

Abstract
Objective
The aim of this article is to report how Neuro Emotional Technique (NET) was used for precompetitive anxiety in 2 power-lifting athletes.
Clinical Features
Two athletes (1 elite and 1 novice), who were participating in major competitions within 2 weeks of testing, were assessed for cognitive and somatic anxiety levels pre- and postintervention. Three psychometrics were used to measure mental state (cognitive anxiety): the Sports Competitive Anxiety Test, the Depression Anxiety Stress Scales, and the SF-36v2 Health Survey. To assess somatic anxiety, saliva samples were collected and screened for cortisol and dehydroepiandrosterone.
Intervention and Outcome
The intervention was performed by a doctor of chiropractic and consisted of one 30-minute session of NET that focused on the athletes' concerns regarding the upcoming competitions. The results showed reductions in reported subjective anxiety levels and changes in the salivary hormone profile of both athletes following the intervention, with the more remarkable changes occurring in the novice athlete. The reduction in reported cognitive anxiety levels and the change in somatic anxiety markers may be the result of the mind-body intervention. However, these changes may also be attributed to other factors, such as the natural course of anxiety during competition. An experimental trial would be required to determine the effectiveness of NET for reducing precompetitive anxiety of power-lifters.
Conclusion
Neuro Emotional Technique may have helped these power-lifters control emotional arousal and precompetitive anxiety. However, caution is warranted when using these results to draw conclusions or when extrapolating these results to other settings.
Key indexing terms: Weight lifting, Sports, Anxiety, Alternative therapies, Mind-body therapies, Chiropractic
Introduction
For optimal athletic performance, athletes must able to control anxiety. Although a certain level of arousal can enhance performance, hyperarousal can quickly diminish performance.1-3 In the mid-1960s, Liebert and Morris4 were among the first to recognize the multidimensionality of anxiety. Although there was considerable debate as to the exact constituents, it is now generally accepted that there are clearly cognitive and somatic components of anxiety.4-6 Cognitive anxiety refers to any negative expectations or concerns about oneself, the situation, or possible consequences,7 and is clearly conscious. On the other hand, elements of somatic anxiety are disputed. Martens et al8 describe it as “the physiological and affective elements of the anxiety experience that develop directly from autonomic arousal,” and make no reference to it being conscious or not. Alternatively, Woodman and Hardy9 describe somatic anxiety as “the perception of one's physiological arousal,” implying that it is also a conscious experience. For the sake of clarity, the former definition of somatic anxiety will be used and will pertain to either conscious or nonconscious events. In any case, cognitive anxiety and somatic anxiety are largely thought to be conceptually independent.10 Therefore, because either component can potentially impact performance, both cognitive anxiety and somatic anxiety have been considered in this report.
Although it is possible that athletes from many sports can experience performance anxiety, the focus of this study was power-lifting athletes. Power-lifters were chosen for this preliminary case series for a number of reasons. First, they are solo athletes, in that when they compete, they compete alone. This characteristic makes it theoretically easier to study changes in individuals compared with athletes in team sports. Second, they often compete in front of an audience, which in itself can induce performance anxiety.11-14
Neuro Emotional Technique (NET) is a stress-reduction intervention that has been shown to diminish emotional arousal in phobics.15,16 Hence, it was hypothesized that NET may be effective in lowering precompetitive anxiety in athletes as well. Therefore, the aim of this case study is to describe how NET was used with 2 power-lifting athletes who reported experiencing precompetitive anxiety.
Case reports
Two athletes volunteered to participate in this report: 1 male elite competitor and 1 female novice competitor. With both athletes facing major competitions within 2 weeks of testing, they both reported experiencing precompetitive anxiety. For example, the elite athlete, who was competing in a power-lifting World Championships, reported having mild insomnia, increased irritability, and slight edginess. The novice athlete was competing for the first time and reported having concerns whether or not she was good enough or ready to compete (ie, self-efficacy concerns), and she had had thoughts about pulling out of the competition (ie, avoidance behavior). Before being enrolled and after treatment procedures were fully explained, both athletes were given a participant information sheet and signed an informed consent, giving permission to have their personal health information published. The participants were then assessed for cognitive anxiety levels and adrenal function pre- and postintervention. To assess cognitive anxiety levels, 3 commonly used psychological surveys were implemented: (1) the Sports Competitive Anxiety Test (SCAT), (2) the Depression Anxiety Stress Scales (DASS), and (3) the SF-36v2 (SF-36) Health Survey.
