‘Farinelli died of a fever on September the 16th 1782, close to 78 years of age. He preserved a good memory and was lucid until the day before his death. He accepted the disease as an act of God's will in keeping with his Christian faith’. He was buried in the Church of the Capuchins monastery in Bologna, which was destroyed in 1810 as a result of the Napoleonic invasion of 1796. His corpse was then moved to Certosa, the main cemetery of Bologna, at the bequest of his great-niece Maria Carlotta Pisani. In 1842, Farinelli's remains were moved again in the same tomb that would receive the corpse of Maria Carlotta after her death in 1850. In 2006, Farinelli was exhumed again by our research group.
Recovery and preservation of the remains
When the underground brick tomb at the Certosa cemetery was opened, we found the remains of Farinelli accumulated at the feet of his great-niece (Fig. 1). Farinelli's remains were without any protective structure. Their preservation was poor due to the microclimatic conditions of the tomb and water infiltration, as shown by the concretions found near and on the bones. The bones were very fragile and fragmentary; of the skull, only facial fragments and the incomplete frontal bone were preserved (Fig. 2).
Fig. 1.

Farinelli's tomb. Tomb containing the remains of Farinelli and Maria Carlotta Pisani. Farinelli's bones are accumulated at the feet of his great-niece (circle).
Fig. 2.
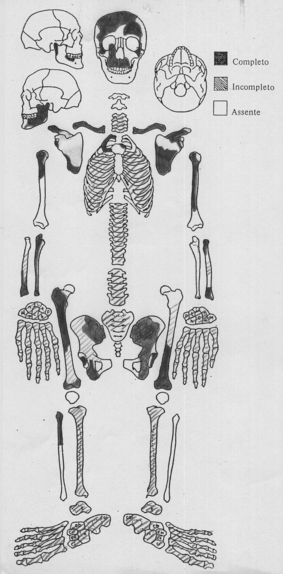
Preservation state. Scheme of the preserved bones of Farinelli.
Osteobiography of Farinelli
In spite of the poor preservation state of Farinelli's skeleton, we observed some characteristics that allow reconstruction of his biological profile. Some of them, such as tall stature and the presence of pathological conditions more frequently found in females, are likely related to castration.
In August 1770, Charles Burney described the 65-year-old Farinelli as follows: ‘Mister Farinelli still lives and is in good health and spirits. I found him much younger in appearance than I expected. He is extremely tall and thin and has a youthful air and he seems by no means infirm’ (Burney, 1773). Many portraits and caricatures of the famous singer confirm this description (Fig. 3), as do his skeletal features.
Fig. 3.

Farinelli's portrait by Corrado Giaquinto (ca. 1750).
The only clear skeletal indicators of sex (cf. Ferembach et al. 1980; Buikstra & Ubelaker, 1994) were the narrow ischiatic notch and the absence of the preauricular sulcus in the left hip bone, typical of males (Fig. 4).
Fig. 4.
Left hip bone. Note the narrow greater sciatic notch and the persistence of the epiphyseal line of the iliac crest.
A few skeletal age markers were preserved. The only preserved portion of the cranial sutures (the lateral, part of the right coronal suture) was completely fused. The irregularity and porosity of the auricular surface is also consistent with old age. The extreme fragility and lightness of the bones, the trabecular thinning and the wide marrow spaces found in cancellous bone, together with a compression fracture of a lumbar vertebra (4th or 5th?) (Fig. 5), indicated an osteoporotic condition. Indicators of degenerative joint disease (marginal lipping, surface porosity) were observed in the few articulations preserved, especially in the vertebral column. All these features are consistent with the relatively advanced age at death. However, the epiphyseal line was still visible on the medial border of the left scapula and on the left iliac crest (Fig. 4). Both sites are normally completely fused at 23 years (McKern & Stewart, 1957). A study of adult age markers in two 19–20th century skeletal collections (Coimbra, Portugal, and Sardinia, Italy) showed that the persistence of the epiphyseal line in completely fused epiphyses is unusual in adults >35 years old (Rastelli, 2005). The iliac crest was completely fused without traces of the epiphyseal line in 91–100% of males over 35 years (the percentage varied in relation to the sex and collection; the medial scapular border was not considered in that study). Considering only males over 50 years, traces of the epiphyseal line were visible in only 1.8% (2/113) in the Sardinian sample and 1.3% (1/79) in the Coimbra sample (Rastelli, 2005).
