

Abstract
Small cell osteosarcoma, a rare histological subtype, has very infrequently been reported in the mandible. We present a case of a 28-year-old female who had classic signs, symptoms, and radiographic features of the lesion. The histology showed sheets of small round cells and osteoid. The absence of the latter would have made it difficult to distinguish from other small round cell tumors of bone, especially Ewing's sarcoma. We have reviewed the clinical and radiographic features, cytologic and histologic characteristics, as well as the immunohistochemistry and molecular genetics of small cell osteosarcoma.
Keywords: Ewing's sarcoma, mandible, osteoid, round cell tumor of bone, small cell osteosarcoma, sunburst
INTRODUCTION
Small cell osteosarcoma is a rare histological subtype of osteosarcoma. It was first described in 1979 by Sim et al. as resembling Ewing's tumor, being made up of small round cells.[1] Small cell osteosarcoma affecting the mandible is even rarer, with only three published cases available in the literature.[2–4] We present a case of small cell osteosarcoma of the mandible with a review of its clinical and radiographic features, its cytologic and histologic characteristics, as well as its immunohistochemistry and molecular genetics.
CASE REPORT
The patient was a 28-year-old lady with a complaint of a painful swelling in the angle region of her left mandible for the past 3 months [Figure 1]. She had visited a local dentist for the problem a month ago, who extracted her second and third left mandibular molars, which made no difference to the pain or swelling. She said that the swelling gradually increased to the present size. She gave no history of trauma to the area, and had no idea about the status of the extracted teeth. The patient was married and was 9 weeks pregnant. She also appeared weak and said she was unable to eat properly due to the pain. On extra-oral palpation, the swelling was bony hard and tender. The left submandibular group of nodes was enlarged and tender, but mobile. Intra-oral examination showed that the extraction wound had not healed completely; there was a thin fibrinous pseudomembrane over it. The swelling had obliterated the buccal vestibule, but the mucosa appeared normal. An orthopantomogram revealed a poorly defined radiolucency with radially oriented radio-opaque streaks, giving a “sunburst” appearance. The lesion occupied the entire ramus and angle region extending up to the lower border of the mandible [Figure 2]. Since the patient was in the first trimester of pregnancy, the obstetrician's consent was sought to conduct an incisional biopsy, approaching through the unhealed extraction socket. A fine needle aspiration was also done at the same time. The cytosmear showed small round cells singly and in clusters, with moderate anisonucleosis. The cytoplasm was scanty and the chromatin was finely granular with no nucleoli [Figure 3]. A provisional diagnosis of a small round cell tumor of bone was given. The histological section showed dense infiltration of soft tissue by small round blue cells with scanty cytoplasm, which were not arranged in any particular pattern [Figure 4]. Some areas of spindled cells were also seen [Figure 5]. Areas of tumor osteoid with bizarre osteocytes were present, very similar to those seen in conventional osteosarcoma [Figure 6]. Based on these features, a diagnosis of small cell osteosarcoma was made. The patient had her pregnancy terminated, and underwent a PET scan, which showed no distant metastases. She underwent a mandibular resection and has been started on chemotherapy now, after recovering from the surgery. So far, there is no evidence of recurrence of the lesion.
Figure 1.

Swelling of the left mandibular angle
Figure 2.

OPG showing poorly defined radiolucency with “sunburst” appearance
Figure 3.
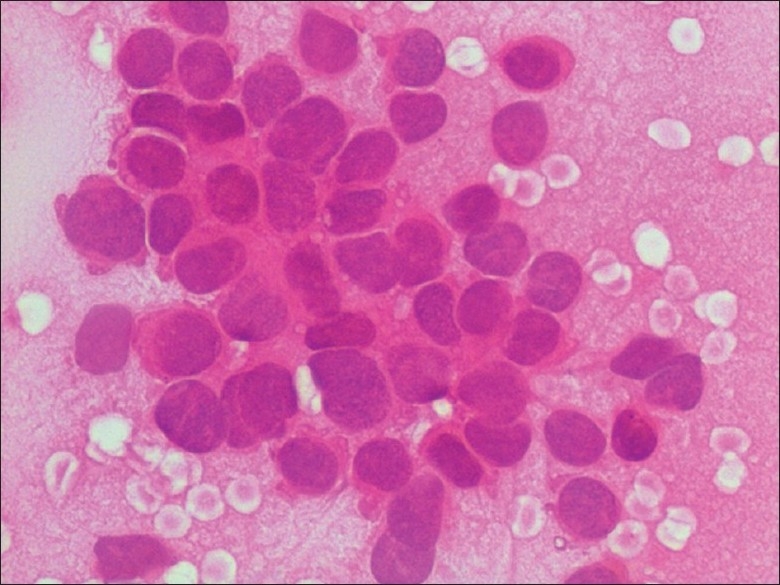
FNA smear showing a cluster of small round cells showing scanty cytoplasm, granular chromatin, absent nucleoli, and moderate anisonucleosis (H and E, 400×)
Figure 4.
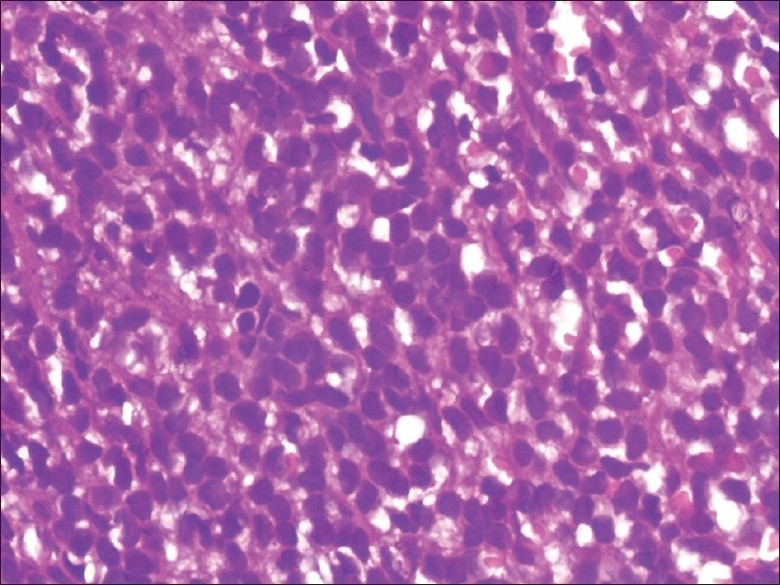
Histologic section showing small round cells arranged in sheet-like pattern, with moderate anisonucleosis (H and E, 400×)
Figure 5.
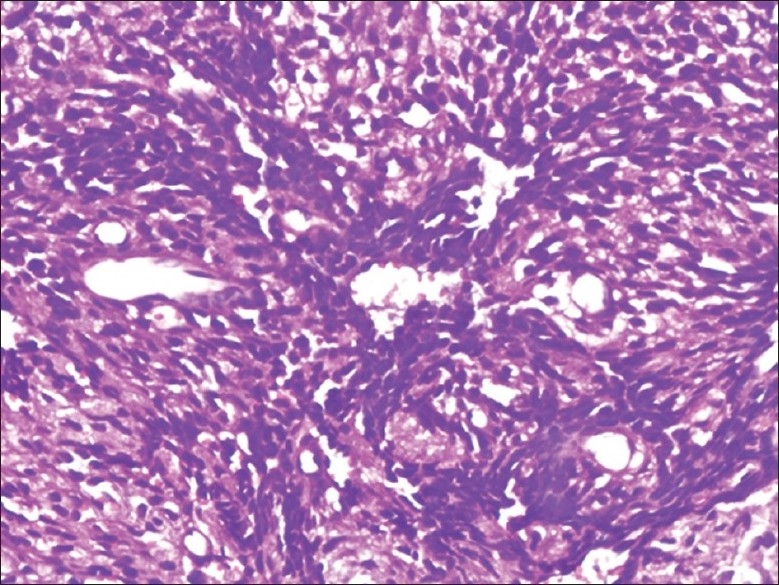
Histologic section showing area of spindled cells (H and E, 200×)
Figure 6.
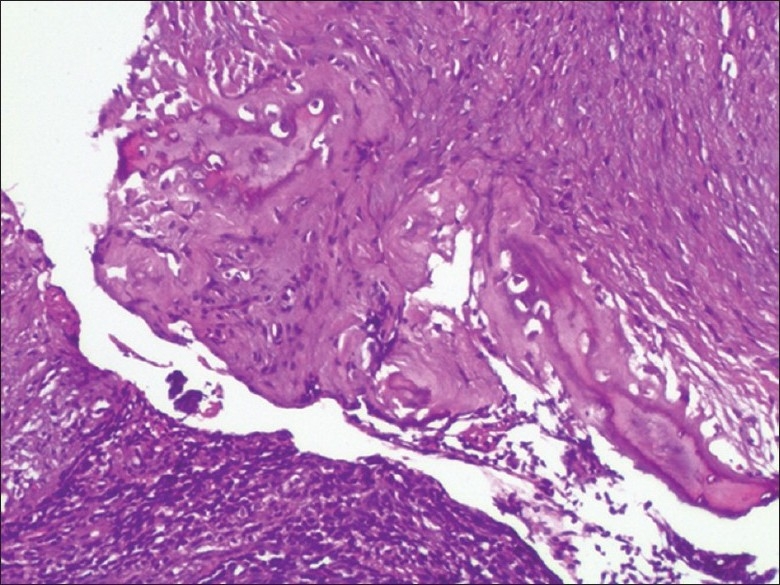
Histologic section showing area of osteoid with bizarre osteocytes (H and E, 100×)
DISCUSSION
Osteosarcoma has several histological variants,[5] of which the small cell osteosarcoma is quite rare. The incidence is said to vary from 1.3%[6] to 4%.[7] The skeletal distribution and age range of patients affected by small cell osteosarcoma are similar to those of conventional osteosarcoma.[7] However, in the first description of the entity, Sim et al. have stated that the age range is wider than that of patients with classic osteosarcoma or Ewing's sarcoma, with almost half occurring in the third decade of life.[1] Small cell osteosarcomas have been reported from almost every part of the skeleton, including extragnathic craniofacial bones,[8] as well as extraskeletal locations.[9–11]
Osteosarcomas affecting the jawbones constitute about 6% of the total.[12] Small cell osteosarcomas of the jawbones, however, are extremely rare. There are only three case reports in the literature,[2–4] and three more mandibular tumors are part of studies of larger series of cases.[7,13]
The most common clinical presentation of small cell osteosarcoma is pain and swelling with durations varying from a few days to several months.[1,6,7,14,15] Patients have also presented with numbness[14] and pathological fractures.[16] Our patient complained of difficulty in eating caused by her painful mandibular swelling.
Radiographically, small cell osteosarcoma usually shows a poorly demarcated radiolucency which may be purely lytic, or may be mixed lytic–blastic.[1,6,7,14–16] Destruction of the cortex[1,6,7,14,16] with elevation of the periosteum (Codman's triangle),[14,17] periosteal new bone formation[1,6,14,15] and soft tissue extension[1,6,7,14,16] have been described. The classic “sunburst” appearance of osteosarcoma also occurs,[14,17] as in our case. The presence of calcified matrix in the tumor, especially when no osteoid is seen in the biopsy, is an important clue to the diagnosis of small cell osteosarcoma, which can otherwise look like any small round cell tumor, especially Ewing's sarcoma.[6,18]
There are very few accounts of the cytology of small cell osteosarcoma.[15,19,20] White et al. have described the tumor cells as being “approximately three to four times the size of a mature lymphocyte,” with scanty cytoplasm and finely dispersed chromatin. The cells were seen to be present singly, as well as in clusters. The nuclei exhibited greater variability in shape, with oval and spindled nuclei. These latter features help differentiate small cell osteosarcoma from Ewing's sarcoma, in which the cells are dispersed singly, and have round, uniform nuclei.[19] In their detailed study of the cytologic characteristics of small cell osteosarcoma, Bishop et al. have described the tumor cells as being small- to intermediate-sized, with high nuclear/cytoplasmic ratios, round hyperchromatic nuclei with finely granular chromatin and fine cytoplasmic vacuoles. The nuclei showed significant molding in some cases, and minimal anisonucleosis. They also obtained osteoid in some of their cases, which stained faint purple or metachromatic with Romanovsky stain and pale green with Papanicolaou stain. The osteoid surrounded the cells and appeared wispy or lacy with ill-defined borders, unlike collagen, which also shows naked fibroblast nuclei.[15] Our case also showed similar cytologic features, except that we did not get any osteoid, cytoplasmic vacuoles were absent, and the nuclei were slightly more pleomorphic.
