

Abstract
Context:
Vital pulp therapy has been known as one of the treatment options to preserve pulp after being exposed by trauma or caries.
Aim:
To investigate human pulpal response to white and grey mineral trioxide aggregate (WMTA, GMTA) and Dycal (MTA) as pulp capping agents.
Setting and Design:
Human volunteers were participated in this randomized clinical trial.
Materials and Methods:
This study was conducted on 90 intact first and second premolars of human maxillary and mandibular teeth. The teeth were randomly assigned into three groups of 30 each. Under local anesthesia, teeth were exposed and capped either with GMTA, WMTA, or Dycal. After 30, 60, and 90 days 10 teeth of each group were extracted and prepared for histologic observation.
Statistical Analysis:
Histopathologic data were analyzed by χ2, Kruskal Wallis and Mann Whitney tests.
Results:
the calcified bridge in teeth that were capped with GMTA was significantly thicker than Dycal at 30 and 60 days (P= 0.015 and P=0.002, respectively); whereas WMTA showed significantly thicker calcified bridge than Dycal at 90 days (P=0.02). In addition, GMTA specimens showed significantly less inflammation compared to Dycal samples at 90 days interval (P=0.019). No significant difference was found between GMTA and WMTA in terms of calcified bridge thickness and pulp inflammatory response to the capping materials (P>0.05).
Conclusions:
Based on the result of this study, both types of MTA can be suggested as the materials of choice for direct pulp capping procedure instead of Dycal as hard setting calcium hydroxide cement.
Keywords: Calcium hydroxide, direct pulp capping, grey, human teeth, mineral trioxide aggregate, vital pulp therapy, white
INTRODUCTION
Mineral trioxide aggregate (MTA) has been introduced for many clinical applications such as root-end filling, perforation repair, apical barrier for teeth with open apexes, pulp capping and pulpotomy of primary and permanent teeth.[1] In vitro and in vivo studies confirmed MTA's excellent sealing ability and biocompatibility.[2] In addition, MTA ability for hard tissue induction and conduction has been confirmed.[2]
At first MTA marketed as the grey form, but because of discoloration potential white form of the material has been introduced as well. Nowadays, MTA has been commercially available in both white and grey forms (white MTA=WMTA, grey MTA=GMTA). The major difference between GMTA and WMTA are the presence of the higher amount of aluminum, magnesium, and iron in the former material.[3,4] MTA basically consists of calcium, silica, and bismuth oxide.[3–8] After hydration MTA releases calcium hydroxide that is the reason of the high pH value of the material.[8]
Several animal studies have evaluated either white or grey MTA as pulp capping agents.[9–18] However, only one animal investigation compared both forms of MTA and reported no histologic difference between the materials as pulp capping agents in terms of calcified bridge formation and pulp inflammatory response.[14] Results of that study illustrated that pulp formed calcified bridge in response to both GMTA and WMTA as pulp capping materials after 1 and 2 weeks. Human studies that evaluate MTA either by case series or clinical trial investigations have shown favorable histologic results when the material used for pulp capping.[19–27]
Some human histologic investigations have used either WMTA or GMTA and compared them with calcium hydroxide (CH) as pulp capping agents.[19,20–24,26,27] However, so far, no published investigation has compared GMTA, WMTA, and CH at the same time. Therefore, the aim of this study was to compare both forms of MTA (GMTA and WMTA) with CH as pulp capping materials.
MATERIALS AND METHODS
The protocol of this study was approved by the Ethic Committee of Kerman University of Medical Sciences (protocol no. 10/60/5860). Ninety sound intact mandibular and maxillary first and second premolar teeth from 40 volunteers that were candidate for extraction because of orthodontic reasons were used in this study. Each volunteer or his/her parents received and signed a consent form, in which the nature of the procedure and the possible discomforts and risks had been fully explained. Inclusion criteria were consisted of health volunteers over 18 years of age, who accepted the terms of the study, having sound intact teeth, without history of trauma, with no periodontal disease involvement, having at least three premolar teeth that need extraction for orthodontic reasons. Exclusion criteria were the presence of clinical of radiographic signs of pulp or peridontal involvement, tooth anomaly, and no response to vitality tests cold, warm, or electric pulp tester. For volunteers who were under 18 years of age, the terms and nature of the study was also described to one of their parents and asked them to sign the consent form. All teeth were examined clinically and radiographically to be sure about the absence of proximal caries and periapical lesion as well as the maturity of the root apex.
