

Abstract
Objective
The present study evaluated the efficacy of the Middle School Success intervention (MSS) for reducing substance use and delinquency among girls in foster care, using a randomized controlled trial (RCT) design. The program was designed to fill a service gap during the summer prior to the middle school transition and to prevent delinquency, substance use, and related problems.
Method
One hundred girls in foster care and their caregivers were randomly assigned either to the intervention (n = 48) or to a regular foster care control (n = 52) condition. The girls completed a baseline (T1) assessment and follow-up assessments at 6 months (T2), 12 months (T3), 24 months (T4), and 36 months (T5) postbaseline. Caregivers participated in assessments from T1 through T4. This study is a follow up to Smith et al. (2011)’s study, which examined immediate outcomes at T2.
Results
Girls in the intervention condition showed significantly lower levels of substance use than did girls in the control condition at 36-months postbaseline. The group difference was only marginally significant for delinquency. Further analyses indicated significant indirect effects of the intervention through increased prosocial behaviors which led to decreased internalizing and externalizing symptoms and then to lower levels of substance use. The direct effect of the intervention on substance use remained significant in the presence of the indirect effects. For delinquency, the intervention had positive effects mainly through increased prosocial skills.
Conclusions
Findings highlight the importance of providing preventive intervention services for early adolescent girls in foster care.
Keywords: foster care, girls, drug use, delinquency, adolescent, intervention
Adolescent girls in foster care are at high risk for a wide range of poor outcomes including drug use, delinquent behavior, poor school adjustment, and health risking sexual behavior (e.g., Courtney et al., 2005; Courtney & Dworsky, 2006; Jonson-Reid & Barth, 2000; Leve & Chamberlain, 2007; Pecora et al., 2003). For instance, Cusick and Courtney (2007) found that girls in foster care reported significantly higher rates of arrest by age 19 as compared to girls in the National Longitudinal Study of Adolescent Health (Add Health) (34.4% vs. 2.8%). Although girls in foster care commit lower levels of offenses than their counterpart boys, many girls in foster care are at increased risk of having multiple pregnancies/live births and maltreating their own children (Dworsky & DeCoursey, 2009). This suggests that girls in foster care may be at high risk for engaging in problem behaviors that are likely to have negative cascading effects and lead to continued involvement in public services sectors as young adults (Courtney et al., 2005; Leve, Chamberlain, & Reid, 2005). Therefore, effective approaches to prevent girls in foster care from initiating problem behaviors are of great significance from a public health perspective.
While a few promising intervention programs for girls at-risk for delinquent behaviors have been reported (Hipwell & Loeber, 2006), evidence-based preventive intervention programs that specifically target girls in foster care during early adolescence are rare. This may be because pathways to problem behaviors, especially substance use and delinquent behavior, are not well understood for early adolescent girls (Chamberlain, 2003). However, given that girls in foster care tend to have experienced more physical and sexual abuse and subsequently suffered more from emotional problems than boys in foster care (Burns et al., 2004; Leve & Chamberlain, 2005), they are likely to be susceptible to negative trajectories of problem behaviors across adolescence and adulthood without any prevention or intervention efforts (Pecora, 2010). Furthermore, findings on the early onset of risky behaviors for youth in foster care suggest that prevention efforts should target preadolescents before they initiate problem behaviors (MacMillan et al., 2009). In the present study, we evaluated the efficacy of the Middle School Success intervention (MSS), a program aimed at promoting healthy adjustment in adolescent girls in foster care during the transition to middle school (Chamberlain, Leve, & Smith, 2006). The curriculum was designed to prevent problems with delinquency, substance use, and related problems. Prior work has shown that girls in the MSS intervention condition had significantly lower rates of internalizing and externalizing behaviors than did girls in the control condition at 6-months postbaseline (Smith, Leve, & Chamberlain, in press). The present study extended this previous work and focused on effects of the MSS intervention on substance use and delinquency at 36-months postbaseline.
Substance Use and Delinquent Behavior Among Foster Girls
According to the National Survey on Drug Use and Health, youths (aged 12 to 17) who have been in foster care report higher rates of illicit drug use (33.6 % vs. 21.7%) and a higher need for substance abuse treatment (17.4% vs. 8.8%) than youth who have never been in foster care (Substance Abuse and Mental Health Services Administration [SAMHSA], 2005). Additionally, early onset of substance use, a strong predictor for later substance abuse problems, is especially prevalent among youth in foster care (Jonson-Reid, Scott, McMillen, & Edmond, 2007; Thompson & Auslander, 2007). A survey of youth between the ages of 12 and 17 who were living with foster families in the State of Washington in 1998-1999 found that the mean age of first alcohol consumption and marijuana use was as early as 11.5 years and 12.2 years, respectively (Kohlenberg, Nordlund, Lowin, & Treichler, 2002). Furthermore, limited evidence has suggested that girls in foster care report similarly high levels of substance use as their counterpart boys (e.g., Taussig, Clyman, & Landsverk, 2001; Thompson & Auslander, 2007).
Girls in foster care are also at increased risk for serious delinquency and involvement in the juvenile justice system (Chamberlain, Leve, & DeGarmo, 2007). Based on juvenile delinquency petition data, Ryan and Testa (2005) found that, of the 10- to 16-year-olds in the Illinois child welfare system between 1995 and 2000, over 50% had at least one report of delinquency, a 47% greater likelihood than their non–foster care peers. Studies using diagnostic interviews (e.g., the Casey Field Office Mental Health Study) have also indicated that youth in foster care tend to show high lifetime prevalence rates for disruptive disorders such as conduct disorder and oppositional defiant disorder, ranging from 21% to 48% (White, O’Brien, White, Pecora, & Phillips, 2007).
Substance use and delinquent behaviors have often been identified as significant predictive factors of other cascading health risking behaviors and negative outcomes such as early initiation of sexual intercourse, STI-/HIV risk behaviors (e.g., having multiple partners, having sex while intoxicated), early pregnancy, and dating violence for youth in foster care (e.g., Keller, Salazar, & Courtney, 2010; Pecora, 2010). However, the literature has typically focused on late adolescence, and little is known about the risks during early adolescence. Given that substance use and other co-occurring problem behaviors tend to increase substantially during middle-school years (Lochman & Wells, 2002), preventive interventions for preadolescent girls aimed at reducing risk for a set of problems are urgently needed.
Processes Targeted by the MSS Intervention Program
Emanating from developmental theories and intervention work with at-risk youth (e.g., Eddy & Chamberlain, 2000; Price et al., 2008), the MSS program included two components (one for the girls and another for their caregivers) with an emphasis on two mediating processes (increasing girls’ prosocial skills and placement stability) and one immediate outcome (decreasing girls’ internalizing/externalizing symptoms during early adolescence, which is often a precursor to more severe forms of problem behaviors in late adolescence and young adulthood). A detailed description of the MSS program is provided below.
One of the immediate goals of the MSS curriculum was to build girls’ prosocial skills and increase self-efficacy. It has been hypothesized that children in foster care who experience child abuse and neglect and multiple caregiver transitions show deficiencies in the development of prosocial skills (Cicchetti, 1990; Koenig, Cicchetti, & Rogosch, 2004). Evidence has shown that poor prosocial behavior is significantly related to increased externalizing behaviors, conduct disorder, deviant peer relations, and maladaptive emotional well-being (e.g., Cicchetti, 1990; Pursell, Laursen, Rubin, Booth-LaForce, & Rose-Krasnor, 2008). Another line of research has indicated that early adolescence may provide an important opportunity for the development of prosocial skills because the middle-school years are when children face physical and social changes and must adapt to new interpersonal relationships with peers, parental figures, and teachers (Carlo, Fabes, Laible, & Kupanoff, 1999). These findings indicate that prosocial skills may serve as a pathway to more positive adjustment (Cicchetti, 1990) and that preventive efforts to promote prosocial skills during early adolescence may be particularly beneficial for girls in foster care.