The SCAT is a 15-item self-report instrument used to measure performance anxiety traits.8 The participant grades each item on a 3-point Likert scale: rarely, sometimes, and often. Scores can range from 10 to 30, with the higher score meaning the greater the tendency toward competitive anxiety.8 The SCAT has been shown to be a consistently valid and reliable measure of competitive trait anxiety as evidenced by high internal consistency (KR-20 values from 0.95 to 0.97) and high test-retest reliability (M retest reliability = 0.77).8
The DASS is a set of 3 self-report scales measuring the affective states of depression (D), anxiety (A), and stress (S). Each of the 21 items is scored from “0” (“Did not apply to me at all”) to “3” (“Applied to me very much or most of the time”). A template is used to score the test, and score is achieved for each of the 3 categories. For each category, scores can range from 0 to 28+, with healthy people being at the lower end of the range. The DASS was found to have excellent reliability and adequate convergent and discriminant validity in healthy populations.17
The SF-36 is a generic 36-item multidimensional self-report, a quality of life scale that has been shown to adequately measure aspects of general health in adults.18-20 It yields an 8-scale profile of functional health and well-being scores plus summary scores for physical and mental health.19,20 Because of the nature of the NET intervention, this study will highlight only the 3 subscales thought to be related to mental functioning: social functioning (SF), role emotional (RE) and mental health (MH).21 The Mental Component Summary score was excluded from interpretation because its validity as an accurate summary of subscale scores is questionable.22 In addition, although the SF-36 subscale scores have been shown to have limitations within specific groups (eg, the elderly23) and with certain conditions (eg, Parkinson disease24), for the population under investigation, the instrument has been shown to be of value, demonstrating satisfactory internal consistency,20,25 construct validity,25 and test-retest reliability,25 including good test-retest reliability over a short interval.
The athletes took each questionnaire twice: the day before the NET intervention and then 2 days following. A positive treatment effect may be indicated by a reduction in SCAT scores; a reduction in the A and S scores of the DASS; or an increase in the SF, RE, or MH subscores of the SF-36.
Two tests of adrenal function were used to assess somatic anxiety: (1) waking salivary cortisol and (2) waking salivary dehydroepiandrosterone (DHEA). For each sample, assessment was performed on 50 to 100 μL of saliva by means of commercial immunoenzymatic kits (ARL, Melbourne, Australia) for direct salivary assay of cortisol and DHEA-S. Interassay coefficient of variation was less than 10%; and intraassay coefficient of variation was less than 7%, with a minimum detectable concentration of 0.5 ng/mL for cortisol and 25 pg/mL for DHEA-S. Saliva testing was chosen over blood testing because of its ease of collection. It is widely accepted that blood cortisol levels rise in response to stressors,26,27 and there is a reliable direct correlation between blood cortisol and salivary cortisol levels.28 Although there is significant controversy about the usefulness of cortisol testing in general, waking cortisol levels appear to show acceptable reliability.29 In addition, samples of saliva were analyzed for DHEA levels. Dehydroepiandrosterone, the most abundant steroid hormone in the body, has been shown to significantly buffer the stress response.30-32 It was expected that, following the NET intervention, waking salivary cortisol levels would decrease and salivary DHEA levels would increase.
Each athlete received a single 30-minute NET session by the same certified NET practitioner, which was the only intervention the athletes reported to receive during their participation. Neuro Emotional Technique is considered an alternative stress-reduction technique. Its aim is to remove neurological abnormalities that are thought to have a specified physiopathological pattern.33
During the NET procedure, various psychological components of the anxious state were considered: (1) cognitions (thoughts about the anxiety-producing upcoming competition and the participants' response to it), (2) emotions (participants' affect in response to the upcoming competition), and (3) behaviors (participants' behaviors in response to the upcoming competition, for example, avoidance).34 These various psychological components were explored for a physiological reaction in the participant. The manual muscle test is used throughout the NET procedure as an assessment of a participant's physiological reactivity, the 2 of which have previously been shown to be correlated.15,35,36
The NET procedure involved a series of well-defined steps (Fig 1) that aims at addressing each of these components. Once a physiological reaction is found, the practitioner helps the participant identify the specific emotion using the principle from traditional Chinese medicine that meridians/organs and emotions are coupled37 (Fig 2). The participant then decides how the specific emotion fits the distressing situation. Sometimes, a similar distressing situation is identified earlier in life as well. While the patient thinks about the distressing situation and feels the emotion that was found to be associated, a mechanical force is applied to specific spinal levels (Table 1) during a full respiratory cycle. The procedure is concluded when the patient no longer feels distress or discomfort associated with the cognitive statement or recollection, and as a result can resist the downward pressure of the muscle test.34 Following the intervention, patients frequently report feeling subjective relief.34 Both NET sessions were held in a quiet, private room at the gym where the athletes trained.
