

Abstract
Background
Interleukin 6 (IL-6) is thought to play important roles in the development of reactive thrombocytosis caused by inflammation by its stimulatory effect on megakaryocytopoiesis. A G/C polymorphism of the IL-6 gene at position -174 has been found to be associated to different transcription rates. Specifically, subjects with the CC genotype showed lower plasma IL-6 levels compared with GC or GG subjects. Given this difference in transcription rates of IL-6 we speculated on different platelet count according to this IL-6 polymorphism.
Methods
The G/C polymorphism of the IL-6 gene at position -174, serum IL-6 concentration and platelet count were prospectively analyzed in 59 (25 women) consecutive healthy subjects.
Results
Subjects who were homozygotes for the C allele at position -174 of the IL-6 gene (Sfa NI genotype) showed significantly lower platelet count than carriers of the G allele, despite similar age, sex, body mass index and proportion of smokers (205400 ± 44088 vs 239818 ± 60194, p = 0.047). This was in parallel to differences in peripheral white blood cell count (5807 ± 1671 vs 6867 ± 1192 × 109/ml, p = 0.01).
Conclusion
This is the first description, to our knowledge, of a genetical influence on basal platelet counts, which appears to be partially dependent on a polymorphism of the IL-6 gene, even in the absence of inflammation.
Background
Interleukin-6 (IL-6) is a pleiotropic cytokine involved in the regulation of the acute phase reaction, immune responses, and hematopoiesis. Earlier studies have found that IL-6 is a potent thrombopoietic factor in vivo in mice acting on maturational stages in megakaryocytopoiesis and promoting platelet production [1]. Human IL-6 was also found as a direct promoter of maturation of megakaryocytes in vitro [2]. In recent reports, circulating IL-6 appeared to be an active mediator involved in the regulation of thrombopoiesis during clonal and reactive thrombocytosis [3,4]. However, at the present moment, there is no evidence that IL-6 is required for normal thrombopoiesis in humans.
A polymorphism in the 5' flanking region of the IL-6 gene alters the transcriptional response to stimuli such as endotoxin and interleukin-1. This G/C polymorphism of the IL-6 gene at position -174 has been found to be associated to different plasma IL-6 levels in healthy volunteers [5]. Given the role of IL-6 in megakaryocytopoiesis we aimed to study the G/C polymorphism of IL-6 in relation with the blood platelet count.
Subjects and Methods
Subjects
Fifty-nine healthy subjects (25 women) were prospectively studied. All subjects were of caucasian origin from Catalonia (northern part of Spain). Inclusion criteria were: 1) absence of any systemic disease, 2) absence of any infections in the previous month. None of the subjects were taking any medication (including glucocorticoids or estrogens) or had any evidence of metabolic disease. Liver disease and thyroid dysfunction were specifically excluded by biochemical workup. The protocol was approved by the Hospital Ethics Committee, and informed consent was obtained from each subject.
Platelet count was determined by routinary laboratory tests (Coulter Electronics, Hialeah FL).
Serum interleukin-6 levels were measured using a commercial immunoassay (MEDGENIX IL-6 EASIA™, BioSource Europe S.A., Zoning Industriel B-6220, Fleunes, Belgium), with coefficients of variation lower than 6%. The minimum detectable doses of IL-6 was 0.094 pg/ml.
Restriction fragment length polymorphism (RFLP)-IL-6 gene analysis
The Sfa NI (restriction enzyme) polymorphism is due to a replacement of G by C at position 174, and primers were designed to amplify the promoter region of IL-6 gene. The primers used in the PCR were: 5' TGACTTCAGCTTTACTCTTTGT 3' and 5' CTGATTGGAAACCTTAT TAAG 3'. The reaction was carried out in a final volume of 50 μL containing 1.5 mmol/L of MgCl2, 0.2 mmol/L of each dNTP (Boehringer MannheimTM, Mannheim, Germany), 0.2 mmol/L of each primer and 2.5 unit of Taq polimerase (Gibco BRL). DNA was amplified during 35 cycles with an initial denaturation of 10 minutes at 94°C and a final extension of 10 m at 72°C. The cycle program consisted in 1 minute denaturation at 94°C,1 minute and 35s annealing at 55°C and 1 m extension at 72°C. PCR products were digested with SfaNI restriction enzyme at 37°C overnight and electrophoresed on a 2% agarose gel. SfaNI RFLP was detected by ethidium bromide staining.