For each patient after administrating local anesthesia with 3% perilocaine with 0.03 Ul felypressin (Prilonest 3%, DFL Industria, Rio de Janeiro, Brazil) the tooth was washed with 0.2% chlorhexidine prior to cavity preparation. Then a classic class V cavity was prepared at the buccal aspect of the crown and at the final part of the cavity preparation a standard small exposure was intentionally prepared as closely as possible to a size between 0.5 to 1 mm. Homeostasis was achieved by placing a cotton pellet that was moistened with normal saline over the exposure area. In case of uncontrolled bleeding, a cotton pellet moistened with 2.5% sodium hypochlorite was used for 1 min. After that, the exposure area was randomly capped with either Dycal (Dentsply DeTrey, GmbH, Konstanz, Germany), Tooth-coloured ProRoot MTA (Dentsply, Tulsa Dental, Tulsa, OK, USA) or grey ProRoot MTA (Dentsply). After placing MTA, a wet cotton palette was placed over MTA, after 10 min the cotton pellet was removed and the cavity was resorted with amalgam. For randomization, each volunteer received a sealed opaque envelope in which the type of the capping material and maxillary or mandibular teeth had been written by another person so that for volunteers who needed to extract at least three premolar teeth all of the capping materials were used. Finally, the cavities were restored with amalgam (Sinalloy, Shahid Faghihi, Tehran, Iran). All cavity preparation and tooth restoration procedures were performed by one of the authors (A. E). At 30, 60, and 90 days, ten teeth that were capped with one of the capping materials were extracted (30 teeth at each time interval). The extraction was performed as atraumatically as possible. After extraction the apical 3 mm of the root apex of each tooth was cut by a new unused high-speed diamond fissure bur with copious of water spray for increasing the amount of formalin penetration. Then teeth were stored in 10% formalin for at least 2 weeks prior to histologic processing.
After histopathological processing and H and E staining, the specimens were observed by an oral pathologist who was unaware of the type of the capping materials and the time interval under an optical microscope (Zeiss, Goettingen, Germany). The presence and thickness of complete calcified bridge, and pulp inflammation were evaluated. Pulp inflammation was determined at the coronal pulp by taking three central sections, beneath the capping material/calcified bridge. Pulp inflammation were graded and calculated based on criteria that used in a previously published study[18] with slight modification: 1 – no inflammation; 2 – minimal inflammation (scattered chronic inflammatory cells beneath the calcified bridge or capping area); 3 – moderate inflammation (obvious number of chronic inflammatory cells without sign of necrosis); 4 – severe inflammation: (abscess formation, necrosis and presence of polymorphonuclear cells). Dentine bridge thickness was measured to be 10-μm accuracy using the Adobe Photoshop software CS (Adobe Systems Inc, San Jose, CA, USA). One way ANOVA, Kruskal–Wallis, and Mann–Whitney tests were used for data analysis.
RESULTS
The patients aged between 14–21 years, which consist of 25 female and 15 male individuals. Both types of MTA showed higher percentage of calcified bridge formation 30 days after pulp capping [Table 1]. The calcified bridge that was formed in response to pulp capping with either types of MTA showed higher consistency and less defect compared to Dycal specimens that showed higher percentage of tunnel defects and irregularity in their calcified bridge formed beneath the capping material.
Table 1.
