

We report a case of baby who had an unusual cause for absent femoral pulses. A term, male infant presented after normal pregnancy and delivery with absent femoral pulses on routine newborn examination. Four-limb blood pressure measurement showed a difference of 30 mmHg in systolic pressures between upper and lower limbs. The initial echocardiogram suggested a diagnosis of aortic coarctation, but further assessment by a cardiologist showed a thrombus at the aortic isthmus with small collaterals and a persistent ductus arteriosus supplying the descending aorta. Cerebral ultrasonography showed gross abnormality of left middle cerebral artery (LMCA) territory raising the possibility of cerebral infarction. There was no improvement with prostaglandin E2 or streptokinase. Magnetic resonance imaging showed cystic encephalomalacia of LMCA territory, suggesting prenatal insult, and confirmed complete obstruction of the aortic lumen. He underwent thrombectomy with subclavian flap augmentation of the aorta on day 7 of life and had an uneventful postoperative recovery, but unfortunately still suffers from a dense right hemiparesis and seizures and now has evolving cerebral palsy. A thrombophilia screen was negative.
Fig 1.

MRI scan of the brain showing extensive encephalomalacia in the left cerebral hemisphere
Fig 2.
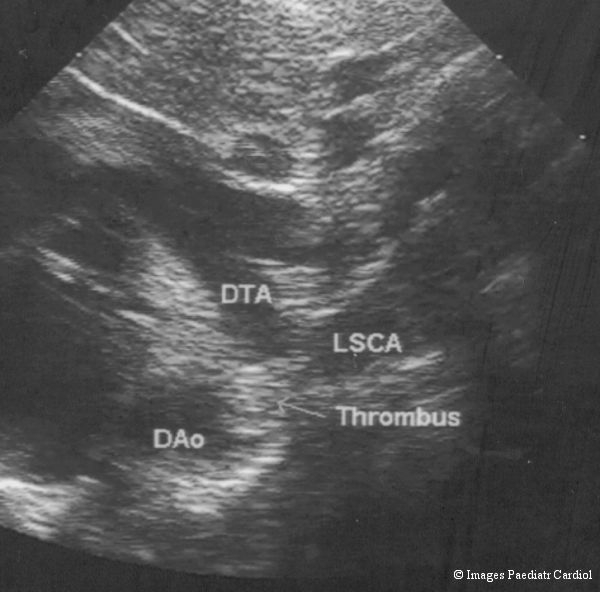
Echocardiogram – Supra-sternal view showing an organised thrombus in the Distal Transverse Aortic Arch (DTA: Distal transverse arch; Dao: Descending aorta; LSCA: Left subclavian artery)
Fig 3.

MRI scan of the aorta showing thrombus in the arch. The appearance of the arch mimics coarctation of the aorta.
Discussion
Causes of absent or reduced femoral pulses in neonatal period amongst others include coarctation of the aorta and bilateral dislocation of the hips. Aortic thrombosis can simulate aortic coarctation and can be potentially life threatening with significant morbidity1,2. Aortic thrombus is not uncommonly associated with umbilical arterial cannulation in the neonatal intensive care setting3. De novo neonatal aortic obstruction due to thrombus is rare. In this case we hypothesise that a thrombus embolised into the systemic circulation at around 22-24 weeks of gestation (based on the MRI findings). The aortic isthmus, lying between the left subclavian artery and ductus arteriosus, is the narrowest part of the aorta and obstruction at this point mimics aortic coarctation or interruption. The fact that the thrombus was well-organised and collateral vessels had developed confirmed its chronic nature.
Acknowledgments
Dr Andrew Wood, Consultant Radiologist, University Hospital of Wales, Cardiff, UK
References
- 1.de Godoy JM, De Marchi CH, Silva MG, Carvalho MC, Moscardini A, Medeiros JC. Thrombosis of the abdominal aorta in a newborn: case report and review of literature. J Pediatr Surg. 2003;38(4):E11. doi: 10.1053/jpsu.2003.50149. [DOI] [PubMed] [Google Scholar]
- 2.Rodriguez M, Sosenko I. Catheter-induced aortic thrombus masquerading as coarctation of the aorta. Clin Pediatr. 1989;28:581–584. doi: 10.1177/000992288902801207. [DOI] [PubMed] [Google Scholar]
- 3.Das BB, Sahoo S, Ivy DD. Neonatal aortic arch thrombosis masquerading as coarctation of the aorta. Pediatr Cardiol. 2004;25:80–83. doi: 10.1007/s00246-003-0571-7. [DOI] [PubMed] [Google Scholar]