

Abstract
Background:
Ultrasonography is accepted as a useful imaging modality in the early detection of developmental dysplasia of the hip (DDH). Early detection and early treatment of DDH prevents hip dislocation and related physical, social, economic, and psychological problems. The purpose of this study was to evaluate the reliability of ultrasonographic and roentgenographic measurements measured by seven different observers.
Materials and Methods:
The alpha angles of 66 hips in 33 patients were measured using the Graf method by seven different observers. Acetabular index degrees on plane roentgenograms were measured in order to assess the correlation between the ultrasonographic alpha angle and the radiographic acetabular index, which both show the bony acetabular depth, retrospectively.
Results:
The interclass correlation coefficient, measuring the interobserver reliability, was high and statistically significant for the ultrasonographic measurements. There was a negative correlation between the alpha angle and the acetabular index.
Conclusions:
Ultrasonography, when applied properly, is a reliable technique between different observers, in the diagnosis and follow up of DDH. When assessed concomitantly with the roentgenographic measurements, the results are reliable and statistically meaningful.
Keywords: Developmental dysplasia, hip, ultrasonography, acetabular index
INTRODUCTION
Developmental dysplasia of the hip (DDH) is a dynamic disease which can present in different forms at different ages and evolves over time, potentially capable of getting better or worse as the child develops.1 The disease can be managed and can be less harmful if diagnosed and treated early. Diagnosis, however, has often presented with problems.2 Late diagnosis results in complex treatment modalities with higher rates of failures and complications. It may lead to disabling osteoarthritis in adulthood.3
Physical examination helps to diagnose hip pathology, but may not always be sufficient, because of different interpretations of the examiners. Plane roentgenograms do not show the hip adequately in the first three months of life.4 Ultrasonography shows the cartilaginous and soft tissue anatomy of the hip. It is an effective and noninvasive method without radiation.4
Even from the same images, different results can be obtained due to different landmark indications depending on the observer. In this study, we aimed to measure the reliability of ultrasonographic measurements between different observers and assess the correlation between the ultrasonographically measured alpha angle and the radiologically measured acetabular index, which both show the bony acetabular depth.
MATERIALS AND METHODS
Between January 2008 and July 2008, selective ultrasonography was performed in 50 children, younger than 6 months of age, who were suspected to be at risk for DDH. These patients were selected from our outpatient clinic archive. Patients having an acceptable ultrasonographic image, containing a standard measurement plane to carry out a reproducible measurement (n = 33), were included in the study group and were numbered randomly by an Orthopedic Surgeon (C.C) who was specialized in pediatric hip ultrasonography.
We aimed to assess the reliability of the ultrasonographic measurements between different observers. Seven observers participated in the study, including five senior residents and two assistant professors in Orthopedics and Traumatology. Four of the observers (two assistant professors and two senior residents) had attended a hip ultrasonography course given by Dr. Graf and they had the basic course certificate. None of the observers knew about the patients’ profile.
The hip ultrasonography images were taken in the outpatient clinic by the Graf method with the help of a 7.5-MHz, 80-mm linear transducer (Hitachi EUB-405, Hitachi Medical Co., Japan). The images were multiplied through photocopy in good quality. None of the reprints included any informative landmarks. Each blinded observer did not know how these ultrasonograms had been interpreted by the other observers. Seven different observers measured the alpha angles on these ultrasonographic images in 66 hips of 33 patients.
According to Graf's technique, the ultrasound picture is taken laterally in a coronal plane and the coronal plane should pass through the center of the hip joint. The center of the hip joint is marked by the lower limb of the os ilium in the acetabulum. If the picture is taken in the correct plane, not directed dorsally or ventrally, some reference points must be identified such as the deepest point of the acetabulum, the lower iliac margin at the triradiate cartilage, the labrum, and the chondroosseous border of the proximal femur. To classify different hip types, Graf has introduced an angle for the bony acetabular roof or “α” (alpha) angle and another for the cartilaginous acetabular roof or “β” (beta) angle.5
To measure the alpha and beta angle, a coronal image of the hip is obtained, and three lines are constructed: a vertical line drawn parallel to the ossified lateral wall of the ilium (base line); a line drawn along the roof of the cartilaginous acetabulum, from the lateral osseous edge of the acetabulum to the center of the labrum (cartilaginous roof line); and a line drawn from the inferior edge of the osseous acetabulum (the inferior iliac margin) at the roof of the triradiate cartilage to the most lateral point on the ilium (the superior osseous rim) (bony roof line). The alpha angle is formed by the intersection of the baseline and the bony roof line. The lower limit accepted as normal for the alpha angle is 60 degrees. The alpha angle reflects the osseous coverage of the femoral head by the acetabulum; the smaller the angle, the greater the degree of dislocation. The beta angle is formed by the intersection of the baseline and the cartilaginous roof line.6,7 The ultrasonographic parameters were measured as described above. In our daily practice, we use ultrasonography in the follow-up and during treatment of DDH. We use roentgenograms after the fourth month of life in the hip dysplasia suspected patients.
The other part of our study was to assess the correlation between the ultrasonographic alpha angle and the roentgenographic acetabular index. Acetabular index in degrees was measured in 30 hips of 15 patients on anterior-posterior (AP) roentgenograms of the pelvis by these seven observers.
Fifteen of 33 patients had acceptable plane roentgenograms when they visited our clinic. These roentgenograms were taken in other clinics, and because of suspected hip dysplasia, the patients were referred to our clinic. Criteria for acceptable plane roentgenograms were as follows; radiograph taken from one meter distance, good quality radiograph having a standard measurement plane (giving the opportunity to make measurements) and an appropriate radiation dose. In 11 patients, the plane roentgenograms and the ultrasonographic images were taken on the same day. In four of them, plane roentgenograms were taken 2 days earlier.
Various lines may be drawn on a pelvic radiograph to evaluate acetabular maturity and femoral head position. Hilgenreiner's line is a horizontal line connecting the superior margins of the triradiate cartilages of both hips. The acetabular index is the angle between Hilgenreiner's line and a line drawn from the most superolateral margin of the ossified acetabulum to the superolateral margin of the triradiate cartilage. In the neonate, this angle is normally less than 30 degrees and by 2 years of age, the angle is normally less than 20 degrees.8 DDH is associated with an increased angle.9 All the observers measured the acetabular index from the pelvis AP roentgenogram of the patient without leaving any informative landmark for the other observers and saved the measurements according to the patient number. All the observers measured acetabular index with the same technique and same landmarks. The correlations between the measurements of the ultrasonographic and roentgenographic images were calculated.
Measurements were analyzed statistically using a computer program (Medcalc for Windows 11.1, Broekstraat 52B-9030 Mariakerke, Belgium). The single measure interclass correlation coefficient (and 95% confidence intervals) by choosing two-way random model and absolute agreement type (method 1) was used to evaluate interobserver reliability. According to this system, a value less than 0 indicates bad agreement, a value of 0 to 0.20 indicates slight agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, substantial agreement; and 0.81 to 1.0 indicates excellent agreement. Level of statistical significance was regarded as P<0.05. If the measurement is minus, it shows the negative correlation between the measurements.2 Correlation between acetabular index and alpha angle was analyzed by calculation of the Pearson correlation coefficient. We obtained informed consent from parents of these cases who underwent this study.
RESULTS
Our study group included 66 hips of 33 patients. The mean age of the patients was 2.19 months (range, 0.23 [7 days] to 6 months). Nineteen of the patients (57.6 %) were females and 14 (42.4%) were males. Twenty-eight (84.8%) of the patients had no family history about DDH and five (15.2%) had DDH in the family. Twenty-one (63.6%) of the infants were born with caesarian section and 12 (36.4%) were born with the normal vaginal delivery. Thirty-one (93.9%) of the infants had no abnormality during delivery and two (6.1%) had abnormalities (1 oligohydramnios, 1 meningomyelocele). Twenty-four infants (72.7%) were the first child, six (18.2%) were second, two (6.1%) were third, and one (3%) was the fourth child. Twenty-seven (81.8%) of the patients had no other congenital pathologies and six (18.2%) had pathologies (4 pes equinovarus deformity, 1 meningomyelocele, 1 hyperbilirubinemia).
On physical examination, no finding could be obtained by Barlow or Ortolani maneuver. One of the patients had minimal limited abduction and 12 (36.4%) had skin fold asymmetry. Patients suspected to be at risk of having DDH i.e. those with normal physical examination but with a positive family history of DDH or first born girl child were also included in the study.
The total number of observations were 462. Differences were observed in the measuring technique of the observers [Figure 1]. The mean alpha angle was 65.5 degrees (range, 54° to 72°).
Figure 1.
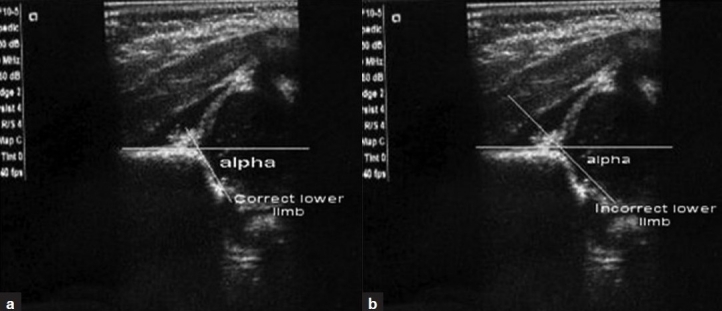
Signing the deepest point of the acetabulum differed according to the observer. (a) Some observers (4 of 7) signed the lower limb of the os ilium correctly. (b) Some observers (3 of 7) measured the ligament with the fovea centralis instead of the lower limb incorrectly
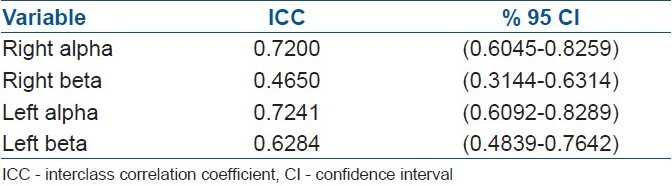
There was a moderate agreement between the observers for the right beta values, and there was a substantial agreement between the observers for the other measurements [Table 1].
Table 1.
Interclass correlation coefficient (and 95% confidence intervals) for evaluation of interobserver reliability
The mean acetabular index was 23.7° for the right hips and 24.7° for the left hips. The pearson correlation coefficient between the alpha angle and the acetabular index of the right and left hips are shown in Table 2.
Table 2.
Pearson correlation coefficient and statistical P values between the alpha values and acetabular index degrees
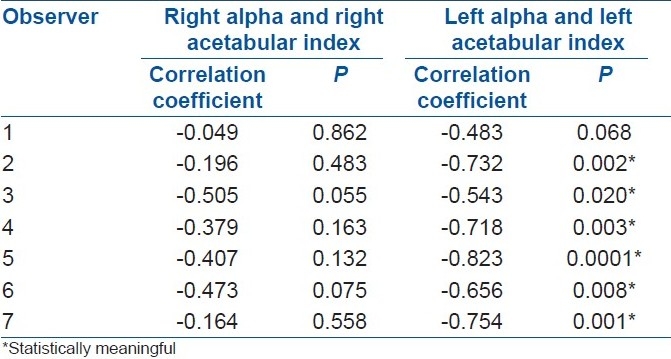
As an example, for the second observer, left acetabular alpha and left acetabular index Pearson correlation coefficient is -0.732 and P=0.002, which shows the reverse, medium powered, statistically meaningful relation.
DISCUSSION
In the screening of infants for DDH, hip ultrasonography is a frequently used method. Plain roentgenograms can give inaccurate measurements of the hip joint in the first three months of life.10 After ossification of the femoral epiphysis, roentgenographic techniques can be helpful in the detection of hip dysplasia. Determining the reliability of ultrasonographic measurements between different observers and evaluating the correlation of the ultrasonographic measurements with roentgenographic views was the scope of this study.
Having basic knowledge and making a careful examination and classification are the key points to make reliable measurements using Graf's method.2 Omeroglu et al. stated that it is usually easy to obtain a sonogram that has a standard measurement plane, but it is not always easy to assess the sonogram correctly.2
Bar-On et al.11 indicated that the technique of ultrasonographic examination and the interpretation of the image and the availability of a history and physical examination might influence the results. The variability in measurement is not an important factor and standardization is easier to be established, when ultrasonography is performed properly.7 The observer making the diagnosis plays an important role, because ultrasound screening is only reliable if the examiners are experienced.12
Different results can be obtained from the same ultrasonographic image due to different alpha values depending on the observer. There were differences in identifying the landmarks for ultrasonographic measurements in our study group. In a study reported by Boal and Schwenkter, findings of 212 sonograms of infant hips were correlated with those of radiographies, orthopedic examination, or both. There were no false-negative or false-positive results among infants with congenital hip dysplasia.13
Discrepancies between the ultrasound appearance of the bony acetabulum and the radiographic appearance indicate that there is not always an exact correlation. This may result from observer variation, tilting effect of a plane roentgenogram, and the nature of the ultrasound measurements.14
Radiographs are very dependent on proper positioning and do not show the cartilaginous components of the acetabulum and femoral head. Also, radiographs are not capable of assessing femoral head stability as they offer only a static two-dimensional image.9
Roposh et al. stated that ultrasonography scans correlated well with radiographic results in dislocated and in normal hips.15 In another study by Terjesen et al., normal and dislocated hips correlated well on ultrasonography and radiography, but dysplastic hips did not. Terjesen et al. concluded that ultrasonography was reliable in detecting hip pathology.16
Morin et al.,17 in a study of 171 infants, used ultrasonography to calculate a parameter which they called “femoral head coverage,” and compared it with the acetabular index obtained through AP roentgenogram of the pelvis in the same patients. They found a correlation between the femoral head coverage and the acetabular index.