In tandem with the goal of increasing girls’ prosocial skills, an immediate goal of the caregiver curriculum was to increase placement stability by improving parenting skills. Using administrative child welfare data linked to Medicaid Claims in the state of Washington from 1998 to 1999 (N = 903), DiGiuseppe and Christakis (2003) found that children stay in the foster care system for approximately 2 years on average, with half experiencing at least one placement change and 20% reporting at least three placement changes in less than a year. Evidence has suggested that such multiple placement changes are associated with adjustment difficulties among children in foster care (Barth, Weigensberg, Fisher, Fetrow, & Green, 2008; Fisher, Kim, & Pears, 2009). Rubin and colleagues (2004) found that children in foster care who experienced multiple placement changes, compared to those who did not experience such instability, had up to 63% higher risk for behavior problems. Thus, increasing placement stability may help ameliorate some of the negative consequences of early adversity and alter negative trajectories among youth in foster care (Harden, 2004; Price et al., 2008).
Given the significant association of prosocial skills and placement stability with problem behaviors among youth in foster care, we hypothesized decreases in internalizing and externalizing symptoms as an immediate response to the MSS intervention. There is considerable evidence that externalizing symptoms during early adolescence lead to more severe forms of problem behaviors in late adolescence and young adulthood (e. g., Chassin, Pitts, DeLucia, & Todd, 1999). Studies have also indicated significant links between various internalizing symptoms (e.g., depression, anxiety) and later substance use among girls (e.g., Marmorstein et al., 2010). These findings highlight the etiological significance of internalizing and externalizing symptoms for later substance use and delinquency, although this developmental pathway has not yet been systematically examined among girls in foster care. Prior work with this sample has indicated that girls in the MSS intervention condition showed significantly lower rates of internalizing and externalizing behaviors than did those in the control condition during the fall of the first year of middle school (6-months postbaseline) (Smith et al., in press); longer term outcomes have not been previously examined. In the present study, we examined whether the intervention effects on internalizing and externalizing symptoms of the girls remained significant at 12- and 24-months postbaseline, as well as whether lowered internalizing and externalizing symptoms would serve as a pathway to prevent substance use and delinquent behaviors at 36-months postbaseline.
Significance of the Middle School Transition
A distinctive feature of the MSS intervention program is its timing during the transition to middle school, a critical period that has been associated with a range of subsequent adjustment problems (Moilanen, Shaw, & Maxwell, 2010), including significant declines in academic achievement, motivation, and self-esteem, and significant increases in discipline problems and psychological distress (e.g., Chung, Elias, & Schneider, 1998; Theriot & Dupper, 2010). A prominent aspect of the middle school transition is ‘discontinuities’ in social roles and context/environment; middle schools are often larger, impersonal, and more achievement-oriented than elementary schools and require different teacher-student and peer relationships (Chung et al., 1998; Moilanen et al., 2010). Given that girls in foster care have typically experienced a great deal of adversity earlier in development, the middle school transition may represent a particularly challenging period. Drawing upon these findings, as well as the argument that an optimal time for children to learn about problem behaviors, competence, and resilience is when they face challenges and developmental transitions (Luthar & Cicchetti, 2000), the MSS program was delivered during the summer prior to the middle school entry to support girls in foster care during a particularly vulnerable stage in development.
The Present Study
The present study evaluated the efficacy of the MSS program using a randomized controlled trial (RCT) design in a sample of girls in foster care who were recruited during their last year of elementary school. First, we examined mean differences in substance use and delinquency between the MSS intervention condition and the control condition at 36-months postbaseline. We hypothesized that girls randomly assigned to the MSS condition would show lower levels of substance use and delinquent behaviors compared to girls in the control condition. Second, we examined potential pathways through which the MSS intervention influenced girls’ substance use and delinquency. Given the intervention’s focus on the girls’ prosocial skills and placement stability, we hypothesized that the MSS would have direct and positive effects on the girls’ prosocial skills and placement stability, which would in turn lead to lower levels of internalizing/externalizing symptoms and to lower levels of substance use and delinquent behavior. We also hypothesized that the direct effects of the intervention on substance use and delinquent behavior would persist even in the context of the indirect effects of prosocial skills and placement stability because of the direct emphasis of the intervention on the prevention of the two primary outcomes.
Method
Sample
Eligible participants were girls in (a) relative or nonrelative foster care in one of two counties containing major metropolitan areas in the Pacific Northwest and (b) in their final year of elementary school. A total of 145 girls were referred to the study by child welfare staff members, who ran a search of their database to gather information on all girls who were 10-12 years old, in their final year of elementary school, currently in foster care, and living in the targeted county. All 145 girls who met the above criteria were invited to participate in the study. Recruitment consisted of the research team contacting the child’s case worker to discuss the study and invite participation. If the caseworker agreed to the girls’ participation, the girl and her foster parent were then contacted and invited to participate. Of the 145 eligible girls, 27 refused to participate (either the girl, her caregiver, or her caseworker did not agree to the girls’ participation), and an additional 18 girls were excluded because their eligibility status changed by the time they were contacted by study personnel for recruitment (e.g., moved out of the state, were pending reunification or adoption, or were in an incorrect grade level). The resulting sample included 100 girls and their caregivers. Girls were randomly assigned (via a coin flip) to the intervention condition (n = 48) or to a regular foster care control condition (n = 52; Chamberlain et al., 2006). The flow of participants through the study is presented in Figure 1. Caseworkers and the foster caregivers provided informed consent, and the girls provided assent prior to participation. The girls and their caregivers were compensated for participating. All procedures were approved by our institution’s Institutional Review Board.
Figure 1.
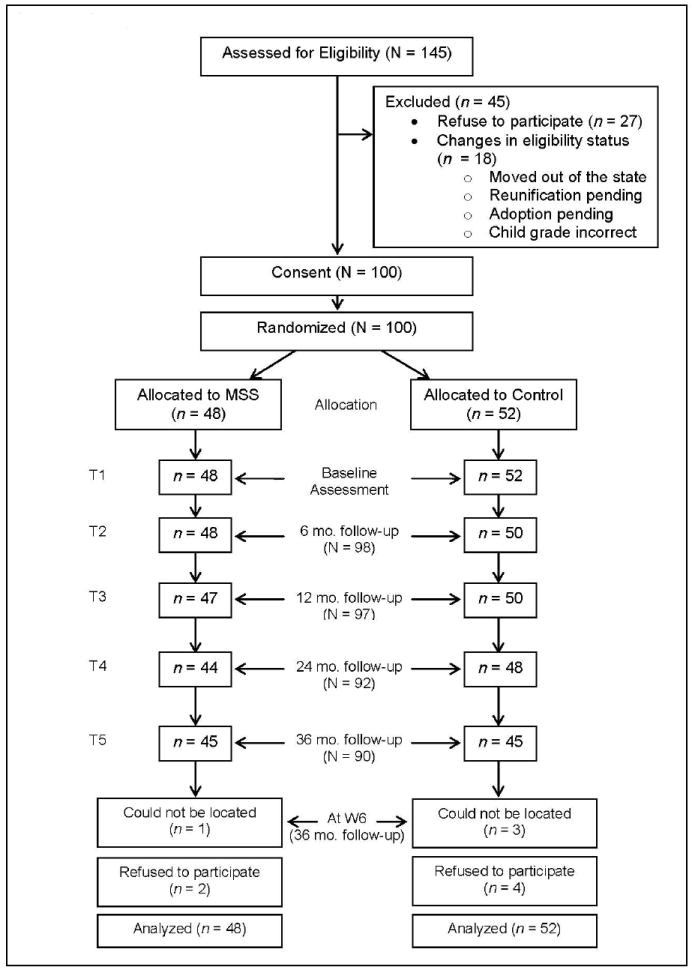
Consort Chart
The mean age of the girls was 11.54 years (SD = 0.48) at the first assessment (baseline). The ethnicity breakdown of the sample was 63% European American, 9% African American, 10% Latino, 4% Native American, and 14% multiracial. The girls were, on average, 7.63 years old (SD = 3.14) when first placed in foster care and had spent approximately 2.90 years (SD = 2.25) in foster care prior to the study. Overall, 56% and 67% of the girls had at least one reported incident of physical and sexual abuse, respectively, 97% had at least one reported incident of neglect, and 32% of the girls experienced all three types of maltreatment. Most girls had experienced more than one placement change (ranged from 1 to 20) since first placement (M = 4.29, SD = 3.32). Sixty-eight percent of the girls were in nonrelative foster homes and 32% were in relative foster homes at baseline.1 At the start of the study, there were no differences between the intervention and control condition on any of the demographic characteristics (e.g., ethnicity, caregiver’s income), severity levels for physical and sexual abuse, and foster care characteristics (number of placement changes and type of care). In addition, both groups had very similar levels of internalizing and externalizing behavior at baseline. The only group difference was found for the level of the mean severity in neglect. Girls in the intervention group had slightly higher levels of severity in neglect than those in the control condition (t(95) = -2.60, p < .05). However, the mean severity of neglect was not related to any of the outcome measures in the study and when included in the subsequent models, it was not significant. Thus, the final models did not include neglect in the interest of parsimony. Baseline characteristics by group are presented in Table 1.