DNA was extracted from cellular blood components by the salting-out method. The polymerase chain reaction was used to detect the IL-6 SfaNI RFLP. The identified genotypes were named according to the presence or absence of the enzyme restriction sites, so SfaNI (G/G), (G/C), and (C/C) are homozygotes for the presence of the site (140/58 bp), heterozygotes for the presence and absence of the site (198/140/58 bp), and homozygotes for the absence of the site (198 bp), respectively. The frequency of the alleles in a large sample of subjects was C: 0.55, G: 0.45. The Χ2 value of a goodness-of-fit statistics to test for Hardy-Weinberg equilibrium was 1.3 (p = 0.52, df = 1).
Statistical analysis
Descriptive results of continuous variables are expressed as mean ± SD. Comparison of variables between groups of subjects was performed using unpaired t test.
Results
Clinical and biochemical characteristics of the subjects at the time of entry into the study are shown on Table 1. The samples from 59 subjects were divided into two groups on the basis of the IL-6 genotype. Forty-four subjects had a G at position -174 of the IL-6 gene, 29 heterozygotes (C/G) and 15 homozygotes (G/G). Fifteen subjects were homozygotes for the presence of C at this position.
Table 1.
General characteristics of the Study Subjects
| Variable | C/C | G/C and GG | P |
| N | 15 | 44 | - |
| Men/women | 8/7 | 26/18 | NS |
| Age (years) | 36.4 ± 10.6 | 40.4 ± 8.5 | NS |
| Body mass index | 26.07 ± 5.1 | 26.8 ± 4.8 | NS |
| (Kg/m2) | |||
| Smokers (yes/no) | 4/11 | 12/32 | NS |
| Platelet count (/μl) | 205400 ± 44088 | 239818 ± 60194a | 0.04 |
| Median (range) | 201.000 (135000-298000)b | 223.500 (159000-477000)c | |
| WBC (× 109/ml) | 5807 ± 1671 | 6867 ± 1192 | 0.01 |
| Hematocrit (%) | 40.4 ± 5.4 | 42.2 ± 4.8 | NS |
| Circulating IL-6 (pg/ml)* | 6.8 ± 1.7 | 10.3 ± 6.9 | 0.07 |
C/C, C/G and G/G define the allele polymorphism of the promoter of interleukin-6 gene. Data are provided as mean ± SD. * IL-6, circulating interleukin 6, which was determined in 30 subjects, 10 of whom with the C/C allele; WBC, peripheral white blood cells. a. After excluding the outlier, the differences remained significant at a p = 0.046. b. There was only one subject below the lower normal range of 150.000 platelets/μl and 6 between 160.000-185.000/μl. c. The maximum platelet level is 353.000/μl after excluding the outlier. The normal range, mean and median of platelet counts are 230.970, 220500 (150.000-400.000) /ml.
Platelet count showed a normal distribution (Figure 1). Subjects who were homozygotes for the C allele, associated to lower plasma levels of IL-6 in a recent study [5], were similar in age, sex, body mass index and proportion of smokers in comparison with carriers of the G allele (Table 1). The former subjects showed significantly lower platelet count than carriers of the G allele (mean difference -34.418 platelets, with a Levene's test for equality of Variances: F = 0.74, p = 0.39, indicating a similar variance for platelet count in both groups (Table 1) (Figure 2).
Figure 1.