Fig 1.
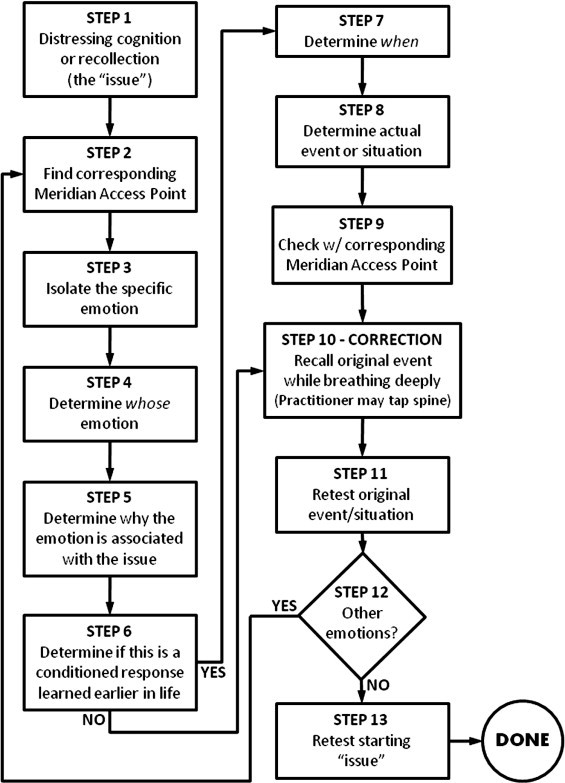
Neuro Emotional Technique protocol flowchart.33
Fig 2.
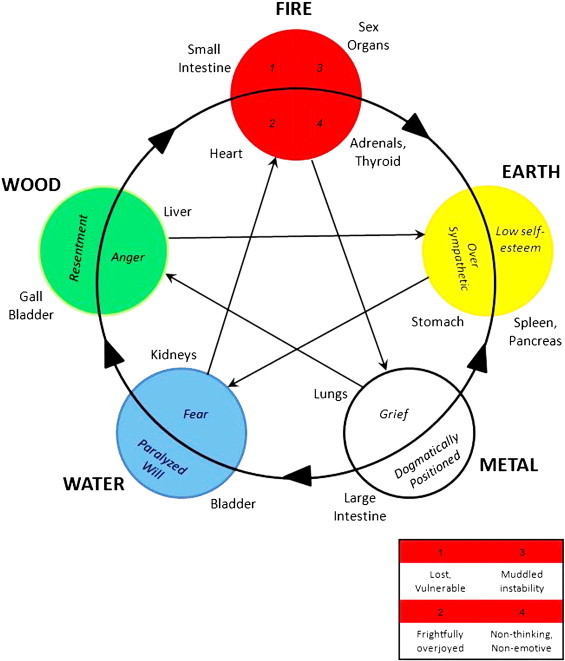
The meridian/organ-emotion relationship.33 (Color version of figure is available online.)
Table 1.
Meridian/organ spinal levels33
| Meridian access point | Spinal levels addressed |
|---|---|
| Earth element | |
| Stomach | T8-T10-T12 |
| Spleen | T1-T5-T9 |
| Pancreas | T5 |
| Metal element | |
| Large intestine | L5 |
| Left lung | T1-T8-L2 |
| Right lung | T2-T9-L3 |
| Water element | |
| Bladder | L5 |
| Kidney | T1-T5-T8 |
| Wood element | |
| Gallbladder | T4 |
| Liver | T2-T5-T8 |
| Fire element | |
| Small intestine | L5 |
| Heart | T2-T8-T12 |
| Thyroid | C1-C4-C7 |
| Adrenals | T7-T9-T11 |
| Prostate | L5 |
| Testes/ovaries/uterus | Bilateral SI joints-L3-L5-coccyx |
| Pituitary | C2-C5-T1 |
| Other | |
| Governing vessel | T3-T6 |
| Conception vessel | T3-T6 |
There was an improvement in both the cognitive and somatic anxiety of both athletes. The changes exhibited by the novice athlete were more remarkable than for the elite athlete. See Table 2 for the results of the psychometric testing and Table 3 for the results of the salivary hormone profile.
Table 2.
Psychometric scores: SCAT, DASS, and SF-36 (specific scale scores)
| SCAT |
DASS |
SF-36 |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| D |
A |
S |
SF |
RE |
MH |
|||||||||
| Athlete | Pre | Post | Pre | Post | Pre | Post | Pre | Post | Pre | Post‡ | Pre | Post | Pre | Post |
| Novice | 24 | 20 | 4 | 0 | 14b | 4 | 18a | 0 | 56.8d | 56.8d | 55.9d | 55.9d | 50.0f | 52.8e |
| Elite | 22 | 19 | 6 | 4 | 8 | 10a | 42c | 34c | 40.5h | 45.9g | 32.6h | 32.6h | 35.9h | 38.7h |
For a table containing all SF-36 scale scores, see the Supplemental Material (Supplement 4). Pre, Preintervention; Post, postintervention.
aMild, bmoderate, and cextremely severe. All other values considered “normal.”
dExcellent, every good, fgood, gfair, and hpoor.
Table 3.
Salivary hormone profile (raw scores)
| Cortisol (nmol/L) |
DHEA (nmol/L) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Pre |
Post |
Pre |
Post |
|||||
| Athlete | −2a | −1 | +1 | +2 | −2 | −1 | +1 | +2 |
| Novice | 6 | 8 | 4 | 12 | 15.3 | 15.7 | 26.9 | 17.2 |
| Elite | 17 | 25 | 23 | 20 | 5.7 | 8.2 | 8.1 | 8.9 |
Days from intervention (intervention = day 0).
Discussion
Anxiety in sport is commonplace. Although a certain level of anxiety enhances performance, uncontrolled emotions and negative cognitions can have adverse effects. Various techniques have been used to help athletes control their emotions. These include hypnosis, biofeedback training, progressive relaxation, visuomotor behavior rehearsal, autogenic training, meditation, positive self-monitoring, thought-stopping, various self-talk techniques, induced affect, and cognitive-behavioral therapies.8 The evidence supporting the durable effectiveness of these methods for the general population is limited, mostly underpowered, and often contradictory.38-42 The evidence supporting the effectiveness of these methods for athletes is weaker still. It is apparent that research is greatly needed in this area. Moreover, it is apparent that a robust intervention to consistently control performance anxiety is also critically needed.
The changes exhibited by these 2 athletes are encouraging. However, full-scale randomized trials are needed to qualify the effectiveness of NET in reducing precompetitive anxiety. Until that time, the interpretation of the results of this report is limited.
The minimally clinically important difference (MCID) is a useful tool for reporting changes in participant outcomes. It can be defined as “the smallest change in measurement that signifies an important difference” and may refer to either an improvement or a worsening.43 Unfortunately, most of the measures chosen for this report do not yet have established MCIDs; therefore, the significance of the observed changes is open to interpretation.
The SF-36 is the one measure used in this study that has a documented MCID: 3 to 5 points for each subscale score.44 Therefore, the only clinically significant change (>3 points) in subscale score occurred for the elite athlete in the SF subscale. Keeping in mind that all of the SF-36 mental health scores for this athlete were in the fair-to-poor range, a 5.4-point improvement may be of great importance for this individual. Without controlling for other factors, it cannot be determined if this change was due to the NET intervention or other reasons. In addition, it is interesting note that many of the physical component subscale scores (Supplement 4) for the elite athlete also improved considerably, which may have contributed to the improvement in the mental health subscales as well.
During the analysis of the SCAT and DASS, in the absence of recognized MCIDs, a 3-point and a 7-point change in score (respectively) was regarded as clinically significant.*8,17 Both athletes achieved a clinically significant drop in SCAT score, indicating a reduction in cognitive anxiety. In addition, for the DASS, both athletes achieved a significant drop in their respective A scale and S scale scores; and the novice athlete achieved a significant drop in her D scale score. Although it is possible that these significant improvements may be attributed to the NET intervention, they also may be attributed to confounding factors. For the elite athlete, there was a 2-point increase in his A scale score and a 2-point decrease in his D scale score following the intervention, both of which were considered insignificant. However, the 2-point increase in this athlete's A scale score indicates that he went from “normal” to “mild” anxiety, which may have significance to this individual. A change of 1 standard deviation of the mean scores or levels from normative data was used to determine clinical significance.