Table 1.
Baseline characteristics of the sample by group (N = 100)
| Control Condition (n = 52) | MSS Condition (n = 48) | |
|---|---|---|
| Age | 11.59 (.45) | 11.48 (.51) |
| Ethnicity | ||
| Caucasian | 61.5% | 64.6% |
| African American | 15.4% | 2.1% |
| Hispanic/Latino | 7.7% | 12.5% |
| Multi-racial | 13.5% | 14.6% |
| American Indian/Alaska Native | 1.9% | 6.3% |
| Caregiver family income | ||
| $24,999 or below | 22.7% | 17.8% |
| $25,000 – 59,999 | 47.8% | 51.1% |
| $60,000 or more | 29.5% | 31.1% |
| Severity of Maltreatment experience | ||
| Physical | 1.98 (.85) | 2.07 (.91) |
| Sexual | 2.50 (.98) | 2.61 (.88) |
| Neglect1 | 2.41 (.47) | 2.70 (.66) |
| Age at 1st placement (years) | 7.96 (2.81) | 7.32 (3.44) |
| Number of placement changes (pre-baseline) | 4.33 (3.11) | 4.25 (3.55) |
| Foster care type | ||
| Relative foster parent | 36.5% | 31.3% |
| Non-relative foster parent | 63.5% | 68.8% |
| History of delinquency | ||
| Arrest records | 3.8% | 2.1% |
| Runaway | 7.7% | 4.2% |
| History of special services | 36.6% | 46.2% |
| Psychosocial adjustment 2 | ||
| Internalizing behavior | 11.56 (9.42) | 11.96 (8.19) |
| Externalizing behavior | 14.38 (11.65) | 16.06 (11.05) |
Note. Values in the parentheses indicate standard deviations.
The group difference was significant for neglect (t = -2.60 (df = 95), p = .01), which was the only difference between the intervention and control condition.
Raw scores from caregiver reports on the Achenbach System of Empirically Based Assessment were used (ASEBA; Achenbach & Rescorla, 2001).
Procedure
Girls and their caregivers participated in a baseline (T1) assessment prior to the intervention and completed follow-up assessments at 6 months (T2), 12 months (T3), 24 months (T4), and 36 months (T5) postbaseline (only the girls participated in the T5 assessment). Retention rates were at or above 90% during the study period (Figure 1). The assessment included a structured interview and questionnaires for each girl and her caregiver, an interview with the girl’s caseworker, and the collection of child welfare records. Assessments lasted 2 hr and were conducted by trained assessors who were blind to the participants’ group assignment. All group-based intervention sessions were videotaped for purposes of training and monitoring model fidelity.
MSS Intervention
Overview
The MSS intervention was delivered during the summer prior to middle school entry with the goal of preventing delinquency, substance use, and related problems for girls in foster care (Chamberlain et al., 2006). The intervention consisted of two primary components: (a) six sessions of group-based caregiver management training for the foster parents and (b) six sessions of group-based skill-building sessions for the girls. The groups met twice a week for 3 weeks, with approximately seven participants in each group. The caregiver sessions were led by one facilitator and one co-facilitator. The girl sessions were led by one facilitator and three assistants to allow a high staff-to-girl ratio (1:2) for individualized attention, one-on-one modeling/practicing of new skills, and frequent reinforcement of positive behaviors. In addition to the summer group sessions, follow-up intervention services (i.e., ongoing training and support) were provided to the caregivers and girls in the intervention group once a week for two hr (foster parent meeting; one-on-one session for girls) during the first year of middle school. The interventionists were supervised weekly, where videotaped sessions were reviewed and feedback was provided to maintain the fidelity of the clinical model (Chamberlain et al., 2006; Smith et al., in press).
Intervention structure and curriculum for caregivers
The summer group sessions for the caregivers emphasized establishing and maintaining stability in the foster home, preparing girls for the start of middle school, and preventing early adjustment problems during the transition to middle school. The caregivers’ curriculum focused on developing a behavioral reinforcement system to encourage adaptive behaviors across home, school, and community settings. Guided by prior studies of youth in foster care (Chamberlain, 2003), the group facilitators used data from the Parent Daily Report Checklist (PDR, Chamberlain & Reid, 1987), a 10-min phone interview with caregivers about behavioral and emotional issues and the types of discipline and supervision used during the past 24 hr to connect the planned curriculum to the daily challenges the foster parents were facing. Facilitators used items on the PDR to review specific problem behaviors that occurred during the day, which were then used as the week’s examples of the curriculum. Weekly home practice assignments were provided to encourage foster parents to apply new skills. On average, participants completed 5.62 of the 6 summer sessions (SD = .99). When a participant missed a session, the interventionist either went to the families’ home to deliver the content in person or delivered the content via a telephone call. The caregivers also participated in the weekly follow-up sessions as a group during the following school year. Of the 40 sessions offered, caregivers attended 20 weekly follow-up sessions on average (SD = 10.4).
Intervention structure and curriculum for girls
The summer group sessions were designed to prepare the girls for the middle school transition by increasing their social skills for establishing and maintaining positive relationships with peers, increasing their self-confidence, and decreasing their receptivity to initiation from deviant peers. Specifically, the girls’ curriculum targeted strengthening prosocial skills; practicing sharing/cooperating with peers; increasing the accuracy of perceptions about peer norms for abstinence from substance use, sexual activity, and violence; and practicing strategies for meeting new people, dealing with feelings of exclusion, and talking to friends and teachers about life in foster care. Each session was highly structured with specific content and instructions for each activity. The group structure typically included an introduction to the session topic, role plays, and a game or activity during which girls practiced the new skill. In addition, the girls engaged in overt discussions about self-image and the personal characteristics and behaviors (e.g., being a good friend, getting good grades, and abstaining from substance use) they wished to project as they entered middle school. During the final summer session, each girl proclaimed and solidified her goals and commitments in a small ceremony. The ceremony included members of the girl’s session group and their foster parents and was designed to help the girls build confidence in who they are and who they want to become, and to build supportive ties between the girls and their foster parents by “publicizing” their goals and commitments. Participation rates mirrored those of their caregivers (Chamberlain et al., 2006; Smith et al., in press).
