

Abstract
Aim:
To determine the incidence of clinically unrecognized critical congenital heart disease (CCHD) in the newborns by using pulse oximetric screening.
Methods:
Pulse oximetry was performed on clinically normal newborns at 24-48 hours of age. If screening oxygen saturation (SpO2) was below 95%, echocardiography was then performed. Data regarding true and false positives as well as negatives were collected and analyzed.
Results:
Pulse-oximetric screening was performed on 1847 clinically normal newborns. Low SpO2 (<95%) was found in three babies two of them had CCHD, including one with transposition of the great vessels, one with complete atrioventricular canal with moderate tricuspid regurgitation (sensitivity: 100%; specificity: 99.8%; positive predictive value: 100%; negative predictive value: 100%; accuracy: 99.8%).
Conclusions:
In addition to routine physical examination in the newborn infants pulse oximetry may improve the early diagnosis CCHD in the newborn. If oxygen saturation in clinically normal newborns is below 95% at 24-48 hours of age, referral to a cardiology unit is suggested.
MeSH: Heart Defects, Infant, Newborn, