

Abstract
INTRODUCTION
Ankle fractures are common injuries affecting all age groups and constitute a large proportion of the orthopaedic trauma case load. Patients are usually admitted directly to the ward from the emergency department and a large number of bed-days are spent waiting for the ankle swelling to subside prior to surgery. We audited current practice and then implemented a home therapy programme (HTP). The purpose of the study was to assess the pioneering HTP with respect to cost effectiveness, length of stay and patient satisfaction.
PATIENTS AND METHODS
If HTP criteria were met, patients with reduced, unstable ankle fractures were taught safe mobilisation by physiotherapists in the emergency department. They were then discharged home to ice and elevate their ankle in a plaster backslab. A provisional operation date was allocated on discharge. They were admitted to hospital the day of surgery and then discharged home when safe and comfortable.
RESULTS
Forty-three consecutive patients met our inclusion criteria and underwent surgical fixation of unstable ankle fractures over a 3-month period (February–April 2008). The average length of hospital stay was 8 days (range, 1–18 days), 4.5 days pre-operatively and 3.5 days postoperatively. Patients were frustrated and dissatisfied with the whole process. In total, 177 patients underwent surgical fixation of unstable ankle fractures over an 11-month period (November 2008 to October 2009) and, of these, 59 met the home therapy criteria. The average length of hospital stay was 2.4 days, 1 day pre-operatively (range, 0–4 days) and 1.4 days postoperatively (range, 0–5 days). All HTP patients expressed satisfaction with the process. Over the course of the HTP, 354 bed-days were saved which equates to a saving of £81,774. The annual estimated cost saving is £90,000.
CONCLUSIONS
The home therapy programme has proved effective in reducing hospital stay both pre- and postoperatively. It is cost-effective and well received by patients.
Keywords: Ankle fractures, Cost, Satisfaction, Pathway
As clinicians, we have an obligation to review our practice and strive to provide high quality care for all. We should also endeavour to be responsible stewards of the finite resources available to the NHS. This is even more relevant in the current financial climate. Occasionally, it is possible to combine these two ideals without compromising care. This was the idea behind setting up and running a home therapy treatment programme for adult, unstable, ankle fractures. Ankle fractures are common injuries which tend to affect an active and independent adult population. Hospitalisation for a number of days is poorly tolerated by this group of patients. This was borne out by an audit undertaken at Poole General Hospital (a 789-bed district general hospital) between February and April 2008. The audit findings led to the conception and implementation of a home therapy programme (HTP).
The aim of the HTP was to reduce the overall length of hospital stay in a safe and effective manner, whilst improving patient experience.
Patients and Methods
Over a 3-month period between February and April 2008, 46 consecutive adult patients underwent surgery for unstable acute ankle fractures. The average length of hospital stay on an acute trauma ward was 8 days. The initial 4.5 days were spent waiting for the ankle swelling to resolve to a sufficiently safe level in order to allow surgery. The postoperative 3.5 days were spent recovering and learning safe mobilisation.
Patients expressed their dissatisfaction and frustration with their hospital pathway in a survey.
The HTP was initiated on 1 November 2008 in conjunction with the physiotherapy department. Data were collected prospectively over a continuous 11-month period. All adult patients (over 18 years of age) with isolated, unstable or displaced ankle fractures requiring surgery were included in the study. Patients were not suitable for HTP if they had any of the following exclusion criteria:
Neurovascular compromise, open or particularly unstable ankle fracture pattern. (These were trimalleolar ankle fractures with a posterior fragment involving more than 25% of the articular surface.)
Medically unstable.
Previous history of venous thro mbo-embolism (VTE).
Social circumstances precluded safe home discharge.
In order to meet the safe HTP discharge criteria, patients had to be:
Fit.
Independent in activities of daily living.
Able to mobilise safely, non-weight bearing.
Have sufficient provisions of food, a telephone and inside sanitation at home.
Live within 1 h of the hospital and be able to comply with instructions to elevate and ice the ankle.
After confirmation of an ankle fracture, the patients were referred to the on-call orthopaedic team via the emergency department as per the care pathway (Fig. 1). A post manipulation radiograph of the ankle in a plaster of Paris backslab was reviewed by the middle-grade surgeon. If the patient met the previously described safe discharge criteria, a senior physiotherapist discussed the study with the patient, gained consent and taught and assessed safe mobilisation. The patient was instructed on elevation technique and exercises prior to discharge home with a provisional operation date 4–6 days later. Verbal and written instructions were provided. If the patient presented outside of normal working hours, the duty orthopaedic senior house officer performed the senior physiotherapist role, having received prior training. The next morning, the senior physiotherapist resumed the lead role and would contact each HTP patient by telephone, asking a short series of questions to screen for complications. If there was any concern from the physiotherapist or patient, arrangements were made for a prompt hospital review. If no complications arose, patients were assessed in the physiotherapy department the morning of surgery to ensure that the post traumatic oedema had resolved sufficiently to allow surgery to proceed. An ankle was suitable for surgery when the skin creases had reappeared.
Figure 1.