The histologic picture of small cell osteosarcoma consists of small round cells arranged in islands or sheets,[1,16] sometimes separated by septae of dense fibrous tissue.[1,6] In some tumors, hemangiopericytomatous areas may be seen.[1,6,16] Areas of myxoid tissue may be present;[6] in some cases associated with chondroid tissue.[1,14] Areas of necrosis may also occur.[1,13,16] In some cases, the cells may be arranged in strands and cords.[6] Epithelioid cells arranged in nests or gland-like structures have also been described.[6] Our case showed sheets of round cells with areas of dense fibrous tissue and a focal area of myxoid tissue. The cells were round to oval in shape with scanty cytoplasm.[1,14,16] Some areas of spindled cells have been noted.[1,6,7,16] The nuclei were usually round or oval showing variability in size.[1,6,7,14,16] The nuclear chromatin was finely dispersed[1,6,7,14,16] with some cases described as having vesicular chromatin[13] or hyperchromatic and coarse chromatin.[6] The nucleoli varied from indistinct to prominent.[1,6,7,13,14,16] Mitotic figures were present and varied widely.[1,6,7,13,16] Ayala et al.[7] have classified the tumor into three histological types based on cell morphology: Ewing's sarcoma – like in which the histology closely resembled Ewing's sarcoma, with cells showing scanty cytoplasm and round nuclei with fine chromatin and inconspicuous nucleoli; lymphoma – like pattern resembling large cell lymphoma showing large cells with abundant cytoplasm, round to oval nuclei, finely dispersed chromatin and prominent nucleoli; spindle cell pattern showed cells with scanty cytoplasm and short ovoid or spindle-shaped nuclei with inconspicuous or no nucleoli. In tumors with multiple patterns, the predominant pattern determined the type.[7] According to this classification, our case fits the Ewing's sarcoma – like pattern, as it predominantly shows small round cells with scanty cytoplasm with finely dispersed nuclear chromatin, no nucleoli and moderate anisonucleosis. The defining histologic feature of small cell osteosarcoma is the presence of osteoid, which has been described in each and every case reported so far. It varies from fine, lace-like deposits around the tumor cells,[1,6,7,14,16,21] to larger areas of calcified matrix.[1,6,14,21] Several cases also showed cartilage formation[1,6,7,13,14,16,17] often closely associated with the osteoid. Our case showed calcified osteoid in one area, and a smaller area of uncalcifed osteoid with bizarre osteocytes, quite similar to that seen in conventional osteosarcoma.
Staining for the presence of glycogen and reticulin showed variable results and was not helpful in differential diagnosis. Sim et al. found all their cases to be PAS negative, while many other cases were PAS positive.[6,7,13,14,16] Reticulin was positive in some studies, forming an intercellular network,[1,16] being virtually absent in some, and surrounding a few to several tumor cells in others.[13] One case, with multiple skeletal metastases, was positive for alkaline phosphatase.[17]
Though the histologic differential diagnosis of small cell osteosarcoma includes several round cell tumors, it can be most easily mistaken for either Ewing's sarcoma or mesenchymal chondrosarcoma: The former when the biopsy specimen does not include any osteoid and the latter when there is presence of cartilage. The cells and nuclei in Ewing's sarcoma are more uniform than in small cell osteosarcoma. There is no osteoid formation, though on occasion, fibrin present between tumor cells may be mistaken for lacy osteoid.[1] The presence of tumor cartilage may lead one to think of mesenchymal chondrosarcoma. But most of the cases of small cell osteosarcoma show the presence of cartilage along with osteoid.[1,7,14,16,17] Mesenchymal chondrosarcoma does not show any osteoid; also, the cartilage formed is usually of low-grade malignancy, whereas high-grade malignant cartilage is seen in small cell osteosarcoma.[7]