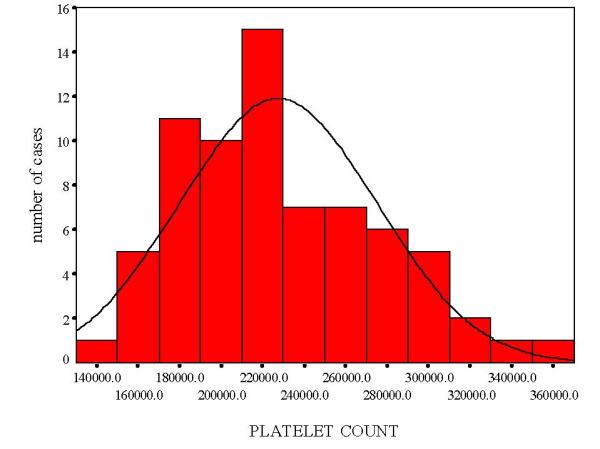
Histogram showing the normal distribution of platelet count.
Figure 2.
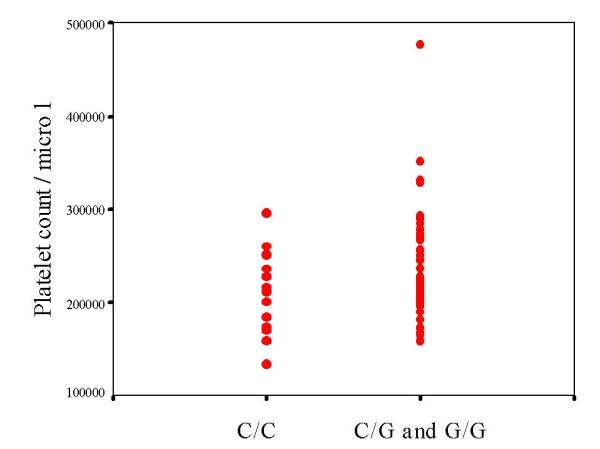
Peripheral platelet count according to interleukin-6 genotype. After excluding the outlier, the differences remained significant at a p = 0.046.
Discussion
When comparing constructs of the 5' flanking region of IL-6 in a luciferase reporter vector transiently transfected intoHeLa cells, the -174C construct showed lower expression than the -174 G construct [5]. This different transcription rate was supported by the in vivo observation that IL-6 levels were lower in normal subjects with the CC genotype [5]. We have found a tendency towards lower levels of IL-6 in CC homozygotes using a different assay. Unlike other cytokines, IL-6 is unusual, in that its major effects take place at sites distinct from its origin and are consequent upon its circulating concentrations. For this reason, it is called the endocrine cytokine [6]. For instance, increased circulating levels of IL-6 and C-reactive protein have been recently associated with mortality in healthy older persons [7]. Serum IL-6 concentration is tightly regulated and circulates in proportion to different metabolic abnormalities such as lipid levels [8], insulin resistance and blood pressure [9].
The importance of this observation is that it is the first description of a molecular influence of basal platelet counts. The findings of the present study suggest that subjects with the G allele would be prone to a procoagulant state. This matter is of considerable importance in atherosclerosis. It has been speculated that IL-6 might play a key role in the development of coronary disease through a number of metabolic, endothelial and procoagulant mechanisms [7,8,9,10]. In fact, circadian interrelationships among levels of plasma fibrinogen, blood platelets and serum interleukin 6 have been recently reported [11]. Although basal interleukin 6 levels were not statistically different between genotypes in this report (p = 0.07), the study of circadian IL-6 levels will shed light on differences of transcription rate attributed to IL-6 gene polymorphism. The effect of IL-6 on platelets, fibrinogen activation and coagulation would lead to a procoagulant state, as demonstrated in an experimental model of endotoxemia [12]. In fact, the asymptomatic homozygous subjects with the G allele showed an 11% greater carotid artery intima-media thickness than CC homozygous for the C allele, as indicative of early atherosclerosis [13]. Furthermore, diabetic patients with vascular disease show significantly increased platelet count [14]. We have hypothesized that inflammation is inherent to insulin resistance of type 2 diabetic patients that contribute to their chronic diabetic complications [15]. Given that patients with the G allele also showed significantly higher area under the curve of glucose after an oral glucose tolerance test in a recent study [16], a relationship between concomitant higher glucose levels and platelet count attributed to IL-6 gene polymorphism cannot be excluded.