For analysis of the salivary hormone profile, which also lacked standardized MCIDs, a change in 1 nmol/L for salivary cortisol and 0.5 nmol/L for salivary DHEA was considered clinically significant.†45,46 Salivary cortisol levels for both athletes dropped significantly the day after the intervention. However, on the second day following the intervention, cortisol levels for the elite athlete continued to drop, whereas those for the novice rose again. Because salivary cortisol levels have been positively correlated with stress levels,27 the changes on the day following the intervention could be considered a reduction in somatic anxiety. Salivary DHEA levels also changed following the intervention. Levels for the novice athlete rose significantly on the day following the NET intervention; and although they dropped again, they remained significantly elevated on the second day after the intervention (compared with before the intervention). For the elite athlete, there was no significant change in DHEA levels 1 day after the intervention; but there was a significant difference 2 days afterward. Increases in DHEA levels signify an increased capacity to resist the effects of stress.31 Whether or not it was the NET intervention that caused the changes in hormone levels cannot be deduced.
However, it is hypothesized that NET may have contributed to some of the changes in outcome measures by the mechanism described below. According to Edler as cited in Cox,10 there are 5 different fears often associated with anxiety: (1) threat to self-esteem as a result of failure, (2) threat of personal harm, (3) unpredictability or fear of the unknown, (4) fear of disruption of daily habits, and (5) fear of being negatively evaluated by others. It is speculated that these fears are also commonly present in athletes and may contribute to the anxiety felt before a competition. Athletes may be able to identify with these fears, yet may not know exactly why they are experiencing them—and therefore can do nothing to alleviate them.
It is well understood that past emotional trauma can lead to learned emotional responses,47 such as a conditioned fear. As a result, certain physiopathological and behavioral patterns may emerge.47,48 Under normal conditions, in time, these learned responses become extinct; and the physiopathological and behavioral patterns resolve. However, occasionally, this does not happen; and both persist.49 It is further speculated that, in some cases, precompetitive anxiety may be the result of a conditioned fear response. It is thought that NET allows for the extinction of a conditioned response by encouraging the participant to reexperience the emotion associated with the anxiety-producing event in a safe and supportive environment. Therefore, because NET is thought to encourage the extinction of adverse emotionally driven conditioned responses,16,33 it is hypothesized that NET would be effective in lessening precompetitive anxiety.
Limitations
The changes observed in the anxiety markers of these athletes might be attributable to other variables. For example, the athletes might have been experiencing high levels of anxiety (for reasons unknown to the investigator) before testing and intervention, which may have then resolved naturally.50 Another explanation of the observed reduction in anxiety might be that the athletes used another way to self-manage their stress. Alternatively, the tests administered might have produced inaccurate results. For instance, preintervention testing might have revealed anxiety when there was actually none (type I error or a false-positive result); or postintervention testing might have showed no anxiety when there actually was (type II error or a false-negative result). In addition, a type III error may have been made, where the wrong tests were used to measure the construct of precompetitive anxiety.
Because of the nature of a case report, caution must be used when drawing conclusions and generalizations from these results. Limitations of this study include those for any case report. This article was qualitative by design, and not quantitative, without controlled conditions and without follow-up. Therefore, no cause-and-effect relationship can be established; and the results may not be representative of the general group or population. As a result, extrapolating these results to other athletes is not warranted. However, when little research on a topic exists, as is the case with the use of NET with athletes, case reports lend themselves to both generating and testing hypotheses51; therefore, they are worthwhile and contribute to the scientific literature.
Another limitation of this study was that participant adherence to study protocol could not be strictly monitored during saliva sample collection. Because waking samples were requested, adherence was left to the fidelity of each participant to follow the outlined procedure. Criticism may also be presented regarding the broadness of the variables measured. Future trials may want to narrow the scope. For example, a future trial may focus on assessing either cognitive anxiety or somatic anxiety specifically. Other possible avenues of exploration include the real-time use of NET to diminish competitive anxiety (ie, anxiety experienced by athletes during actual competition), such as after a poor shot during a golf match.
In addition, because it was qualitative in design, this study may have been strengthened by the inclusion of comments by the participating athletes. For instance, it would have been interesting to note what the athletes thought of the NET intervention or if they could report any other subjective observations about how they felt regarding their upcoming competitions. It also would have been interesting to report the actual results of their respective competitions and if they thought that the intervention had any impact on their performance.
Conclusion
For these power-lifters, it appears that NET may have impacted both the cognitive and somatic components of their anxiety. However, NET's effectiveness in this arena can only be established following a full-scale, randomized, controlled clinical trial with adequate follow-up and homogenized samples. Although the results of this study are encouraging, drawing definitive conclusions would be premature.
Funding sources and potential conflicts of interest
No external funding was received in the preparation of this manuscript. The author reports no conflict of interest.
Footnotes
A change in 1 standard deviation of the mean scores or levels from normative data was used to determine clinical significance.
