

Editor
We report the case of a transverse-sigmoid colon knot, a rare cause of large bowel obstruction. There have been no previous documented reports of a transverse-sigmoid colon knot in the literature. Early surgical exploration in this case prevented progression to strangulation of the bowel and gangrene, which avoided the need for resection.
Fig 1.

Coronal CT image showing dilated large bowel loops loaded with faeces.
Case Report
A 63year old lady was admitted to hospital with a 3day history of lower abdominal pain and obstipation. On examination, she demonstrated a distended tender abdomen. Digital examination revealed faecal impaction of the rectum. Blood investigations were normal and abdominal X-ray revealed dilated large bowel loops with some faecal loading. Initially managed conservatively, she proceeded for a CT abdomen and pelvis to ascertain the cause of obstruction. This revealed a very convoluted and faecally loaded large bowel, with two apparent areas of volvulus involving the mid-transverse and sigmoid colon. There was no evidence of free fluid or free air. Without clinical improvement, she proceeded to an exploratory laparotomy which revealed a long and redundant sigmoid colon found to be looping around a very mobile and redundant transverse colon. The caecum, distal transverse and proximal sigmoid colon were grossly distended and loaded with faeces. The entire large bowel was carefully untwisted to relieve the apparent knot and all involved loops appeared congested but viable. No resection of bowel was required. The sigmoid colon and mobile left and right colon were fixed with Vicryl to the abdominal wall. A caecostomy was formed to allow the colon to remain decompressed. Post-operatively, the patient made an unremarkable recovery.
Fig 2.
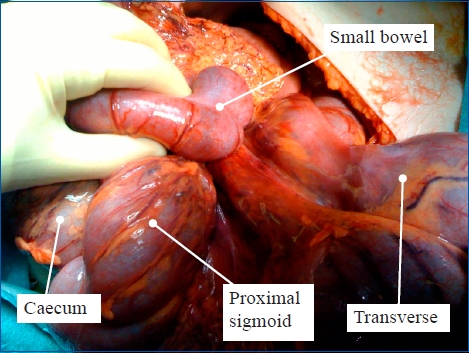
Photograph taken from theatre showing a grossly distended caecum, distal transverse and proximal sigmoid colon as a result of a transverse-sigmoid colon knot.
Discussion
The aetiology for intestinal knotting is unclear. It is likely that the knot is initiated by a hyperactive bowel which winds itself around the pedicle of a passive segment of bowel.1 On presentation, patients complain of abdominal pain and symptoms suggestive of intestinal obstruction.2 Preoperative diagnosis is extremely difficult due to the rarity of its occurrence and atypical radiological findings.2 As an advantage over the plain abdominal X-ray in diagnosing ileosigmoid knotting, computed tomography (CT) can identify medial deviation of the distal descending bowel with a pointed appearance of its medial border.3 Transverse-sigmoid knotting, however, does not appear to have such characteristic findings on CT imaging.4
Closed proximal loops become congested and gangrenous within a few hours. Therefore, aggressive resuscitation, early surgical relief of obstruction and appropriate antibiotic cover followed by exploratory laparotomy are indicated.3 Usually the knot is tight and so untwisting the knot following deflation of the bowel is only possible when bowel loops remain viable. When friable, there is risk of perforation and septic shock and in such cases en-bloc resection of the gangrenous loops within the knot is highly recommended.
Conclusion
Intestinal knotting is a rare cause of bowel obstruction and despite reports in the literature that describe the clinical features and radiological appearances, diagnosis remains difficult. This report highlights to surgeons that in rarer cases of obstruction, where a clear diagnosis is not given and when conservative measures appear to be failing, prompt surgical intervention can work to reduce complications.
The authors would like to thank their colleagues in the Radiology Department at Altnagelvin Area Hospital for their assistance in preparation of this article.
The authors have no conflict of interest.
REFERENCES
- 1.Dorai CRT. Ileosigmoid knot- case report. Singapore Med J. 1988;29(4):413–5. [PubMed] [Google Scholar]
- 2.Lee SH, Park YH, Won YS. The ileosigmoid knot: CT findings. AJR Am J Roentgenol. 2000;174(3):685–7. doi: 10.2214/ajr.174.3.1740685. [DOI] [PubMed] [Google Scholar]
- 3.Mallick IH, Winslet MC. Ileosigmoid knotting. Colorectal Dis. 2004;6(4):220–5. doi: 10.1111/j.1463-1318.2004.00361.x. [DOI] [PubMed] [Google Scholar]
- 4.Shaff MI, Himmelfarb E, Sacks GA, Burks DD, Kulharni MV. The whirl sign: a CT finding in volvulus of the large bowel. J Comput Assist Tomogr. 1985;9(2):410. [PubMed] [Google Scholar]