In our study, we think that the major reason that made the difference between the observers was to find the correct landmarks for measuring the angles on an ultrasonographic image. We see two problems: the observers had problems to identify the anatomical structures [Figure 1], or they did not handle the correct definitions, e.g., the bony rim [Figure 2]. Two senior residents without certificate of Graf's method signed anatomical landmarks, especially iliac bony rim, incorrectly, according to the other experienced doctors. These changes in signing the landmark points caused the difference in measuring the alpha and beta angles. Although there was difference in measuring the angles between the observers, correlation coefficient was statistically high [Figure 3]. This may be a weakness of our study. Although measurement techniques are different, there is a high correlation, if the measurement techniques were the same, then correlation coefficient would be probably higher.
Figure 2.
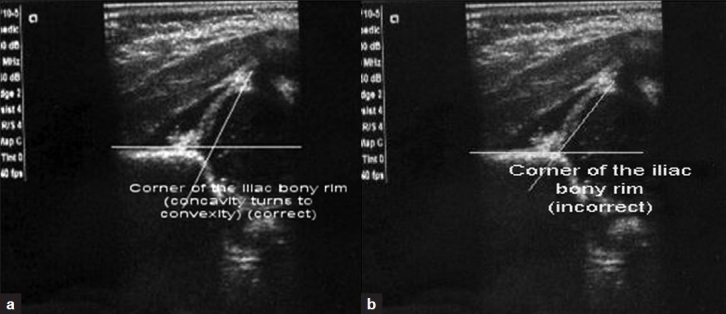
Signing the iliac bony rim differed according to the observer. (a) Some observers (3 of 7) signed the point where the concavity of the rim turns to convexity correctly. (b) Some observers (4 of 7) signed the strict corner of the iliac bony rim incorrectly
Figure 3.
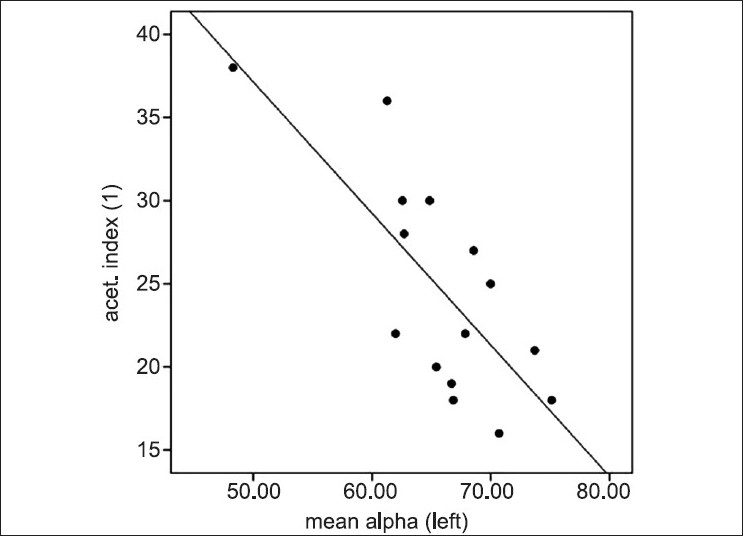
Sample for the negative correlation between the acetabular index and alpha angle. When the alpha angle increases, acetabular index degree decreases
CONCLUSIONS
Ultrasonography, as a diagnostic tool for DDH, should be applied properly. The position of the patient, the position of the probe, and signing the landmarks for measuring the angles are important factors for a reliable result. Although most of the hips in our study group were normal, this study focused on the measuring differences between the observers, in the diagnosis, and follow-up of patients suspected to be having DDH. We observed a high level of agreement in the measurement of the ultrasonographic data between different observers. Statistical meaningfulness of these measurements is encouraging and shows us the reliability of the ultrasonographic measurements between different observers.
In the assessment of the correlation between the ultrasonographic alpha values and acetabular index degrees, we observed a mismatch between the right and left side measurements. For the left hips, statistical values were meaningful, but for the right hips, correlation coefficients were statistically meaningless. This situation can be the result of observer variability or related with the plain roentgenography.