Fig. 5.

Crush fracture of the lumbar vertebra (superior and lateral view).
The estimation of living height based on the right ulna (Olivier et al. 1978), the only bone whose complete length could be measured (maximum length: 315 mm), gave a value of 190 cm (6 ft 3 in).The dentition was in good condition. Twenty-five teeth were preserved and only two were decayed (caries was recordable in only 14 teeth). This situation is compatible with good oral care. The health and aesthetic of the dentition is likely to have been important in the career of a singer.
The biological profile of Farinelli's remains is consistent with the historical data in our possession, strongly supporting the identification of the skeletal remains as those of Farinelli.
This osteobiography confirms the presence of many characteristics that one would expect to see in a castrato, e.g. long limb-bone dimensions and consequential tall stature due to delayed epiphyseal fusion (cf. Jenkins, 1998). The crush fracture of the lumbar vertebra is typical of postmenopausal osteoporosis in women, whereas in age-related osteoporosis, which affects both sexes over 70 years (though more common in women), the vertebral fractures are often of the multiple wedge type (Riggs, 1991). It has been reported that hypogonadism in either sex increases the incidence of osteoporosis (Riggs, 1991). Another interesting feature likely to be related to castration is the severe hyperostosis frontalis interna (HFI) affecting the frontal bone. This pathology will be analysed in detail below.
Paleopathological analysis of Farinelli's skull
The endocranial surface of the frontal bone is characterised by a continuous bilateral and rather symmetrical bony thickening caused by the deposition of appositional bone, not affecting the groove for the superior sagittal sinus. The bony thickening has an irregular and lobular appearance with clearly demarcated borders near the sagittal sulcus (Figs 6 and 7). Where post mortem breakage reveals a profile of the thickened area, the diploe thickness shows no clear discontinuity (Fig. 8). The frontal bone thickness ranges from 9 mm at the sagittal sulcus (free of appositional bone), to 21 mm at the maximally thickened area. All these features indicate the most severe grade of hyperostosis frontalis interna (type D according to Hershkovitz et al. 1999: continuous bony overgrowth, involving more than 50% of the frontal endocranial surface); they also allow a clear differentiation from other diseases that may produce endocranial bone thickening, such as Paget's disease, acromegaly, fibrous dysplasia and meningioma (Hershkovitz et al. 1999).
Fig. 6.
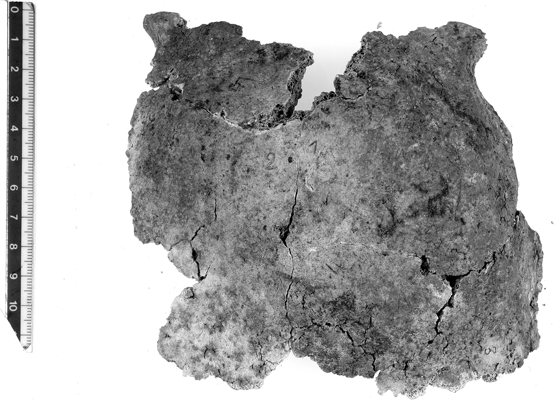
Ectocranial view of the frontal bone reconstructed from five fragments.
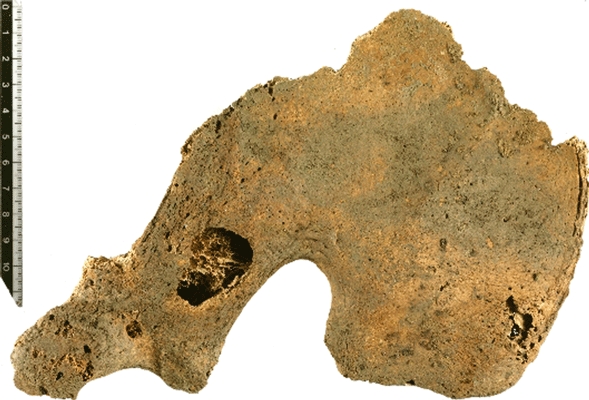
Fig. 7.