A change in 1 standard deviation of the mean scores or levels from normative data was used to determine clinical significance.
Appendix A.
. SF-36 scores (all subscales, raw scores)
References
- 1.Hanin Y.L., editor. Emotions in sport. Human Kinetics; Leeds, UK: 2000. pp. 26–27. [Google Scholar]
- 2.Woodman T., Hardy L. Stress and anxiety. In: Singer R.N., Hausenblas H.A., Janelle C.M., editors. Handbook of sport psychology. John Wiley and Sons; New York: 2001. pp. 290–318. [Google Scholar]
- 3.Zaichowsky L.D., Baltzell A. Arousal and performance. In: Singer R.N., Hausenblas H.A., Janelle C.M., editors. Handbook of sport psychology. John Wiley and Sons; New York: 2001. pp. 319–339. [Google Scholar]
- 4.Liebert R.M., Morris L.W. Cognitive and emotional components of test anxiety: a distinction and some initial data. Psychol Rep. 1967;20(3):975–978. doi: 10.2466/pr0.1967.20.3.975. [DOI] [PubMed] [Google Scholar]
- 5.Hardy L., Whitehead R. Specific modes of anxiety and arousal. Curr Psychol. 1984;3(3):14–24. [Google Scholar]
- 6.Lacey J.I. Somatic response patterning and stress: some revisions of activation theory. In: Appley M.H., Turnbull R., editors. Psychological stress: issues in research. Appleton-Century-Crofts; New York: 1967. pp. 14–42. [Google Scholar]
- 7.Morris L.W., Davis M.A., Hutchings C.H. Cognitive and emotional components of anxiety: literature review and a revised worry-emotionality scale. J Educ Psychol. 1981;73(4):541–555. [PubMed] [Google Scholar]
- 8.Martens R., Vealey R.S., Burton D. Human Kinetics; London: 1990. Competitive anxiety in sport. [Google Scholar]
- 9.Woodman T., Hardy L. The relative impact of cognitive anxiety and self-confidence upon sport performance: a meta-analysis. J Sports Sci. 2003;21(6):443–457. doi: 10.1080/0264041031000101809. [DOI] [PubMed] [Google Scholar]
- 10.Cox R.H. 6th ed. McGraw-Hill; New York: 2006. Sport psychology: concepts and applications. [Google Scholar]
- 11.Finn A.N., Sawyer C.R., Schrodt P. Examining the effect of exposure therapy on public speaking state anxiety. Commun Educ. 2009;58(1):92–109. [Google Scholar]
- 12.Osborne M.S., Kenny D.T. The role of sensitizing experiences in music performance anxiety in adolescent musicians. Psychol Music. 2008;36(4):447–462. [Google Scholar]
- 13.Kjørmo O., Halvari H. Two ways related to performance in elite sport: the path of self-confidence and competitive anxiety and the path of group cohesion and group goal-clarity. Percept Mot Skills. 2002;94(3 PART 1):950–966. doi: 10.2466/pms.2002.94.3.950. [DOI] [PubMed] [Google Scholar]
- 14.Norton P.J., Burns J.A., Hope D.A., Bauer B.K. Generalization of social anxiety to sporting and athletic situations: gender, sports involvement, and parental pressure. Depress Anxiety. 2000;12(4):193–202. doi: 10.1002/1520-6394(2000)12:4<193::AID-DA2>3.0.CO;2-X. [DOI] [PubMed] [Google Scholar]
- 15.Peterson K.B. The effects of spinal manipulation on the intensity of emotional arousal in phobic subjects exposed to a threat stimulus: a randomized, controlled, double-blind clinical trial. J Manipulative Physiol Ther. 1997;20(9):602–606. [PubMed] [Google Scholar]
- 16.Jensen A.M., Ramasamy A. Treating spider phobia using Neuro Emotional Technique (NET): findings from a pilot study. J Altern Complement Med. 2009;15(12):1363–1374. doi: 10.1089/acm.2008.0595. [DOI] [PubMed] [Google Scholar]
- 17.Crawford J.R., Henry J.D. The Depression Anxiety Stress Scales (DASS): normative data and latent structure in a large non-clinical sample. Br J Clin Psychol. 2003;42(2):111–131. doi: 10.1348/014466503321903544. [DOI] [PubMed] [Google Scholar]