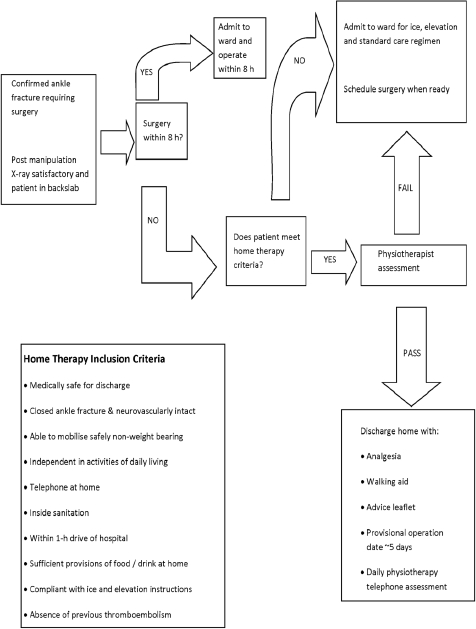
Care pathway for management of ankle fractures requiring surgical stabilisation.
HTP patients did not receive chemical thromboprophylaxis whilst awaiting surgery.
Results
Out of 177 patients, 59 were suitable for home management. No patients were excluded because of a previous history of VTE and no patients developed a VTE whilst on the programme.
The home therapy ankle fractures consisted of 22% trimalleolar fractures, 42% bimalleolar fractures and 36% with a displaced medial or lateral malleolar fracture. Figure 2 shows the reasons for exclusion from the HTP.
Figure 2.
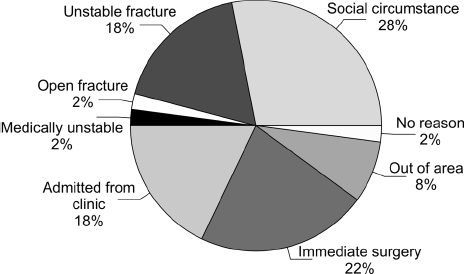
Reasons for exclusion from the home therapy programme.
The average length of time on home therapy was 6 days (range, 0–11 days). The mean pre-operative hospital length of stay was 1 day (range, 0–4 days) and the mean postoperative hospital stay was 1.4 days (range, 0–5 days). When compared with the original audit, this resulted in a saving of 354 bed-days which equated to £81,774 over the 11-month period. This was based on the cost of a trauma bed being £231 per day. This extrapolates to a predicted saving of about £90,000 per year.
The study period involved 171 h of physiotherapy time (2.9 h per patient). Patients were satisfied with their management whilst on the HTP as shown in Table 1.
Table 1.
Results of the patient satisfaction survey for the home therapy programme
| Survey question | Completely agree | Agree | Neither agree/disagree | Disagree | Completely disagree |
|---|---|---|---|---|---|
| I was provided with clear instructions about how best to use ice and elevation | 50 | 6 | 3 | 0 | 0 |
| I was clearly taught how to use crutches or a frame | 45 | 11 | 3 | 0 | 0 |
| I was shown exercises to do at home | 40 | 14 | 3 | 2 | 0 |
| I felt that the leaflet I was given contained useful information | 41 | 14 | 2 | 2 | 0 |
| I felt able to manage at home with the advice and support provided | 43 | 14 | 2 | 0 | 0 |
| I was satisfied to be discharged with advice and support and brought back for my operation | 48 | 9 | 2 | 0 | 0 |
| I was kept informed about my operation date | 40 | 15 | 4 | 0 | 0 |
| Being telephoned at home by the physiotherapist was re-assuring | 48 | 9 | 2 | 0 | 0 |
Complications
The physiotherapy telephone questions prompted three patients to be reviewed early. They all noted that they had felt their ankles move in plaster. Clinical and radiographic examination did confirm displacement of the ankle mortise. Two patients were admitted and underwent re-manipulation of the ankle and application of a new cast under general anaesthetic and X-ray control in theatre. Their scheduled operation dates were postponed by 3 days because of excessive swelling. The other patient went ahead with surgery as planned. There were no adverse outcomes from the complications.
Breach of proposed operation date
Eleven out of 59 patients did not receive their operation on the original scheduled date. All 11 cases occurred within the first 4 months of the HTP. This included two of the re-displaced fractures described above. Five patients were too swollen the morning of surgery and rescheduled for uneventful surgery 2–3 days later. Unfortunately, four patients admitted to a ward had their surgery postponed by 24 h because of more urgent trauma cases.
Discussion
The optimal management of acute ankle fractures remains surgical stabilisation within 8 h of injury. This results in the lowest rate of complications and allows early patient discharge.1–3 However, a reduction in working hours combined with an ever increasing trauma work load and a drive towards reducing ‘out-of-hours’ operating means that the 8-h goal is rarely achievable. Only 14% of the patients received their operation within 8 h. If the 8-h window is missed, the AO group recommend delaying surgery until at least day 4 post injury.4 This reduces the chance of wound complications from the post traumatic swelling. It was this majority group of patients to whom this study was targeted.