Endocranial view of the frontal bone showing severe hyperostosis frontalis interna. Note the irregular and lobular appearance of the appositional bony thickening, sparing the groove for the superior sagittal sinus.
Fig. 8.

Hyperostosis frontalis interna: endocranial view of a frontal bone fragment before restoration. Note the clearly demarcated borders of the appositional bone adjacent to the sagittal sulcus and the continuity of the thickened diploe (left side of the pictures).
The prevalence of HFI in modern populations is still disputed, but it is much more common in women (24%) than in men (5%) (Hershkovitz et al. 1999; May et al. 2010a). Most of the clinical cases of HFI have been observed in postmenopausal women (Salmi et al. 1962; Barber et al. 1997; Devriendt et al. 2005; May et al. 2010a). Few cases of HFI have been described in males.
Despite the vast literature on HFI, ambiguity exists as to its aetiology (Hershkovitz et al. 1999; Yamakawa et al. 2006; Talarico et al. 2008; Nikolić et al. 2010). HFI can result from hormonal disturbances (prolonged oestrogen stimulus during the reproductive period, menstrual disorders, hyperprolactinemia, galactorrhea, etc.), anomalous glucose regulation (diabetes mellitus), arterial hypertension, obesity and genetic factors. Even though no clinical symptoms or disorders appear to be specific to HFI, the association with Morgagni–Stewart–Morel (headache, obesity, virilism and hypertrichosis, behaviour disturbances) and Troell–Junet syndromes (acromegaly, toxic goiter and diabetes mellitus), as well as with epilepsy and dementia, have been reported (Ortner & Putschar, 1985; Armelagos & Chrisman, 1988; Barber et al. 1997; Hershkovitz et al. 1999; Rühli et al. 2004; Devriendt et al. 2005; Yamakawa et al. 2006; Nikolić et al. 2010). Both the occurrence and the severity of HFI in women are progressive age-related phenomena. The mildest form of HFI has been observed in females around 20 years of age and advanced forms do not appear before the age of 40 (Hershkovitz et al. 1999; Nikolić et al. 2010). Most patients are asymptomatic (Barber et al. 1997). The slow progression of HFI and accompanying cortical compression may allow individual patients to develop compensatory processes that preclude the appearance of any sudden pronounced impairment (Hershkovitz et al. 1999; Nikolić et al. 2010).
As far as we know, all male cases of HFI are associated with sex hormonal disturbance. Men with HFI and feminisation and/or testicular atrophy have been described in reports from the mid-20th century (Hershkovitz et al. 1999). Hershkovitz et al. (1999) describe the case of a male cadaver with HFI and a single atrophied testis. A clinical case refers to a 72-year-old male affected by hypogonadism (Yamakawa et al. 2006). Two cases of HFI associated with Klinefelter's syndrome, which causes reduced testosterone and increased circulating oestradiol, have been reported (Néel et al. 1974; Ramchandren & Liebeskind, 2007). HFI has also been found associated with Kallmann syndrome (hypogonadism caused by a deficiency of gonadotropin-releasing hormone, GnRH) (Miazgowski et al. 1991). A 32-year-old man with the Morgagni–Morell–Stewart syndrome showed increased serum concentrations of prolactin and thyrotropic hormone (Hrycek et al. 1989). Recently, May et al. (2010b) reported that males who are hormonally treated for prostatic cancer (androgen suppression altering the androgen–oestrogen ratio) are at a higher risk of developing HFI compared to healthy males.
These case reports allow us to relate the finding of HFI in Farinelli's skull with castration.