In addition to the group-based summer sessions, the girls in the intervention condition participated in weekly individual coaching sessions during the 1st year of middle school. The goal of these individual sessions was to provide ongoing social support and training. These individual coaching sessions continued to focus on establishing and maintaining positive peer relations, increasing knowledge of accurate norms for problem behaviors, and increasing self-competence in academic and social areas. Coaches also emphasized the risks of substance use and discussed issues around dating and partner relations. The coaches were recent female college graduates who were trained and supervised to serve as role models of prosocial behaviors and confidants to discuss issues around family and peer relations (Chamberlain et al., 2006). Approximately 40 sessions were offered and the average attendance rate was 56.4% (SD = 28.5%).
Control Condition
The girls and caregivers in the control condition received the usual services provided by the child welfare system, including services such as referrals to individual or family therapy, parenting classes for biological parents, and case monitoring. Sixty two percent of girls in the control condition received individual counseling, 20% received family counseling, 22% received group counseling, 30% received mentoring, 37% received psychiatric support, and 40% received other counseling or therapy services (e.g., school counseling, academic support) during the 1st year of middle school. Note that many girls received more than one service, and therefore the percentages listed above exceed 100%. Child welfare caseworkers managed each case and were responsible for making all decisions on referrals to community resources, including individual and family therapy and parenting classes (Smith et al., in press).
Measures
Outcomes
Substance use
Three indicators were used to assess the girls’ substance use at T5: tobacco use, alcohol use, and marijuana use. The girls were asked how many times in the past year they had (a) smoked cigarettes or chewed tobacco, (b) drank alcohol (beer, wine, or hard liquor), and (c) used marijuana. The response scale ranged from 1 (never) through 9 (daily). Twenty-three percent of the girls reported either smoking or chewing tobacco, 33% reported using alcohol, and 24% reported using marijuana in the past year.
Delinquency
Delinquency at T5 was assessed using two indicators: girls’ own delinquent behavior and girls’ association with delinquent peers. Girls’ own delinquent behavior was measured using the 36 items from the general delinquency scale from the Self-Report Delinquency Scale (SRD; Elliott, Huizinga, & Ageton, 1985). Girls were asked to rate how many times they had committed various delinquent acts in the past year, using an open-ended format. The sample items included ‘purposely damaged or destroyed properties that did not belong to them’ and ‘stole or tried to steal something worth more than $50’. The scale showed good internal reliability (Chronbach alpha = .85). The mean of frequencies across these items was used to represent the level of delinquency for girls. The sample mean was .62 (SD = 2.03), suggesting girls in the present sample committed approximately 22 delinquent acts in the past 12 months. The girls’ association with delinquent peers was measured using 30 items from a modified version of the general delinquency scale from the SRD Scale (Elliott et al., 1985). Girls were asked to rate how many of their friends were involved in delinquent acts and how often their friends used (a) alcohol, (b) tobacco, (c) marijuana, and (d) drugs in the past year. Sample items include, ‘hit or threaten to hit other kids’, and ‘purposely set fire (or tried to) to a house, building, car or other property’. The original response scale for the first 26 items ranged from none (1) to all (5) which were then recoded to 0 (none) to 4 (all) to facilitate the interpretability. The response scale for the last 4 items on the substance use ranged from none (0) to a lot (4). Because the first 26 items and the last 4 items were on different response scales, they were standardized before combined to compute a mean value. The internal reliability of the scale was .96.
Predictors
Girls’ placement changes (cumulative changes from T1 through T3), prosocial behavior (T2 and T3), and internalizing and externalizing symptoms (T3 and T4) were included as predictors and were taken from assessment time points prior to T5 (when the primary outcome measures for substance use and delinquent behavior were assessed). The temporal order of the variables was selected so that all predictors were assessed prior to T5 in order to facilitate the examination of a causal mechanism through which the intervention might influence girls’ substance use and delinquency at 36-months postbaseline.
Placement changes
Child welfare system records were collected at each assessment to determine the girls’ placement changes (including the number and type of changes). Placement changes since the start of the study through T3 were summed for each girl. The number of placement changes ranged from 0 to 7 during this period (M = .56, SD = 1.14).
Prosocial behavior
Prosocial behavior was measured using a subscale from the Parent Daily Report Checklist (PDR; Chamberlain & Reid, 1987). The PDR was administered individually by telephone to foster parents on 3 consecutive or closely spaced days (1–3 days apart) at each assessment for both conditions. Note that PDR calls that were conducted as part of the MSS intervention were only for the intervention condition and were not included in the analysis. A trained interviewer asked the foster parent whether a list of prosocial behaviors took place during the previous 24 hr (yes/no format). The PDR was designed to avoid the potential bias of aggregate recall of frequency estimates. Studies have reported concurrent and predictive validity of the PDR checklist (Chamberlain et al., 2006; Chamberlain et al., 2008; McClowry, Snow, & Tamis-LeMonda, 2005). The prosocial scale was computed based on 9 items, such as ‘clean up after herself’ and ‘do a favor for someone’. The items are primarily focused on the girls’ behavior in the home setting. However, if the caregiver was aware of activities with peers and school, many of the items could also reflect school/peer behavior. The scores were averaged across calls from three days. Internal reliabilities ranged from .61 at T2 and .74 at T3. Prosocial behavior at T2 and T3 were significantly correlated at .48 (p < .001) and thus the mean of both time points was used in the subsequent analysis.
Internalizing and externalizing symptoms
Internalizing and externalizing symptoms at T3 and T4 were measured using caregiver report on the Achenbach System of Empirically Based Assessment (ASEBA; Achenbach & Rescorla, 2001). This widely used checklist for psychopathological behaviors includes scales for behaviors such as Anxious/Depressed; Withdrawn; Somatic Complaints; Thought Problems; Attention Problems; Aggressive Behavior; Rule-Breaking Behavior; and Intrusive. The ASEBA has been shown to have both construct and content validity in the literature. For the present study, raw scores for the internalizing and externalizing symptoms subscales were used. Scores at T3 and T4 were significantly correlated with one another (ranged from .52 to .76, all p < .001) and thus combined and averaged. The internal reliabilities ranged from .85 to .94.
Data analysis plan
Structural Equation Modeling (SEM) was conducted for each outcome measure, using Mplus 6 (Muthén & Muthén, 1998-2010). In order to include the full intent-to-treat randomized sample (N = 100), full information maximum likelihood (FIML) estimation was used, which has been shown to provide unbiased estimates when data are missing at random (Arbuckle, 1996). Missing data in the present sample was minimal due to the high retention rates. Further, the results of the Little’s MCAR test indicated the data were missing completely at random in the present sample (χ2= 20.88, df = 12, p > .05); thus, it is safe to use the FIML estimation. Variables were examined for nonnormal distributions and outliers; three indicators for substance use, two indicators for delinquency, prosocial behavior, and internalizing/externalizing symptoms exhibited significant skewness and thus were transformed to more closely resemble a normal distribution. A log transformation was used for the substance and delinquency indicators and a square root transformation was used for prosocial behavior and internalizing/externalizing symptoms. The significance of indirect effects was tested using Mplus.
Results
Descriptives
Means and standard deviations of the study variables by condition are presented in Table 2. Bivariate correlational analyses indicated that being in the intervention condition was negatively correlated with the number of placement changes and positively correlated with the girls’ prosocial behavior at T2 and T3. While the intervention condition was also significantly and negatively correlated with the girls’ tobacco and marijuana use, it was not significantly associated with the girls’ alcohol use, their own delinquent behavior, or their association with delinquent peers at T5. The number of placement changes was significantly related to higher marijuana use and girls’ own delinquent behavior. Girls’ prosocial behavior at T2 and T3 was significantly and negatively related to their internalizing/externalizing symptoms at T3 and T4, and to tobacco use, delinquent behavior, and association with delinquent peers at T5. Higher internalizing/externalizing symptoms were significantly related to increased tobacco and marijuana use. All of the indicators of substance use and delinquency were correlated with each of the other variables (Table 2).