HTPs are a common occurrence in the US, where private insurance and cost are a major driving force in patient management. It is exceptionally rare to find centres in the UK that manage their ankle fractures via home therapy. It should only be considered an acceptable alternative practice if it meets with patient approval and has an acceptable complication rate. The patient survey shows that all who participated in the trial were satisfied with their overall experience of home management.
Less time in hospital pre-operatively and postoperatively meant that patients were more empowered in managing their injury and maintaining their independence from the comfort of their own home. They were more involved in the decision-making process and scheduling of their operation date. This flexibility enabled one patient to delay his operation by 11 days so as not to interfere with examinations.
The initial audit showed that the average postoperative length of stay was 3.5 days, reducing to 1.4 days on the HTP. This reduction is multifactorial. The ability of the patients to be proficient with crutch use pre-operatively played a role in the shortened stay. A combination of better postoperative pain relief and an increased awareness amongst the healthcare professionals also contributed to earlier mobilisation.
Out of 177 patients, 59 were suitable for the HTP. Figure 2 reflects the population dynamics of East Dorset. It is a popular holiday and retirement destination which accounts for the 8% of out-of-area patients and the 30% of frail patients who were unable to meet the safe discharge criteria.
There was less chance of disappointment often experienced by hospitalised patients who are sometimes starved on a ‘just-in-case’ daily basis whilst awaiting surgery. This can lead to false expectations about the timing of surgery. Patients particularly appreciated the continuity of care ensured by the daily physiotherapist telephone call. They were also comforted in the knowledge that there was always a direct point of contact should it be necessary.
The hospital trust experienced some direct and indirect advantages from the HTP. Patients were happier with their overall hospital experience and care. Allocating provisional operation dates to patients ensured a stream-lining of trauma theatre services. This, in turn, led to a more efficient and realistic booking of the operating lists resulting in fewer cancellations and over-runs.
Fewer hospitalised patients relieves pressure on finite resources by freeing healthcare professionals and beds. This, in turn, means that patients are more likely to be admitted to appropriate wards with all the benefits5 and less of a negative impact on other specialist services within the hospital.
The HTP was safely and efficiently spear-headed by the physiotherapy department with close liaison with the orthopaedic surgeons. The physiotherapists usually made contact with the patient prior to discharge from the emergency department and then daily via the telephone. The patient arrived in the physiotherapy department on the morning of surgery for a provisional ankle swelling check. If satisfactory, they were then admitted to the ward and again mobilised by the physiotherapist postoperatively. This ensured excellent continuity of care and an intelligent use of resources.
The financial savings equate to almost £90,000 per year.
There were few disadvantages with the programme. A smooth and efficient pathway was ensured only after all of the services involved had been appropriately educated. The study period required an extra 2.9 h of physiotherapy time per patient. This was absorbed within the redundant capacity of the physiotherapy department at no extra financial cost.
There were no adverse outcomes for any of the patients. They all received their surgery in a timely and efficient manner. Only three patients experienced complications. These were bimalleolar fractures which re-displaced in plaster. This complication can occur independently of HTP. There were no concerns or complications reported in retrospect.
On reviewing the initial 4 month's data, it was apparent that almost half of the patients (11 of 23) were being allocated an inaccurate provisional operation date. Closer liaison with the admissions personnel ensured that this teething problem was resolved. There were four patients who were postponed due to more urgent cases. It is inevitable when dealing with an unpredictable, acute surgical intake that exceptional circumstances will occur.
Conclusions
Home management reduces in-patient hospital length of stay and is a cost-effective alternative to the traditional hospital management of selected patients with acute, unstable, isolated ankle fractures. It is also the preferred option of the patients.
We still advocate that acute ankle fractures should be operated on within 8 h of injury. However, for the majority of patients this is rarely achievable and home management offers the ideal combination of cost effectiveness and quality care.
As a result of this study, our hospital continues to offer HTP for acute ankle fractures and we would encourage other trusts to consider the virtues.
References
- 1.Hoiness P, Stomsoe K. The influence of the timing of surgery on soft tissue complications and hospital stay. Ann Chir Gynaecol. 2000;89:6–9. [PubMed] [Google Scholar]
- 2.Carrage E, Csongradi J, Bleck E. Early complications in the operative treatment of ankle fractures. J Bone Joint Surg Br. 1991;73:79–82. doi: 10.1302/0301-620X.73B1.1991782. [DOI] [PubMed] [Google Scholar]
- 3.Konrath G, Karges D, Watson JT, Moed BR, Cramer K. Early versus delayed treatment of severe ankle fractures: a comparison of results. J Orthop Trauma. 1995;9:377–80. doi: 10.1097/00005131-199505000-00003. [DOI] [PubMed] [Google Scholar]
- 4.Muller M, Allgover M, Schneider R, Willengger H. Manual of Internal Fixation. Berlin: Springer; 1992. p. 600. [Google Scholar]
- 5.Lloyd JM, Elsayed S, Majeed A, Kadambande S, Lewis D, et al. The practice of out-lying patients is dangerous: a multicentre comparison study of nursing care provided for trauma patients. Injury. 2005;36:710–3. doi: 10.1016/j.injury.2004.11.006. [DOI] [PubMed] [Google Scholar]