- 18.Mangione C.M., Goldman L., Orav E.J., Marcantonio E.R., Pedan A., Ludwig L.E. Health-related quality of life after elective surgery: measurement of longitudinal changes. J Gen Intern Med. 1997;12(11):686–697. doi: 10.1046/j.1525-1497.1997.07142.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Burke J.D., Burke K.C., Baker J.H., Hillis A. Test-retest reliability in psychiatric patients of the SF-36 Health Survey. Int J Methods Psychiatr Res. 1996;5(3):189–194. [Google Scholar]
- 20.Jenkinson C., Wright L., Coulter A. Criterion validity and reliability of the SF-36 in a population sample. Qual Life Res. 1994;3(1):7–12. doi: 10.1007/BF00647843. [DOI] [PubMed] [Google Scholar]
- 21.Ware J.E., Snow K.S., Kosinski M., Gandek B. The Health Institute, New England Medical Center; Boston: 1993. SF-36 Health Survey manual and interpretation guide. [Google Scholar]
- 22.Taft C., Karlsson J., Sullivan M. Do SF-36 summary component scores accurately summarize subscale scores? Qual Life Res. 2001;10(5):395–404. doi: 10.1023/a:1012552211996. [DOI] [PubMed] [Google Scholar]
- 23.Varma G.R., Kusuma Y.S., Babu B.V. Health-related quality of life of elderly living in the rural community and homes for the elderly in a district of India—application of the Short Form 36 (SF-36) Health Survey questionnaire. Z Gerontol Geriatr. 2009:1–5. doi: 10.1007/s00391-009-0077-x. [DOI] [PubMed] [Google Scholar]
- 24.Hagell P., Törnqvist A.L., Hobart J. Testing the SF-36 in Parkinson's disease: implications for reporting rating scale data. J Neurol. 2008;255(2):246–254. doi: 10.1007/s00415-008-0708-y. [DOI] [PubMed] [Google Scholar]
- 25.Brazier J.E., Harper R., Jones N.M.B., O'Cathain A., Thomas K.J., Usherwood T. Validating the SF-36 Health Survey questionnaire: new outcome measure for primary care. Br Med J. 1992;305(6846):160–164. doi: 10.1136/bmj.305.6846.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Guyton A.C., Hall J.E. 6th ed. W.B. Saunders Co.; London: 1997. Human physiology and mechanisms of disease. [Google Scholar]
- 27.Shirotsuki K., Izawa S., Sugaya N., Yamada K.C., Ogawa N., Ouchi Y. Salivary cortisol and DHEA reactivity to psychosocial stress in socially anxious males. Int J Psychophysiol. 2009;72(2):198–203. doi: 10.1016/j.ijpsycho.2008.12.010. [DOI] [PubMed] [Google Scholar]
- 28.ARL Functional Pathology . ARL Pathology; Melbourne: 2004. Adrenal hormone profile: interpretive guide. [Google Scholar]
- 29.Roberts A.D.L., Wessely S., Chalder T., Papadopoulos A., Cleare A.J. Salivary cortisol response to awakening in chronic fatigue syndrome. Br J Psychiatry. 2004;184:136–141. doi: 10.1192/bjp.184.2.136. [DOI] [PubMed] [Google Scholar]
- 30.Diamond D.M., Fleshner M., Rose G.M. The enhancement of hippocampal primed burst potentiation by dehydroepiandrosterone sulfate (DHEAS) is blocked by psychological stress. Stress. 1999;3(2):107–121. doi: 10.3109/10253899909001116. [DOI] [PubMed] [Google Scholar]
- 31.Hu Y., Cardounel A., Gursoy E., Anderson P., Kalimi M. Anti-stress effects of dehydroepiandrosterone: protection of rats against repeated immobilization stress-induced weight loss, glucocorticoid receptor production, and lipid peroxidation. Biochem Pharmacol. 2000;59(7):753–762. doi: 10.1016/s0006-2952(99)00385-8. [DOI] [PubMed] [Google Scholar]
- 32.Wang J.S., Chen S.M., Lee S.P., Lee S.D., Huang C.Y., Hsieh C.C. Dehydroepiandrosterone sulfate linked to physiologic response against hot spring immersion. Steroids. 2009;74(12):945–949. doi: 10.1016/j.steroids.2009.06.011. [DOI] [PubMed] [Google Scholar]
- 33.Walker S. Neuro Emotional Technique, Inc; Encinitas, CA: 2004. Neuro Emotional Technique certification manual. [Google Scholar]
- 34.Monti D.A., Stoner M.E., Zivin G., Schlesinger M. Short term correlates of the Neuro Emotional Technique for cancer-related traumatic stress symptoms: a pilot case series. J Cancer Surv. 2007;1(2):161–166. doi: 10.1007/s11764-007-0018-x. [DOI] [PubMed] [Google Scholar]