Under physiological conditions, IL-6 would play a role to regulate homeostasis by maintaining the level of platelets and leukocytes. In fact, we have also described that the IL-6 -174 gene polymorphism was associated to peripheral white blood cell count in healthy subjects [16], specifically neutrophils and lymphocytes, reinforcing the potential importance of IL-6 in hematopoiesis [17]. Peripheral white blood cell count constitutes another risk factor for atherosclerosis [18]. Elevated serum IL-6 levels cannot be excluded, however, to constitute an anti-inflammatory attempt [17] to fight against a chronic inflammatory process (atherosclerosis), being the enhanced hematopoiesis a byproduct.
Conclusion
A polymorphism of the IL-6 gene influences the platelet count in healthy volunteers even in the absence of inflammation. Whether this polymorphism leads to differences in reactive thrombocytosis merits further research.
Pre-publication history
The pre-publication history for this paper can be accessed here:
http://www.biomedcentral.com/content/backmatter/1471-2350-2-6-b1.pdf
Acknowledgments
Acknowledgements
This work was partially supported by grant grant CICYT SAF 98-0130, and grant 00/0024-01 from the Fondo de Ivestigaciones Sanitarias, National Health Institute.
Competing interests
Have you in the past five years received reimbursements, fees, funding, or salary from an organisation that may in any way gain or lose financially from the publication of this paper? NO
Do you hold any stocks or shares in an organisation that may in any way gain or lose financially from the publication of this paper? NO
Do you have any other financial competing interests? NO
Are there any non-financial competing interests you would like to declare in relation to this paper? NO
Contributor Information
José-Manuel Fernandez-Real, Email: endocrino@htrueta.scs.es.
Joan Vendrell, Email: jvo@galenics.com.
Cristobal Richart, Email: jvo@galenics.com.
Cristina Gutierrez, Email: endocrino@htrueta.scs.es.
Wifredo Ricart, Email: endocrino@htrueta.scs.es.
References
- Ishibashi T, Kimura H, Shikama Y, Uchida T, Kariyone S, Hirano T, Kishimoto T, Takatsuki F, Akiyama Y. Interleukin 6 is a potent thrompoietic factor in vivo in mice. Blood. 1989;74:1241–1244. [PubMed] [Google Scholar]
- Ishibashi T, Kimura H, Uchida T, Kariyone S, Friese P, Burstein SA. Human interleukin 6 is a direct promoter of maturation of megakaryocytes in vitro. Proc Natl Acad Sci USA. 1989;86:5953–5957. doi: 10.1073/pnas.86.15.5953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsu HC, Tsai WH, Jiang ML, Ho CH, Hsu ML, Ho CK, Wang SY. Circulating levels of thrombopoietic and inflammatory cytokines in patients with clonal and reactive thrombocytosis. J Lab Clin Med. 1999;134:392–397. doi: 10.1016/s0022-2143(99)90154-3. [DOI] [PubMed] [Google Scholar]
- Weisdorf DJ, DeFor T, Nichol J, Panoskaltsis-Mortari A, Blazar BR. Thrombopoietic cytokines in relation to platelet recovery after bone marrow transplantation. Bone Marrow Transplant. 2000;25:711–715. doi: 10.1038/sj.bmt.1702221. [DOI] [PubMed] [Google Scholar]
- Fishman D, Faulds G, Jeffery R, Mohamed-Ali V, Yudkin JS, Humphries S, Woo P. The effect of novel polymorphisms in the interleukin 6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J Clin Invest. 1998;102:1369–1376. doi: 10.1172/JCI2629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris TB, Ferrucci L, Tracy RP, Corti MC, Wacholder S, Ettinger WH, Jr, Heimovitz H, Cohen HJ, Wallace R. Associations of elevated interleukin-6 and C-reactive protein levels with mortality in the elderly. Am J Med. 1999;106:506–512. doi: 10.1016/S0002-9343(99)00066-2. [DOI] [PubMed] [Google Scholar]