Percent of various categories and thickness of calcified bridge at different time intervals of the study
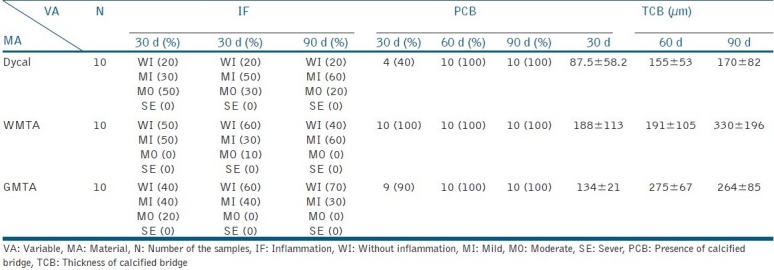
The results of this investigation have shown that both types of MTA provided thicker calcified bridge than Dycal samples at all time intervals [Table 1]. The thickness of calcified bridge in GMTA specimens was significantly greater than Dycal at 30 and 60 days (P= 0.015 and P=0.002, respectively); whereas WMTA showed significantly thicker calcified bridge than Dycal at 90 days (P=0.02) [Figures 1a–c].
Figure 1.
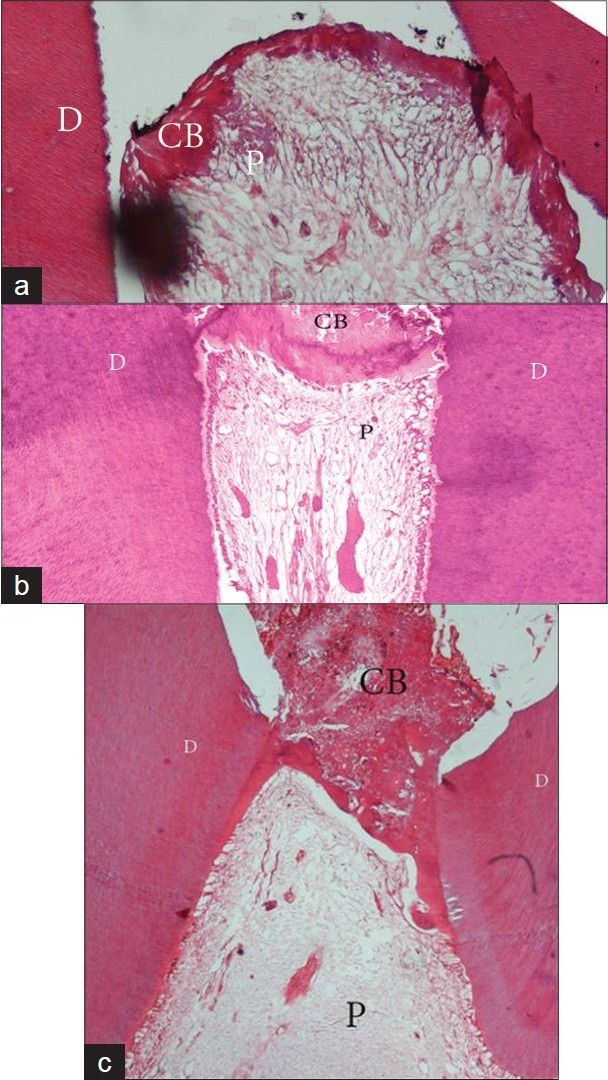
Calcified bridge formation over the capping material after 3 months. (a) Dycal, (b) WMTA, (c) GMTA. CB: Calcified bridge, D: Dentin, P: Pulp (original magnification ×10)
In addition, GMTA specimens showed significantly less inflammation compared to Dycal samples at 90 days interval (P=0.019). Most WMTA specimens and all GMTA specimens showed either free of inflammation or minor pulpal inflammation at 60 and 90 day intervals. In contrast, some Dycal specimens showed moderate inflammation even 90 days after pulp capping. GMTA specimens have shown no significant difference to WMTA in terms of the presence and thickness of calcified bridge as well as the severity of pulp inflammatory response to the either of pulp capping materials at all time intervals of the present study (P>0.05).
DISCUSSION
The results of this study have shown more favorable histologic results following pulp capping with either types of MTA in comparison to Dycal.