Table 2.
Means, standard deviations, bivariate correlations among study variables (N = 100)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Intervention condition (0 = control;1 = intervention) | |||||||||||
| 2. Placement changes (T2 & T3) | -.24* | ||||||||||
| 3. Prosocial behavior (T2 & T3) | .22* | -.12 | |||||||||
| 4. Inter/externalizing behavior (T3 & T4) | .01 | .12 | -.37*** | ||||||||
| 5. Tobacco use (T5) | -.22* | .14 | -.28** | .28** | |||||||
| 6. Alcohol use (T5) | -.12 | .14 | -.07 | .15 | .70*** | ||||||
| 7. Marijuana use (T5) | -.28** | .26* | -.09 | .30** | .72*** | .72*** | |||||
| 8. Composite substance use (T5) | -.23* | .22* | -.16 | .30** | .91*** | .86*** | .91*** | ||||
| 9. Delinquent behavior (T5) | -.18+ | .22* | -.24* | .17 | .50*** | .58*** | .50*** | .57*** | |||
| 10. Association w/Delinquent Peers (T5) | -.17 | .20+ | -.24* | .15 | .59*** | .73*** | .62*** | .71*** | .59*** | ||
| 11. Composite delinquency (T5) | -.19+ | .22* | -.26* | .16 | .59*** | .72*** | .61*** | .70*** | .73*** | .97*** | |
| Control Group (n = 52) | |||||||||||
| M | .76 | .74 | 12.50 | 2.36 | 1.80 | 2.33 | 2.16 | .95 | .17 | .17 | |
| SD | 1.19 | .14 | 8.29 | 2.49 | 1.46 | 2.43 | 1.93 | 2.69 | 1.02 | 1.06 | |
| Intervention Group (n = 48) | |||||||||||
| M | .33 | .80 | 12.77 | 1.49 | 1.49 | 1.29 | 1.42 | .30 | -.17 | -.17 | |
| SD | 1.05 | .12 | 8.53 | 1.63 | .90 | .82 | .93 | .92 | .86 | .57 |
Note.
< .10,
< .05,
< .01,
< .001
Mean Differences in Substance Use and Delinquency at T5
The first purpose of the study was to examine mean differences in substance use and delinquency between the MSS intervention and the control condition. As shown in Tables 2 and 3, the means on the substance use outcome variables indicated that girls in the MSS condition reported significantly lower levels of substance use (Cohen’s d = .47 for the substance use composite score, which is a mean of three substance use indicators), compared to girls in the control condition. The group differences were of a greater magnitude for tobacco use and marijuana use than for alcohol use. The group difference was only marginally significant for the composite score of the girls’ delinquency (i.e., the mean of the two indicators: girls own’ delinquent behavior and her association with delinquent peers).
Table 3.
Independent group t test results for study variables
| Variables | t-test | Cohen’s d |
|---|---|---|
| Placement changes (T2 & T3) | t = 2.45 (df = 97), p = .02 | .50 |
| Prosocial behavior (T2 & T3) | t = -2.25 (df = 97), p = .03 | .46 |
| Internalizing/externalizing symptoms (T2 & T3) | t = -.10 (df = 95), ns | .02 |
| Tobacco use (T5) | t = 2.14 (df = 88), p =.04 | .45 |
| Alcohol use (T5) | t = 1.12 (df = 88), ns | .24 |
| Marijuana use (T5) | t = 2.69 (df = 88), p = .01 | .57 |
| Composite substance use (mean of tobacco, alcohol, and marijuana use at T5) | t = 2.23 (df = 88), p = .03 | .47 |
| Delinquent behavior (T5) | t = 1.67 (df = 88), p = .098 | .36 |
| Association with deviant peer (T5) | t = 1.66 (df = 88), ns | .35 |
| Composite delinquency (mean of delinquent behavior and association with deviant peer at T5) | t = 1.84 (df = 88), p = .07 | .39 |
Direct and Indirect Effects of the MSS Intervention on Substance Use
The second purpose of the study was to examine potential pathways through which the MSS intervention influenced foster girls’ outcomes. For substance use, the model fit the data relatively well (χ2 [15] =17.45, p = .29, CFI = .99, TLI = .98, RMSEA = .04). As shown in Figure 2, all three indicators of substance use significantly loaded on the latent factor and were significantly related to one another. Intervention condition was significantly related to the number of placement changes and the girls’ prosocial behavior during the first year of the study period (assessed at T2 and T3), suggesting that the intervention successfully stabilized the placement and increased the frequency of prosocial behavior. The girls’ prosocial behavior was then significantly and negatively related to her internalizing/externalizing symptoms at T3 and T4, which was subsequently related to higher substance use at T5. In addition, the path from the intervention condition to substance use was also significant, suggesting a significant direct intervention effect on reducing later substance use. The model accounted for 52% of the variance in the latent variable for substance use at T5 (p = .01). Furthermore, we conducted significance tests to examine whether these paths qualified as having significant mediating effects in Mplus. The results indicated that the path from prosocial behavior to internalizing/externalizing symptoms and then to girls’ substance use was the only significant indirect path in the model (β = -.17, p = .02), suggesting that girls’ internalizing/externalizing symptoms are significant mediators that link girls’ prosocial behavior and substance use. The total indirect effects (the combined effects of the two indirect paths, one for the path from intervention condition to prosocial behavior and then to internalizing/externalizing symptoms, and one for the path from intervention condition to placement changes and then to internalizing/externalizing symptoms) were significant (β = -.11, p = .03). However, these paths were not significant individually. This suggests that although the MSS intervention has significant influence on reducing substance use indirectly through increased prosocial behavior and decreased internalizing/externalizing symptoms, the full path from the intervention condition to substance use did not meet statistical significance as a mediation path. However, the estimate for the direct effects of intervention condition on substance use was β = -.42 (p = .01), confirming the significant direct effects of the intervention on substance use.
Figure 2.
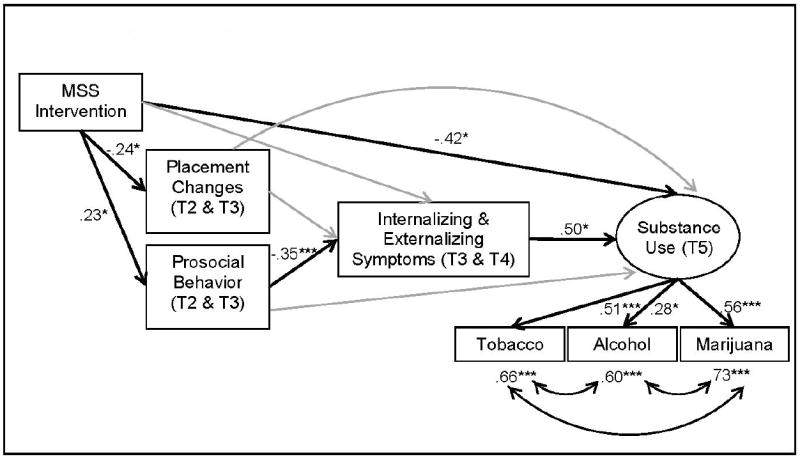
MSS Effects on Substance Use
Direct and Indirect Effects of the Intervention on Delinquency
Similar to the substance use model, the delinquency model fit the data well with a chi-square of 9.25, df = 10, p = .51, CFI = 1.00, TLI = 1.02, RMSEA = .00. Both indicators significantly loaded on the delinquency latent factor. As in the substance use model, there were significant direct intervention effects on placement changes and prosocial behavior, with the intervention associated with decreased placement changes and increased prosocial behavior. The girls’ prosocial behavior then led to reduced internalizing/externalizing symptoms. However, girls’ internalizing/externalizing symptoms were not significantly related to their delinquency. Instead, the direct path from prosocial behavior to delinquency was significant (inverse association). Nineteen percent of the variance in delinquency was accounted for by the model (p = .04). The significance tests of all of the indirect paths in the model revealed that none had significant mediating effects. On the other hand, the direct path from girls’ prosocial behavior to delinquency was significant, in the expected inverse direction (β = -.30, p = .03).