- Papanicolau DA, Vgontzas AN. Interleukin-6: The endocrine cytokine. J Clin Endocrinol Metab. 2000;85:1331–1332. doi: 10.1210/jcem.85.3.6582. [DOI] [PubMed] [Google Scholar]
- Fernández-Real JM, Broch M, Vendrell J, Richart C, Ricart W. Interleukin 6 Gene Polymorphism and Lipid Abnormalities in Healthy Subjects. J Clin Endocrinol Metab. 2000;85:1334–1339. doi: 10.1210/jcem.85.3.6555. [DOI] [PubMed] [Google Scholar]
- Fernández-Real JM, Vayreda M, Richart C, Gutiérrez C, Broch M, Vendrell J, Ricart W. Circulating interleukin 6 levels, blood pressure and insulin sensitivity in apparently healthy men and women. J Clin Endocrinol Metab. 2001;86:1154–1159. doi: 10.1210/jcem.86.3.7305. [DOI] [PubMed] [Google Scholar]
- Yudkin JS, Kumari M, Humphries SE, Mohamed-Ali V. Inflammation, obesity,stress and coronary heart disease: is interleukin-6 the link?. Atherosclerosis. 2000;148:209–214. doi: 10.1016/S0021-9150(99)00463-3. [DOI] [PubMed] [Google Scholar]
- Kanabrocki EL, Sothern RB, Messmore HL, Roitman-Johnson B, McCormick JB, Dawson S, Bremner FW, Third JL, Nemchausky BA, Shirazi P, Scheving LE. Circadian interrelationships among levels of plasma fibrinogen, blood platelets, and serum interleukin 6. Clin Appl Thromb Hemost. 1999;5:37–42. doi: 10.1177/107602969900500108. [DOI] [PubMed] [Google Scholar]
- Van der Poll T, Levi M, Hack CE, ten Cate H, van Deventer SJ, Eerenberg AJ, de Groot ER, Jansen J, Gallati H, Buller HR, et al. Elimination of interleukin 6 attenuates coagulation activation in experimental endotoxemia in chimpanzees. J Exp Med. 1994;179:1253–1259. doi: 10.1084/jem.179.4.1253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rauramaa R, Vaisanen SB, Luong LA, Schmidt-Trucksass A, Penttila IM, Bouchard C, Toyry J, Humphries SE. Stromelysin-1 and interleukin 6 gene promoter polymorphisms are determinants of asymptomatic carotid artery atherosclerosis. Arterioscler Thromb Vasc Biol. 2000;20:2657–2662. doi: 10.1161/01.atv.20.12.2657. [DOI] [PubMed] [Google Scholar]
- Brown AS, Hong Y, de Belder A, Beacon H, Beeso J, Sherwood R, Edmonds M, Martin JF, Erusalimsky JD. Megacaryocyte ploidy and platelet changes in human diabetes and atherosclerosis. Arterioscler Thromb Vasc Biol. 1997;17:802–807. doi: 10.1161/01.atv.17.4.802. [DOI] [PubMed] [Google Scholar]
- Fernández-Real JM, Ricart W. Insulin resistance and inflammation in an evolutionary perspective. The contribution of cytokine genotype/phenotype to thriftiness. Diabetologia. 1999;42:1367–1374. doi: 10.1007/s001250051451. [DOI] [PubMed] [Google Scholar]
- Fernández-Real JM, Broch M, Vendrell J, Gutiérrez C, Casamitjana R, Pugeat M, Richart C, Ricart W. Interleukin 6 gene polymorphism and insulin sensitivity. Diabetes. 2000;49:517–520. doi: 10.2337/diabetes.49.3.517. [DOI] [PubMed] [Google Scholar]
- Xing Z, Gauldie J, Cox G, Baumann H, Jordana M, Lei X-F, Achong MK. IL-6 is an antiinflammatory cytokine required for controlling local or systemic acute inflammatory responses. J Clin Invest. 1998;101:311–320. doi: 10.1172/JCI1368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Facchini F, Hollenbeck CB, Chen YN, Chen YD, Reaven HM. Demonstration of a relationship between white blood cell count, insulin resistance, and several risk factors for coronary heart disease in women. J Intern Med. 1992;232:267–272. doi: 10.1111/j.1365-2796.1992.tb00582.x. [DOI] [PubMed] [Google Scholar]