Previous studies on pulp capping materials have emphasized on having enough number of samples in each group to provide reasonable condition for statistical analysis.[22,28] Therefore, in the present study, the number of samples in each group was set at ten. Previously performed investigations on human teeth used five to ten teeth for each pulp capping material at every time intervals.[22,23,26,27]
Previous investigations on human teeth showed conflicting results when CH was compared with either types of WMTA or GMTA as pulp capping agents.[19,20,22,23,25–27] Some investigations showed no significant difference between MTA and CH in terms of calcified bridge formation.[20,25,27] In contrast, several others have shown superiority of MTA in comparison to CH in terms of calcified bridge formation[19,22,23,26] and pulp inflammation.[19,22,25] The results of this study was in corroboration with previous investigations that have shown both types of MTA were superior to Dycal in terms of the quality and the presence of calcified bridge[19,22,23] as well as the inflammatory response of the pulp to the capping materials.[19,22,25]
Min et al.[23] in their study on human teeth compared Dycal with MTA as pulp capping agents. The results of their study showed the presence of inflammatory cells at the pulp of some of Dycal samples after 2 months that was in corroboration with the results of the present study [Table 1].
Previous human investigations on pulp capping agents used intact maxillary and mandibular third molars or premolars that were candidate for extraction.[19,22,23,26] In this study, intact permanent mandibular and maxillary premolar teeth that were candidate for extraction because of orthodontic reasons were used. Most previous clinical trials that compared MTA and Dycal as pulp capping agents used intact teeth that might not show the real clinical condition in which the teeth have caries and pulp may have chronic or acute inflammation prior to the treatment. Ethical concerns are the major reasons that prevent investigators to pulp cap the teeth with caries. Because when histologic evaluation is going to be performed, the teeth should be extracted prior to tissue processing.
A previous animal investigation that compared WMTA and GMTA as pulp capping agents showed similar pulpal response and presence of calcified bridge at 1 and 2 weeks intervals after pulp capping.[14] Nair et al.[22] have stated that the results of animal studies are not conclusive on human teeth and therefore clinical trials should be performed on volunteers for determining clinical application of a pulp capping material. The results of this study were in corroboration with a previous animal investigation on comparing WMTA with GMTA as pulp capping agents that showed no histologic difference when pulp capped with either of the materials.[14]
The presence of inflammatory cells in pulps capped with either types of GMTA or WMTA in this study may be the result of cavity restoration with amalgam. Although excellent sealing ability of MTA has been confirmed, it may not completely prevent microleakage of the bacteria from the oral cavity.[2] Similar to the present study, several previous animal studies used amalgam as permanent restoration over MTA.[9,10,17,18]
In addition, in the current study poor quality of calcified bridge formed beneath Dycal as pulp capping material was in corroboration with the previous investigations compared Dycal with either types of GMTA or WMTA despite using various materials for coronal restorations.[19,22,23,25]
The application of the capping material at the exposure site is very important for the practitioners. MTA needs wet environment following use as pulp capping material, whereas, placing Dycal at the exposure site as hard setting calcium hydroxide agent is very difficult. Therefore, in addition to the histologic superiority of MTA as pulp capping material, the material is easier to use in comparison to Dycal for pulp capping. A previously published article confirmed this easier clinical application.[22]
In conclusion, based on the results of this study both types of GMTA and WMTA can be suggested as the material of choice for pulp capping and no significant difference was found between them in terms of calcified bridge formation and thickness as well as pulpal inflammatory response.
ACKNOWLEDGMENT
This study was financially supported by Research Committee of Kerman Medical University.
Footnotes
Source of Support: Research Committee of Kerman Medical University
Conflict of Interest: None declared.