Discussion
Results of recent surveys have highlighted the critical need for preventive interventions for girls in foster care to reduce their risk for problem behaviors before the transition into young adulthood (Courtney et al., 2005; Courtney & Dworsky, 2006; Leve & Chamberlain, 2007). However, there has been very little research on developmental pathways leading to substance use and delinquency among early adolescent girls in foster care to guide such intervention efforts. This study examined the efficacy of the MSS, a preventive intervention program for early adolescent girls in foster care, focusing on the girls’ substance use and delinquent behavior. The intervention was designed to promote placement stability and increase positive social skills to reduce girls’ risk for health risking behaviors.
The first goal of this study was to examine mean differences in substance use and delinquency between girls in the MSS intervention condition and girls in the control condition. As hypothesized, findings confirmed that girls in the MSS intervention condition had significantly lower levels of substance use than girls in the control condition at 36 months postbaseline, indicating significant intervention effects on the prevention of substance use among girls in foster care. The final model incorporated a latent factor of substance use; however, examination of the individual substances using t-tests suggested that the MSS intervention was especially effective in reducing risk for tobacco and marijuana use, as reflected in significantly lower levels of tobacco and marijuana use in the past 12 months for the girls in the MSS intervention condition compared to girls in the control condition. The significant intervention effect on marijuana use is very encouraging (Cohen’s d = .57), given that a recent survey indicated that a majority of illicit drug users report marijuana as their first drug (56.6%) (SAMHSA, 2009). The lack of intervention effect on alcohol use is somewhat unexpected. It is possible that our measure (which relied solely on frequency of use) was not sensitive enough to fully evaluate the intervention effects. Furthermore, it is important to note that multi-substance use is a norm rather than an exception (Brecht, Huang, Evans, & Hser, 2008). Our sample corroborates this: of the 30 girls who reported using alcohol in the past year, 22 also reported using tobacco and/or marijuana. Therefore, it is difficult to determine intervention effects that are unique to alcohol use. However, the overall intervention effects on substance use are noteworthy, considering that this is the first study of which we are aware to examine an intervention targeting the prevention of substance use among girls in foster care.
On the other hand, the intervention did not have a direct effect on the girls’ delinquency. Group differences in the girls’ delinquent behavior were only marginally significant in both the multivariate model and at the bivariate level, suggesting that direct effects of the MSS may be somewhat weaker for delinquency than for substance use. This finding may partly be due to the limited sample size but it is also possible that the MSS intervention had an indirect influence on delinquency through other pathways among girls in foster care, which was examined as the next aim of this study, discussed below.
While the direct effects of the intervention remained significant for substance use in the presence of other indirect paths, the MSS influenced delinquent behavior among girls in foster care indirectly through their prosocial skills. These findings have various theoretical and clinical implications. First, although substance use and delinquency are often related, evidence has suggested that there might be distinctive etiological mechanisms involved for each domain. Our finding is in line with the literature (e.g., Chamberlain et al., 2007) and suggests that preventive intervention efforts may need to attend different processes for substance use and delinquency for foster girls. Second, although the tests for mediation effects did not meet statistical significance, the significant indirect paths through prosocial behavior highlight the importance of prosocial skills among girls in foster care for both outcomes. This finding supports the existing literature on the causal link from social competence in childhood to reduced internalizing and externalizing symptoms in adolescence, and onto to the development of psychopathology in young adulthood (e.g., Burt, Obradovic, Long, & Masten, 2008), especially for youth in foster care (Cicchetti, 1990). In particular, the significant direct protective effects of prosocial skills on delinquency among girls in foster care implies that facilitating the development of positive social skills in early adolescence reduces the likelihood of involvement in delinquent acts in mid adolescence (which corresponds to the last year in middle school in the present study). Although it remains to be tested whether the potential influence of prosocial skills on delinquency extends into late adolescence and young adulthood for girls in foster care, our findings provide encouraging preliminary evidence for the clinical utility of targeting prosocial skills in early adolescent girls in foster care to buffer the early adverse experiences and to engender positive trajectories in the future.
The significant intervention effect on placement stability is also noteworthy. Although the number of placement changes was not significant as a mediator in the model, girls assigned to the MSS intervention condition did have significantly fewer placement changes than girls in the control condition over the 12 months after baseline. Studies have shown that children’s problem behaviors are closely linked to placement disruption (Chamberlain et al., 2006). Furthermore, placement instability contributes to increases in adjustment problems among youth in foster care (Fisher et al., 2009; Price et al., 2008). Therefore, increasing placement stability may increase the likelihood of positive downstream effects for foster children and their families. Placement disruptions are also costly to the child welfare system (Fisher et al., 2009); as such, although not examined in the present study, the success of the MSS intervention in reducing placement failures is likely to produce significant taxpayer savings.
Another important aspect of the MSS intervention is its attention to the middle school transition. Studies on the general population indicate that the middle school transition is a critical period in which many children struggle to meet academic and social expectations (Chung et al., 1998; Moilanen et al., 2010). Given that many girls in foster care have experienced early adversities, this period may be particularly challenging and existing difficulties may be easily exacerbated during this transition. However, the MSS intervention utilizes this vulnerable period as a turning point to improve or re-direct potentially negative trajectories (Chamberlain et al., 2006). The overall effects of the MSS intervention indicate that the middle school transition may provide an optimal window to reduce problem behaviors through preventive interventions, especially by increasing prosocial behavior, leading to a cascading effect on reduced substance use and delinquent behaviors among girls in foster care.
Several limitations should be noted. First, the majority of children in the study were Caucasian (63%). Although this was representative of youth in foster care in the study region, replication in more ethnically diverse populations is warranted. Second, the sample size was small (N = 100) which could have compromised our ability to detect smaller effect sizes. In particular, the lack of significance of mediating paths in both models might have been due to the limited sample size. Third, because many variables relied on a single measure, the robustness of the findings should be further investigated. More specifically, the prosocial measure from the PDR was collected from caregivers, and therefore primarily measured the girls’ behavior in the home setting; future work needs to broaden the scope of this measure to capture the girls’ behavior across variety of settings, including the school and peer context. It is also important to note that due to study focus on the girl’s behavior and the more limited focus on parenting measures, we did not include an assessment of intervention effects on parenting behaviors in the present study. Furthermore, data from multiple informants for each construct would have been ideal to increase measurement reliability. We attempted to minimize the potential issues due to shared method variance by utilizing child welfare systems records (i.e., placement changes), caregiver reports (i.e., prosocial behavior and internalizing and externalizing behavior), and the girls’ self-reports (i.e., outcome measures). Because this is the first intervention study of which we are aware that focuses on middle school girls in foster care, the efficacy of the MSS intervention warrants further testing with larger and more ethnically diverse samples, including boys in foster care, before recommendations for dissemination efforts can be drawn.
The present study contributes to the field by demonstrating the efficacy of a unique preventive intervention program designed to prevent health-risking behaviors among early adolescent girls in foster care. The present study utilized a longitudinal RCT design to examine intervention effects on 36-month outcomes. Findings support the argument that potential risks for substance use and delinquent behavior among girls in foster care can be effectively reduced when preventive programs target relevant processes that encompass immediate developmental needs of foster girls. The present study also evidenced that the transition to middle school can be an ideal period for preventive interventions for girls in foster care. Although longer-term effects into late adolescence and young adulthood remain to be seen, the present study indicates the potential clinical value of the MSS intervention in promoting adjustment during middle adolescence.