Concluding remarks
As far as we are aware, there are no published reports on the skeletal characteristics of castrati and eunuchs. The osteobiography of the castrato singer Farinelli presented in this study confirms the presence of many characteristics likely to be related to castration. Regarding HFI in cases of induced hypogonadism, the intellect is not impaired, but there may be a sense of inferiority (though this is unlikely in the case of exceptionally successful singers such as Farinelli) (Jenkins, 1998). Farinelli was described as a good-natured man with an inclination to melancholy that worsened with advancing age. He found release in music and singing, having preserved a beautiful and powerful voice until the end. Three weeks before his death he sang almost the whole day long. He also preserved a good memory and was lucid until the day before his death (Verdi, 2005). These elements indicate that he did not suffer from any of the behavioural disturbances and psychiatric disorders that have been associated with HFI (Devriendt et al. 2005).
In his testament, Farinelli expresses his wishes for his funeral:
‘My poor body, once it has become a cadaver, I ask that it be wrapped up in my cloak of the Calatrava Order, […] and that it be buried without any pomp and circumstance, accompanied by fifty poor people […] all of whom will receive a donation […] I also ask that four hundred masses are given in my memory […]’ (Broschi, 1782).
Acknowledgments
We would like to thank Maestro Luigi Verdi and Carlo Vitali of the Centro Studi Farinelli for providing bibliography and information on Farinelli's life and figure, Dr Benedetta Bonfiglioli for studying the teeth of Farinelli, Dr Stefano Durante of the Istituti Ortopedici Rizzoli (Bologna, Italy) for the CT analysis, and Angelo Rosa for taking the pictures.
Author contributions
Belcastro Maria Giovanna and Mariotti Valentina: research design, acquisition and interpretation of data, drafting of the manuscript; Todero Antonio and Fornaciari Gino: critical revision of the manuscript.
For permission to use the Farinelli portrait we thank Dott.ssa Jenny Servino, Head of the Museo internazionale della Musica di Bologna, and Dr. Mauro Felicori, Head of the Area della Cultura del Comune di Bologna.
References
- Armelagos GJ, Chrisman OD. Hyperostosis frontalis interna: a Nubian case. Am J Phys Anthropol. 1988;76:25–28. doi: 10.1002/ajpa.1330760103. [DOI] [PubMed] [Google Scholar]
- Barber G, Watt I, Rogers J. A comparison of radiological and palaeopathological diagnostic criteria for hyperostosis frontalis interna. Int J Osteoarchaeol. 1997;7:157–164. [Google Scholar]
- Broschi C. Testamento di mè D. Carlo Broschi detto Farinelli. Consegnato al Sig. Notaro D.n Lorenzo Gambarini questo dì 20 Febraio 1782. Bologna: Archivio di Stato, Fondo Notarile Gambarini; 1782. [Google Scholar]
- Buikstra JE, Ubelaker DH. Standards for Data Collection from Human Skeletal Remains. Fayetteville, AR: Arkansas Archaeological Survey Research Series 44; 1994. [Google Scholar]
- Burney C. The Present State of Music in France and Italy. 2nd edn. London: Becket and Co; 1773. [Google Scholar]
- Devriendt W, Piercecchi-Marti MD, Adalian P, et al. Hyperostosis frontalis interna: forensic issues. J Forensic Sci. 2005;50:1–4. [PubMed] [Google Scholar]
- Ferembach D, Schwidetky I, Stloukal M. Recommendations for age and sex diagnoses of skeletons. J Hum Evol. 1980;9:517–549. [Google Scholar]