Immunohistochemical studies have looked for a marker(s) that may help distinguish small cell osteosarcoma from other small round cell tumors.[13,15,21] CD99 (MIC2gene product/HBA71) which was thought to be a specific marker of Ewing's sarcoma, has been found to be positive in several small cell osteosarcomas,[3,4,9,11,21] though some studies have reported negative results too.[13,15] Small cell osteosarcoma has shown positivity for a variety of markers, including cytokeratins, SMA, vimentin, S100[13] and osteonectin, osteocalcin, cell membrane proteins ezrin and caveolin-1.[21] The most useful differentiation is from lymphomas/leukemias, as small cell osteosarcomas have shown consistently negative results for lymphoid markers like LCA, B- and T-cell markers.[4,13,15,21]
The latest area of study is molecular genetics and cytogenetics of small cell osteosarcoma. Machado et al. looked for sarcoma-associated translocations, especially those related to the EWS gene, without any conclusive results.[21] Pellin et al. in a study of several round cell tumors for the translocation (11:22) (q24;q12), found it to be present in Ewing's sarcomas and PNETs, and absent in other round cell tumors, including small cell osteosarcoma.[22] A recent study by Lee et al. on Fli-1 expression in round cell tumors found that it is expressed in Ewing's sarcoma and lymphoblastic lymphoma and negative in mesenchymal chondrosarcoma and small cell osteosarcoma.[23] Further studies are needed in this area. Many of the reviewed studies showed small cell osteosarcoma to have a poor prognosis.[1,6,7,15,16] Nakajima et al.[6] found that their series of patients showed an overall 5-year survival rate of 28.6% compared to conventional osteosarcoma (77%) and Ewing's sarcoma (50%). Sethi et al.[4] believe that a juxtacortical small cell osteosarcoma may have a better prognosis, as it is likely to grow relatively slower. While a review of treatment methods is beyond the scope of this article, it appears that adjuvant chemotherapy improves the prognosis[6] as compared to only surgery.
We have presented a rare case of mandibular small cell osteosarcoma with classic clinical, radiographic, cytologic, and histologic features. The diagnosis of this lesion, if not obvious from histology, can be made using adjunctive techniques such as immunohistochemistry and molecular genetics.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Sim FH, Unni KK, Beabout JW, Dahlin DC. Osteosarcoma with small cells simulating Ewing's tumor. J Bone Joint Surg Am. 1979;61:207–15. [PubMed] [Google Scholar]
- 2.Giangaspero F, Stracca V, Visona A, Eusebi V. Small cell osteosarcoma of the mandible. Case report. Appl Pathol. 1984;2:28–31. [PubMed] [Google Scholar]
- 3.Kim YM, Yang SW, Cho MY, Hong SW, Choi BH. Small cell osteosarcoma similar to Ewing's sarcoma in histologic findings and MIC2 expression. Korean J Pathol. 1999;33:204–9. [Google Scholar]
- 4.Sethi A, Rehani S, Arya K. Small cell osteosarcoma of mandible: A rare case report and review of literature. J Clin Exp Dent. 2010;2:e96–9. [Google Scholar]
- 5.Klein MJ, Siegal GP. Osteosarcoma: Anatomic and histologic variants. Am J Clin Pathol. 2006;125:555–81. doi: 10.1309/UC6K-QHLD-9LV2-KENN. [DOI] [PubMed] [Google Scholar]
- 6.Nakajima H, Sim FH, Bond JR, Unni KK. Small cell osteosarcoma of bone. Review of 72 cases. Cancer. 1997;79:2095–106. doi: 10.1002/(sici)1097-0142(19970601)79:11<2095::aid-cncr6>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- 7.Ayala AG, Ro JY, Raymond AK, Jaffe N, Chawla S, Carrasco H, et al. Small cell osteosarcoma. A clinicopathologic study of 27 cases. Cancer. 1989;64:2162–73. doi: 10.1002/1097-0142(19891115)64:10<2162::aid-cncr2820641031>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 8.Nora FE, Unni KK, Pritchard DJ, Dahlin DC. Osteosarcoma of extragnathic craniofacial bones. Mayo Clin Proc. 1983;58:268–72. [PubMed] [Google Scholar]