Figure 3.
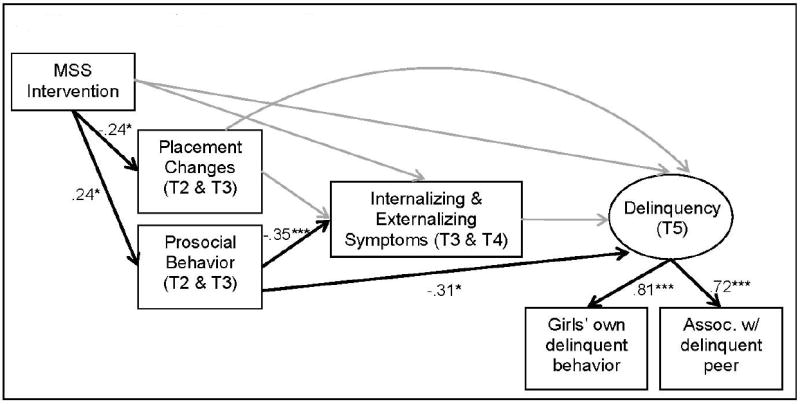
MSS Effects on Delinquency
Acknowledgments
This research was supported by the following grants: MH054257, NIMH, U.S. PHS; DA023920, DA024672, and DA027091, NIDA, U.S. PHS. The authors thank Patti Chamberlain and Dana Smith for their input, Courtenay Padgett, Priscilla Havlis, and Danielle Guerrero for project coordination, Michelle Baumann and Diana Strand for editorial assistance, and the children and families who participated in the project.
Footnotes
At the 12-month postbaseline assessment, 16.7% of the girls in the control condition and 6.4% of the girls in the intervention condition were reunited with biological parent(s) or were adopted. In addition, one girl from the control condition was in a residential/group care program at the 12-month follow-up. At the 36-month postbaseline assessment, a total of 22.2% and 13.6% of the girls in the control condition and intervention condition were reunited with biological parent(s) or were adopted, and one girl from each condition was in a residential/group care program.
Publisher's Disclaimer: The following manuscript is the final accepted manuscript. It has not been subjected to the final copyediting, fact-checking, and proofreading required for formal publication. It is not the definitive, publisher-authenticated version. The American Psychological Association and its Council of Editors disclaim any responsibility or liabilities for errors or omissions of this manuscript version, any version derived from this manuscript by NIH, or other third parties. The published version is available at www.apa.org/pubs/journals/ccp.
References
- Achenbach TM, Rescorla LA. Manual for the ASEBA School Age Forms and Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families; 2001. [Google Scholar]
- Arbuckle JL. Full information estimation in the presence of incomplete data. In: Marcoulides GA, Schumacker RE, editors. Advanced structural equation modeling: Issues and techniques. Hillsdale, NJ: Erlbaum; 1996. pp. 243–277. [Google Scholar]
- Barth RP, Weigensberg EC, Fisher PA, Fetrow RA, Green RL. Reentry of elementary aged children following reunification from foster care. Children and Youth Services Review. 2008;30:353–364. doi: 10.1016/j.childyouth.2007.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brecht ML, Huang D, Evans E, Hser YI. Polydrug use and implications for longitudinal research: Ten-year trajectories for heroin, cocaine, and methamphetamine users. Drug and Alcohol Dependence. 2008;96:193–201. doi: 10.1016/j.drugalcdep.2008.01.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns BJ, Phillips SD, Wagner HR, Barth RP, Kolko DJ, Campbell Y, Landsverk J. Mental health need and access to mental health services by youths involved with child welfare: A national Survey. Journal American Academy of Child & Adolescent Psychiatry. 2004;43:960–970. doi: 10.1097/01.chi.0000127590.95585.65. [DOI] [PubMed] [Google Scholar]
- Burt KB, Obradović J, Long JD, Masten AS. The interplay of social competence and psychopathology over 20 years: Testing transactional and cascade models. Child Development. 2008;79:359–374. doi: 10.1111/j.1467-8624.2007.01130.x. [DOI] [PubMed] [Google Scholar]
- Carlo G, Fabes RA, Laible D, Kupanoff K. Early adolescent and prosocial/moral behavior II: The role of social and contextual influences. Journal of Early Adolescence. 1999;19:133–147. [Google Scholar]
- Chamberlain P. Treating chronic juvenile offenders: Advances made through the Oregon multidimensional treatment foster care model. Washington, DC: American Psychological Association; 2003. [Google Scholar]
- Chamberlain P, Leve LD, DeGarmo DS. Multidimensional treatment foster care for girls in the juvenile justice system: 2-year follow-up of a randomized clinical trial. Journal of Consulting and Clinical Psychology. 2007;75:187–193. doi: 10.1037/0022-006X.75.1.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Leve LD, Smith DK. Preventing behavior problems and health-risking behaviors in girls in foster care. International Journal of Behavioral and Consultation Therapy. 2006;4:518–530. doi: 10.1037/h0101004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Price J, Leve LD, Laurent H, Landsverk JA, Reid JB. Prevention of behavior problems for children in foster care: Outcomes and mediation effects. Prevention Science. 2008;9:17–27. doi: 10.1007/s11121-007-0080-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chamberlain P, Reid JB. Parent observation and report of child symptoms. Behavioral Assessment. 1987;9:97–109. [Google Scholar]
- Chassin L, Pitts SC, DeLucia C, Todd M. A longitudinal study of children of alcoholics: Predicting young adult substance use disorders, anxiety, and depression. Journal of Abnormal Psychology. 1999;108:106–119. doi: 10.1037/0021-843X.108.1.106. [DOI] [PubMed] [Google Scholar]
- Chung H, Elias M, Schneider K. Patterns of individual adjustment changes during middle school transition. Journal of School Psychology. 1998;36:83–101. doi: 10.1016/S0022-4405(97)00051-4. [DOI] [Google Scholar]
- Cicchetti D. The organization and coherence of socioemotional, cognitive, and representational development: Illustrations through a developmental psychopathology perspective on Down syndrome and child maltreatment. In: Thompson R, editor. Nebraska symposium on motivation: Socioemotional development. Vol. 36. Lincoln, NE: University of Nebraska Press; 1990. pp. 259–366. [PubMed] [Google Scholar]
- Courtney ME, Dworsky A. Early outcomes for young adults transitioning from out-of-home care in the USA. Child and Family Social Work. 2006;11:209–219. doi: 10.1111/j.1365-2206.2006.00433.x. [DOI] [Google Scholar]
- Courtney ME, Dworsky A, Ruth G, Keller T, Havlicek J, Bost N. Midwest evaluation of the adult functioning of former foster youth: Outcomes at age 19. Chicago: Chapin Hall Center for Children at the University of Chicago; 2005. [Google Scholar]
- Cusick GR, Courtney ME. Offending during late adolescence: How do youth aging out of care compare with their peers? Chicago: Chapin Hall at the University of Chicago; 2007. [Google Scholar]
- DiGiuseppe DL, Christakis DA. Continuity of care for children in foster care. Pediatrics. 2003;111:e208–e213. doi: 10.1542/peds.111.3.e208. [DOI] [PubMed] [Google Scholar]
- Dworsky A, DeCoursey J. Pregnant and parenting foster youth: Their needs, their experiences. Chicago: Chapin Hall at the University of Chicago; 2009. [Google Scholar]
- Eddy JM, Chamberlain P. Family management and deviant peer association as mediators of the impact of treatment condition on youth antisocial behavior. Journal of Consulting and Clinical Psychology. 2000;68:857–863. doi: 10.1037//0022-006X.68.5.857. [DOI] [PubMed] [Google Scholar]
- Elliott DS, Huizinga D, Ageton SS. Explaining delinquency and drug use. Beverly Hills, CA: Sage; 1985. [Google Scholar]
- Fisher PA, Kim HK, Pears KC. Effects of Multidimensional Treatment Foster Care for Preschoolers (MTFC-P) on reducing permanent placement failures among children with placement instability. Child and Youth Services Review. 2009;31:541–546. doi: 10.1016/j.childyouth.2008.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harden BJ. Safety and stability for foster children: A developmental perspective. Future of Children. 2004;14:31–47. doi: 10.2307/1602753. [DOI] [PubMed] [Google Scholar]