- 35.Monti D.A., Sinnott J., Marchese M., Kunkel E.J.S., Greeson J.M. Muscle test comparisons of congruent and incongruent self-referential statements. Percept Mot Skills. 1999;88(3):1019–1028. doi: 10.2466/pms.1999.88.3.1019. [DOI] [PubMed] [Google Scholar]
- 36.Peterson K.B. A preliminary inquiry into manual muscle testing response in phobic and control subjects exposed to threatening stimuli. J Manipulative Physiol Ther. 1996;19(5):310–317. [PubMed] [Google Scholar]
- 37.Cross J.R. Elsevier Health Sciences; London: 2001. Acupressure and reflextherapy in the treatment of medical conditions. [Google Scholar]
- 38.Huntley A., White A.R., Ernst E. Relaxation therapies for asthma: a systematic review. Thorax. 2002;57(2):127–131. doi: 10.1136/thorax.57.2.127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Becker W.J., Sauro K.M. Recent studies on stress management-related treatments for migraine. Headache. 2009;49(9):1387–1390. doi: 10.1111/j.1526-4610.2009.01476.x. [DOI] [PubMed] [Google Scholar]
- 40.Kolt G.S., Hume P.A., Smith P., Williams M.M. Effects of a stress-management program on injury and stress of competitive gymnasts. Percept Mot Skills. 2004;99(1):195–207. doi: 10.2466/pms.99.1.195-207. [DOI] [PubMed] [Google Scholar]
- 41.Hefner J., Rilk A., Herbert B.M., Zipfel S., Enck P., Martens U. [Hypnotherapy for irritable bowel syndrome—a systematic review] Z Gastroenterol. 2009;47(11):1153–1159. doi: 10.1055/s-0028-1109697. [DOI] [PubMed] [Google Scholar]
- 42.Saini M. A meta-analysis of the psychological treatment of anger: developing guidelines for evidence-based practice. J Am Acad Psychiatry Law. 2009;37(4):473–488. [PubMed] [Google Scholar]
- 43.Kvien T.K., Heiberg T., Hagen K.B. Minimal clinically important improvement/difference (MCII/MCID) and patient acceptable symptom state (PASS): what do these concepts mean? Ann Rheum Dis. 2007;66(Suppl 3):iii40–iii41. doi: 10.1136/ard.2007.079798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hays R.D., Morales L.S. The RAND-36 measure of health-related quality of life. Ann Med. 2001;33(5):350–357. doi: 10.3109/07853890109002089. [DOI] [PubMed] [Google Scholar]
- 45.Ahu R.S., Lee Y.J., Choi J.Y., Kwon H.B., Chun S.I. Salivary cortisol and DHEA levels in the Korean population: age-related differences, diurnal rhythm, and correlations with serum levels. Yonsei Med J. 2007;48(3):379–388. doi: 10.3349/ymj.2007.48.3.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hansen Ã.M., Garde A.H., Persson R. Sources of biological and methodological variation in salivary cortisol and their impact on measurement among healthy adults: a review. Scand J Clin Lab Invest. 2008;68(6):448–458. doi: 10.1080/00365510701819127. [DOI] [PubMed] [Google Scholar]
- 47.Perry B.D., Pollard R.A., Blakely T.L., Baker W.L., Vigilant D. Childhood trauma, the neurobiology of adaptation and ‘use-dependent’ development of the brain: how ‘states’ become ‘traits.’. Infant Ment Health J. 1995;16(4):271–291. [Google Scholar]
- 48.Perry B.D. The neurodevelopmental impact of violence in childhood. In: Schetky D., Benedek E.P., editors. Textbook of child and adolescent forensic psychiatry. American Psychiatric Press; Washington, D.C.: 2001. pp. 221–238. [Google Scholar]
- 49.LeDoux J. Touchstone; New York: 1996. The emotional brain: the mysterious underpinnings of emotional life. [Google Scholar]
- 50.Kathol R.G., Wenzel R.P. Natural history of symptoms of depression and anxiety during inpatient treatment on general medicine wards. J Gen Intern Med. 1992;7(3):287–293. doi: 10.1007/BF02598085. [DOI] [PubMed] [Google Scholar]
- 51.Green B.N., Johnson C.D. How to write a case report for publication. J Chiropr Med. 2006;5(2):72–82. doi: 10.1016/S0899-3467(07)60137-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
. SF-36 scores (all subscales, raw scores)