- 9.Robinson LH, Pitt MJ, Jaffe KA, Siegal GP. Small cell osteosarcoma of the soft tissue. Skeletal Radiol. 1995;24:462–5. doi: 10.1007/BF00941249. [DOI] [PubMed] [Google Scholar]
- 10.Sipos EP, Tamargo RJ, Epstein JI, North RB. Primary intracerebral small-cell osteosarcoma in an adolescent girl: Report of a case. J Neuro-oncol. 1997;32:169–74. doi: 10.1023/a:1005775818317. [DOI] [PubMed] [Google Scholar]
- 11.Yang JY, Kim JM. Small cell extraskeletal osteosarcoma. Orthopedics. 2009;32:217. [PubMed] [Google Scholar]
- 12.Clark JL, Unni KK, Dahlin DC, Devine KD. Osteosarcoma of the jaw. Cancer. 1983;51:2311–6. doi: 10.1002/1097-0142(19830615)51:12<2311::aid-cncr2820511224>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 13.Devaney K, Vinh TN, Sweet DE. Small cell osteosarcoma of bone: An immunohistochemical study with differential diagnostic considerations. Hum Pathol. 1993;24:1211–25. doi: 10.1016/0046-8177(93)90218-6. [DOI] [PubMed] [Google Scholar]
- 14.Martin SE, Dwyer A, Kissane JM, Costa J. Small-cell osteosarcoma. Cancer. 1982;50:990–6. doi: 10.1002/1097-0142(19820901)50:5<990::aid-cncr2820500529>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 15.Bishop JA, Shum CH, Sheth S, Wakely PE, Jr, Ali SZ. Small cell osteosarcoma: Cytopathologic characteristics and differential diagnosis. Am J Clin Path. 2010;133:756–61. doi: 10.1309/AJCPO07VGDZCBRJF. [DOI] [PubMed] [Google Scholar]
- 16.Bertoni F, Present D, Bacchini P, Pignatti G, Picci P, Campanacci M. The Istituto Rizzoli experience with small cell osteosarcoma. Cancer. 1989;64:2591–9. doi: 10.1002/1097-0142(19891215)64:12<2591::aid-cncr2820641231>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 17.Sanjay B, Raj GA, Vishwakarma G. A small cell osteosarcoma with multiple skeletal metastases. Arch Orthop Trauma Surg. 1988;107:58–60. doi: 10.1007/BF00463527. [DOI] [PubMed] [Google Scholar]
- 18.Edeiken J, Raymond AK, Ayala AG, Benjamin RS, Murray JA, Carrasco HC. Small cell osteosarcoma. Skeletal Radiol. 1987;16:621–8. doi: 10.1007/BF00357110. [DOI] [PubMed] [Google Scholar]
- 19.White VA, Fanning CV, Ayala AG, Raymond AK, Carrasco HC, Murray JA. Osteosarcoma and the role of fine-needle aspiration: A study of 57 cases. Cancer. 1988;62:1238–46. doi: 10.1002/1097-0142(19880915)62:6<1238::aid-cncr2820620632>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 20.Park YK, Ryu KN, Ahn JH, Yang MH. A small cell osteosarcoma on the calcaneus - a case report. J Korean Med Sci. 1995;10:147–51. doi: 10.3346/jkms.1995.10.2.147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Machado I, Alberghini M, Giner F, Corrigan M, O’Sullivan M, Noguera R, et al. Histopathological characterization of small cell osteosarcoma with immunohistochemistry and molecular genetic support. A study of 10 cases. Histopathology. 2010;57:162–67. doi: 10.1111/j.1365-2559.2010.03589.x. [DOI] [PubMed] [Google Scholar]
- 22.Pellin A, Boix J, Blesa JR, Noguera R, Carda C, Llombart-Bosch A. EWS/FLI-1 rearrangement in small round cell sarcomas of bone and soft tissue detected by reverse transcriptase polymerase chain reaction amplification. Eur J Cancer. 1994;30A:827–31. doi: 10.1016/0959-8049(94)90300-x. [DOI] [PubMed] [Google Scholar]
- 23.Lee AF, Hayes MM, Lebrun D, Espinosa I, Nielsen GP, Rosenberg AE, et al. FLI1 distinguishes Ewing's sarcoma from small cell osteosarcoma and mesenchymal chondrosarcoma. Appl Immunohistochem Mol Morphol. 2011;19:233–8. doi: 10.1097/PAI.0b013e3181fd6697. [DOI] [PubMed] [Google Scholar]