REFERENCES
- 1.Torabinejad M, Parirokh M. Mineral Trioxide aggregate: A comprehensive literature review- Part II: Sealing ability and biocompatibility properties. J Endod. 2010;36:190–202. doi: 10.1016/j.joen.2009.09.010. [DOI] [PubMed] [Google Scholar]
- 2.Parirokh M, Torabinejad M. Mineral Trioxide aggregate: a comprehensive literature review- Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010;36:400–12. doi: 10.1016/j.joen.2009.09.009. [DOI] [PubMed] [Google Scholar]
- 3.Asgary S, Parirokh M, Eghbal M, Brink F. Chemical Differences between White and Grey Mineral Trioxide Aggregate. J Endod. 2005;31:101–3. doi: 10.1097/01.don.0000133156.85164.b2. [DOI] [PubMed] [Google Scholar]
- 4.Asgary S, Parirokh M, Eghbal MJ, Stowe S, Brink F. A Qualitative X-Ray Analysis of White and Grey Mineral Trioxide Aggregate Using Compositional Imaging. J Mater Sci Mater Med. 2006;17:187–91. doi: 10.1007/s10856-006-6823-3. [DOI] [PubMed] [Google Scholar]
- 5.Asgary S, Parirokh M, Eghbal MJ, Brink F. A Comparative Study of Mineral Trioxide Aggregate and White Portland Cements Using X-ray Analysis. Aust Endod J. 2004;30:86–9. doi: 10.1111/j.1747-4477.2004.tb00416.x. [DOI] [PubMed] [Google Scholar]
- 6.Asgary S, Shahabi S, Jafarzadeh T, Amini S, Kheirieh S. The properties of a new endodontic material. J Endod. 2008;34:990–3. doi: 10.1016/j.joen.2008.05.006. [DOI] [PubMed] [Google Scholar]
- 7.Asgary S, Eghal MJ, Parirokh M, Ghoddusi J, Kheirieh S, Brink F. Comparison of mineral trioxide aggregate's composition with Portland cements and a new endodontic cement. J Endod. 2009;35:243–50. doi: 10.1016/j.joen.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 8.Parirokh M, Torabinejad M. Mineral Trioxide aggregate: A comprehensive literature review- Part I: Chemical, Physical, and antibacterial properties. J Endod. 2010;36:16–27. doi: 10.1016/j.joen.2009.09.006. [DOI] [PubMed] [Google Scholar]
- 9.Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp capping material. J Am Dent Assoc. 1996;127:1491–4. doi: 10.14219/jada.archive.1996.0058. [DOI] [PubMed] [Google Scholar]
- 10.Faraco IM, Jr, Holland R. Response of the pulp of dogs to capping with mineral trioxide aggregate or a calcium hydroxide cement. Dent Traumatol. 2001;17:163–6. doi: 10.1034/j.1600-9657.2001.170405.x. [DOI] [PubMed] [Google Scholar]
- 11.Tziafas D, Pantelidou O, Alvanou A, Belibasakis G, Papadimitriou S. The dentinogenic effect of mineral trioxide aggregate (MTA) in short-term capping experiments. Inter Endod J. 2002;35:245–54. doi: 10.1046/j.1365-2591.2002.00471.x. [DOI] [PubMed] [Google Scholar]
- 12.Dominguez MS, Witherspoon DE, Gutmann JL, Opperman LA. Histological and scanning electron microscopy assessment of various vital pulp-therapy materials. J Endod. 2003;29:324–33. doi: 10.1097/00004770-200305000-00003. [DOI] [PubMed] [Google Scholar]
- 13.Andelin WE, Shabahang S, Wright K, Torabinejad M. Identification of hard tissue after experimental pulp capping using dentin sialoprotein (DSP) as a marker. J Endod. 2003;29:646–50. doi: 10.1097/00004770-200310000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Parirokh M, Asgary S, Eghbal MJ, Stowe S, Eslami B, Eskandari Zadeh A, et al. A Comparative Study of White and Grey Mineral Trioxide Aggregate as Pulp Capping Agent. Dent Traumatol. 2005;21:150–4. doi: 10.1111/j.1600-9657.2005.00311.x. [DOI] [PubMed] [Google Scholar]