We conclude that ultrasonographic measurements are reliable, but may not always be correlated with the roentgenograms between different observers.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Herring JA. Developmental dysplasia of the hip. In: Herring JA, editor. Tachdjian's Pediatric Orthopaedics. Philadelphia, PA: Saunders Company; 2002. pp. 513–654. ch:15. [Google Scholar]
- 2.Omeroğlu H, Biçimoğlu A, Koparal S, Seber S. Assessment of variations in the measurement of hip ultrasonography by the Graf method in developmental dysplasia of the hip. J Pediatr Orthop B. 2001;10:89–95. [PubMed] [Google Scholar]
- 3.Inan M, Korkusuz F. Developmental dysplasia of the hip. Clin Orthop Relat Res. 2008;466:761–2. doi: 10.1007/s11999-008-0175-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Weinstein SL, Mubarak SJ, Wenger DR. Developmental hip dysplasia and dislocation: Part 1. J Bone Joint Surg Am. 2003;85:1824–32. [Google Scholar]
- 5.Tönnis D, Storch K, Ulbrich H. Results of newborn screening for cdh with and without sonography and correlation of risk factors. J Pediatr Orthop. 1990;10:145–52. [PubMed] [Google Scholar]
- 6.Graf R, Wilson B. Sonography of the infant hip and its therapeutic implications. London: Chapman Hall; 1995. pp. 53–65. [Google Scholar]
- 7.Wientroub S, Grill F. Current concepts review. Ultrasonography in developmental dysplasia of the hip. J Bone Joint Surg Am. 2000;82-A:1004–18. doi: 10.2106/00004623-200007000-00012. [DOI] [PubMed] [Google Scholar]
- 8.Matheney TH, Kim YJ. Hip, Pelvis, and Femur Disorders: Pediatrics. In: Fischgrund JS, editor. Orthopaedic Knowledge Update 9. Rosemont, IL: AAOS; 2008. p. 716. Ch. 59. [Google Scholar]
- 9.GE Healthcare Paediatric Hip. Developmental Dysplasia of Hip (Medcyclopaedia Web Site) [Last accessed on 2009 Jan 6]. Available from: http://www.medcyclopaedia.com/library/topics/volume_vii/d/developmental_dysplasia_of_the_hip.aspx .
- 10.Dogruel H, Atalar H, Yavuz OY, Sayli Y. Clinical examination versus ultrasonography in detecting developmental dysplasia of the hip. Int Orthop. 2008;32:415–9. doi: 10.1007/s00264-007-0333-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bar-On E, Meyer S, Harari G, Porat S. Ultrasonography of the hip in developmental hip dysplasia. J Bone Joint Surg Br. 1998;80-B:321–4. doi: 10.1302/0301-620x.80b2.8381. [DOI] [PubMed] [Google Scholar]
- 12.Treiber M, Tomazic T, Tekouc-Galob A, Zolger J, Korpar B, Burja S, et al. Ultrasound screening for developmental dysplasia of the hip in the newborn: A population based study in the Maribor region, 1997-2005. Wien Klin Wochenschr. 2008;120:31–6. doi: 10.1007/s00508-007-0922-0. [DOI] [PubMed] [Google Scholar]
- 13.Boal DK, Schwenkter EP. The infant hip: Assessment with real time US. Radiology. 1985;157:667–72. doi: 10.1148/radiology.157.3.3903853. [DOI] [PubMed] [Google Scholar]
- 14.Harcke HT. Imaging methods used for children with hip dysplasia. Clin Orthop Relat Res. 2005;434:71–7. doi: 10.1097/01.blo.0000162411.55355.c8. [DOI] [PubMed] [Google Scholar]
- 15.Roposch A, Moreau NM, Uleryk E, Doria AS. Developmental dysplasia of the hip: quality of reporting of diagnostic accuracy for US. Radiology. 2006;241:854–60. doi: 10.1148/radiol.2413051358. [DOI] [PubMed] [Google Scholar]
- 16.Terjesen T, Runden TO, Tangerud A. Ultrasonography and radiography of the hip in infants. Acta Orthop Scand. 1989;60:651–60. doi: 10.3109/17453678909149596. [DOI] [PubMed] [Google Scholar]
- 17.Morin C, Harcke HT, MacEwen GD. The infant hip:real time Us assessment of acetabular development. Radiology. 1985;157:673–7. doi: 10.1148/radiology.157.3.3903854. [DOI] [PubMed] [Google Scholar]