- Hershkovitz I, Greenwald C, Rothschild BM, et al. Hyperostosis frontalis interna: an anthropological perspective. Am J Phys Anthropol. 1999;109:303–325. doi: 10.1002/(SICI)1096-8644(199907)109:3<303::AID-AJPA3>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- Hrycek A, Bloch B, Szołtysik I. Morgagni-Stewart-Morel syndrome in a young man. Wiad Lek. 1989;42:1060–1063. [PubMed] [Google Scholar]
- Jenkins JS. The voice of the castrato. Lancet. 1998;351:1877–1880. doi: 10.1016/s0140-6736(97)10198-2. [DOI] [PubMed] [Google Scholar]
- May H, Peled N, Dar G, et al. Hyperostosis frontalis interna: criteria for sexing and aging a skeleton. Int J Legal Med. 2010a doi: 10.1007/s00414-010-0497-6. DOI 10.1007/s00414-010-0497-6. [DOI] [PubMed] [Google Scholar]
- May H, Peled N, Dar G, et al. Hyperostosis frontalis interna and androgen suppression. Anat Rec. 2010b;293:1333–1336. doi: 10.1002/ar.21175. [DOI] [PubMed] [Google Scholar]
- McKern TW, Stewart TW. Natick, MA: Quartermaster Research and Development Center Environmental Protection Research Division; 1957. Skeletal age changes in young American males. Technical Report EP-45. [Google Scholar]
- Miazgowski T, Eisner M, Czekalski S. Kallman's syndrome combined with aortic valve anomaly and epilepsy. Pol Tyg Lek. 1991;46:380–382. [PubMed] [Google Scholar]
- Néel JL, Ménagé JJ, Guilmot JL, et al. Klinefelter's syndrome and cranial bone lesions with parietal holes syndrome. Nouv Presse Méd. 1974;3:2243–2244. [PubMed] [Google Scholar]
- Nikolić S, Djonić D, Živković V, et al. Rate of occurrence, gross appearance, and age relation of hyperostosis frontalis interna in females. A prospective autopsy study. Am J Forensic Med Pathol. 2010;31:205–207. doi: 10.1097/PAF.0b013e3181d3dba4. [DOI] [PubMed] [Google Scholar]
- Olivier G, Fully G, Tissier G. New estimation of stature and cranial capacity in modern man. J Hum Evol. 1978;7:513–518. [Google Scholar]
- Ortner DJ, Putschar WGJ. Identification of Pathological Conditions in Human Skeletal Remains. Washington, DC: Smithsonian Institution Press; 1985. [Google Scholar]
- Ramchandren S, Liebeskind DS. Headache in a patient with Klinefelter's syndrome and hyperostosis frontalis interna. J Headache Pain. 2007;8:342–344. doi: 10.1007/s10194-007-0426-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rastelli E. Bologna: University of Bologna; 2005. Ricerca metodologica su indicatori scheletrici di eta' adulta su collezioni di epoca moderna (prima meta' del XX secolo) italiane (collezione di Sassari e collezione di Bologna) e portoghesi (Colecção de Esqueletos Identificados, Coimbra) di età e sesso noti. PhD Thesis. [Google Scholar]
- Riggs BL. Overview of osteoporosis. West J Med. 1991;154:63–77. [PMC free article] [PubMed] [Google Scholar]
- Rühli FJ, Böni T, Henneberg M. Hyperostosis frontalis interna: archaeological evidence of possible microevolution of human sex steroids? Homo. 2004;55:91–99. doi: 10.1016/j.jchb.2004.04.003. [DOI] [PubMed] [Google Scholar]
- Sacchi G. Vita del Cavaliere Don Carlo Broschi. Venice: Coleti; 1784. pp. 46–48. [Google Scholar]
- Salmi A, Voutilainen A, Holsti L, et al. Hyperostosis cranii in a normal population. Am J Roentgenol. 1962;87:1032–1040. [PubMed] [Google Scholar]
- Talarico EF, Prather AD, Jr, Hardt KD. A case of extensive hyperostosis frontalis interna in an 87-year-old female human cadaver. Clin Anat. 2008;21:259–268. doi: 10.1002/ca.20613. [DOI] [PubMed] [Google Scholar]
- Verdi L. Il Farinelli a Bologna. Mostra storico-documentaria. Bologna: Museo internazionale e biblioteca della musica di Bologna; 2005. [Google Scholar]
- Yamakawa K, Mizutani K, Takahashi M, et al. Hyperostosis frontalis interna associated with hypogonadism in an elderly man. Age Ageing. 2006;35:202–203. doi: 10.1093/ageing/afj051. [DOI] [PubMed] [Google Scholar]