- 15.Briso AL, Rahal V, Mestrener SR, Dezan Junior E. Biological response of pulps submitted to different capping materials. Braz Oral Res. 2006;20:219–25. doi: 10.1590/s1806-83242006000300007. [DOI] [PubMed] [Google Scholar]
- 16.Asgary S, Eghbal MJ, Parirokh M, Ghanavati F, Rahimi H. A comparative study of histologic response to different pulp capping materials and a novel endodontic cement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:609–14. doi: 10.1016/j.tripleo.2008.06.006. [DOI] [PubMed] [Google Scholar]
- 17.Hasheminia SM, Feizi G, Razavi SM, Feizianfard M, Gutknecht N, Mir M. A comparative study of three treatment methods of direct pulp capping in canine teeth of cats: A histologic evaluation. Laser Med Sci. 2010;25:9–15. doi: 10.1007/s10103-008-0584-9. [DOI] [PubMed] [Google Scholar]
- 18.Tabarsi B, Parirokh M, Eghbal MJ, Haghdoost AA, Torabzadeh H, Asgary S. A comparative study of dental pulp response to several pulpotomy agents. Inter Endod J. 2010;43:565–71. doi: 10.1111/j.1365-2591.2010.01711.x. [DOI] [PubMed] [Google Scholar]
- 19.Aeinehchi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: A preliminary report. Inter Endod J. 2003;36:225–31. doi: 10.1046/j.1365-2591.2003.00652.x. [DOI] [PubMed] [Google Scholar]
- 20.Iwamoto CE, Adachi E, Pameijer CH, Barnes D, Romberg EE, Jefferies S. Clinical and histological evaluation of white ProRoot MTA in direct pulp capping. Am J Dent. 2006;19:85–90. [PubMed] [Google Scholar]
- 21.Farsi N, Alamoudi N, Balto K, Al Mushayt A. Clinical assessment of mineral trioxide aggregate (MTA) as direct pulp capping in young permanent teeth. J Clin Ped Dent. 2006;31:72–6. doi: 10.17796/jcpd.31.2.n462281458372u64. [DOI] [PubMed] [Google Scholar]
- 22.Nair PN, Duncan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: A randomized controlled trial. Inter Endod J. 2008;41:128–50. doi: 10.1111/j.1365-2591.2007.01329.x. [DOI] [PubMed] [Google Scholar]
- 23.Min KS, Park HJ, Lee SK, Park SH, Hong CU, Kim HW, et al. Effect of mineral trioxide aggregate on dentin bridge formation and expression of dentin sialoprotein and heme oxygenase-1 in human dental pulp. J Endod. 2008;34:666–70. doi: 10.1016/j.joen.2008.03.009. [DOI] [PubMed] [Google Scholar]
- 24.Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: An observational study. J Am Dent Assoc. 2008;139:305–15. doi: 10.14219/jada.archive.2008.0160. [DOI] [PubMed] [Google Scholar]
- 25.Sawicki L, Pameijer CH, Emerich K, Adamowicz-Klepalska B. Histological evaluation of mineral trioxide aggregate and calcium hydroxide in direct pulp capping of human immature permanent teeth. Am J Dent. 2008;21:262–6. [PubMed] [Google Scholar]
- 26.Accorinte Mde L, Holland R, Reis A, Bortoluzzi MC, Murata SS, Dezan E, Jr, et al. Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth. J Endod. 2008;34:1–6. doi: 10.1016/j.joen.2007.09.012. [DOI] [PubMed] [Google Scholar]
- 27.Accorinte ML, Loguercio AD, Reis E, Carneiro E, Grande RH, Murata SS, et al. Response of human dental pulp capped with MTA and calcium hydroxide powder. Operat Dent. 2008;33:488–95. doi: 10.2341/07-143. [DOI] [PubMed] [Google Scholar]
- 28.Olsson H, Petersson K, Rohlin M. Formation of hard tissue barrier after pulp capping in humans: A systematic review. Inter Endod J. 2006;39:429–42. doi: 10.1111/j.1365-2591.2006.01116.x. [DOI] [PubMed] [Google Scholar]