- Hipwell AE, Loeber R. Do we know which interventions are effective for disruptive and delinquent girls? Clinical Child and Family Psychology Review. 2006;9:221–255. doi: 10.1007/s10567-006-0012-2. [DOI] [PubMed] [Google Scholar]
- Jonson-Reid M, Barth RP. From placement to prison: The path to adolescent incarceration from child welfare supervised foster or group care. Children and Youth Services Review. 2000;22:493–515. [Google Scholar]
- Jonson-Reid M, Scott LD, Jr, McMillen JC, Edmond T. Dating violence among emancipating foster youth. Children and Youth Services Review. 2007;29:557–571. doi: 10.1016/j.childyouth.2006.12.008. [DOI] [Google Scholar]
- Keller TE, Salazar AM, Courtney ME. Prevalence and timing of diagnosable mental health, alcohol, and substance use problems among older adolescents in the child welfare system. Children and Youth Services Review. 2010;32:626–634. doi: 10.1016/j.childyouth.2009.12.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenig AL, Cicchetti D, Rogosch FA. Moral development: The association between maltreatment and young children’s prosocial behaviors and moral ransgressions. Social Development. 2004;13:87–106. [Google Scholar]
- Kohlenberg E, Nordlund D, Lowin A, Treichler B. Alcohol and substance use among adolescents in foster care in Washington State: Results from the 1998-1999 Adolescent Foster Care Survey. Rockville, MD: Center for Substance Abuse Treatment; 2002. [Google Scholar]
- Leve LD, Chamberlain P. Girls in the juvenile justice system: Risk factors and clinical implications. In: Pepler D, Madsen K, Webster C, Levine K, editors. The development and treatment of girlhood aggression. Mahway, NJ: Lawrence Erlbaum Associates; 2005. pp. 191–215. [Google Scholar]
- Leve LD, Chamberlain P. A randomized evaluation of Multidimensional Treatment Foster Care: Effects on school attendance and homework completion in juvenile justice girls. Research on Social Work Practice. 2007;17:657–663. doi: 10.1177/1049731506293971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leve LD, Chamberlain P, Reid JB. Intervention outcomes for girls referred from juvenile justice: Effects on delinquency. Journal of Consulting and Clinical Psychology. 2005;73:1181–1185. doi: 10.1037/0022-006X.73.6.1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lochman JE, Wells KC. The coping power program at the middle-school transition: Universal and indicated prevention effects. Psychology of Addictive Behavior. 2002;16:S40–S54. doi: 10.1037/0893-164X.16.4S.S40. [DOI] [PubMed] [Google Scholar]
- Luthar SS, Cicchetti D. The construct of resilience: Implications for interventions and social policies. Development & Psychopathology. 2000;12:857–885. doi: 10.1017/S0954579400004156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacMillan HL, Wathen CN, Barlow J, Fergusson DM, Leventhal JM, Taussig HN. Interventions to prevent child maltreatment and associated impairment. The Lancet. 2009;393:250–266. doi: 10.1016/S0140-6736(08)61708-0. [DOI] [PubMed] [Google Scholar]
- Marmorstein NR, White H, Chung T, Hipwell A, Stouthamer-Loeber M, Loeber R. Association between first use of substances and change in internalizing symptoms among girls: Differences by symptom trajectory and substance use type. Journal of Clinical Child & Adolescent Psychology. 2010;39:545–558. doi: 10.1080/15374416.2010.486325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClowry SG, Snow DL, Tamis-LeMonda CS. An evaluation of the effects of INSIGHTS on the behavior of inner city primary school children. Journal of Primary Prevention. 2005;26:567–584. doi: 10.1007/s10935-005-0015-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moilanen KL, Shaw DS, Maxwell KL. Developmental cascades: Externalizing, internalizing, and academic competence from middle childhood to early adolescence. Development and Psychopathology. 2010;22:635–653. doi: 10.1017/S0954579410000337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. 6. Los Angeles: Muthén & Muthén; 1998-2010. [Google Scholar]
- Pecora PJ. Why current and former recipients of foster care need high quality mental health services. Administration and Policy in Mental Health and Mental Health Services Review. 2010;37:185–190. doi: 10.1007/s10488-010-0295-y. [DOI] [PubMed] [Google Scholar]
- Pecora PJ, Williams J, Kessler RJ, Downs AC, O’Brien K, Hiripi E, Morello S. Assessing the effects of foster care: Early results from the Casey National Alumni Study. Seattle, WA: Casey Family Programs; 2003. [Google Scholar]
- Price JM, Chamberlain P, Landsverk J, Reid J, Leve L, Laurent H. Effects of a foster parent training intervention on placement changes of children in foster care. Child Maltreatment. 2008;13:64–75. doi: 10.1177/1077559507310612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pursell GR, Laursen B, Rubin KH, Booth-LaForce C, Rose-Krasnor L. Gender differences in patterns of association between prosocial behavior, personality, and externalizing problems. Journal of Research in Personality. 2008;42:472–481. doi: 10.1016/j.jrp.2007.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubin DM, Alessandrini EA, Feudtner C, Mandell DS, Localio AR, Hadley T. Placement stability and mental health costs for children in foster care. Pediatrics. 2004;113:1336–1341. doi: 10.1542/peds.113.5.1336. [DOI] [PubMed] [Google Scholar]
- Ryan JP, Testa MF. Child maltreatment and juvenile delinquency: Investigating the role of placement and placement instability. Children and Youth Services Review. 2005;27:227–249. doi: 10.1016/j.childyouth.2004.05.007. [DOI] [Google Scholar]
- Smith DK, Leve LD, Chamberlain PC. Preventing internalizing and externalizing problems in girls in foster care as they enter middle school: Immediate impact of an intervention. Prevention Science. doi: 10.1007/s11121-011-0211-z. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA), Office of Applied Studies. The National Survey on Drug Use and Health report: Substance use and need for treatment among youths who have been in foster care. Rockville, MD: Author; 2005. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Results from the 2008 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, NSDUH Series H-36, HHS publication No SMA-09-4434) Rockville, MD: 2009. [Google Scholar]
- Taussig HN, Clyman RB, Landsverk J. Children who return home from foster care: A 6-year prospective study of behavioral health outcomes in adolescence. Pediatrics. 2001;108:e10. doi: 10.1542/peds.108.1.e10. [DOI] [PubMed] [Google Scholar]
- Theriot MT, Dupper DR. Student discipline problems and the transition from elementary to middle school. Education and Urban Society. 2010;42:205–22. doi: 10.1177/0013124509349583. [DOI] [Google Scholar]
- Thompson RG, Jr, Auslander WF. Risk factors for alcohol and marijuana use among adolescents in foster care. Journal of Substance Abuse Treatment. 2007;32:61–69. doi: 10.1016/j.jsat.2006.06.010. [DOI] [PubMed] [Google Scholar]
- White CR, O’Brien K, White J, Pecora PJ, Phillips CM. Alcohol and drug use among alumni of foster care: decreasing dependency through improvement of foster care experiences. Journal of Behavioral Health Services & Research. 2007;35:419–434. doi: 10.1007/s11414-007-9075-1. [DOI] [PubMed] [Google Scholar]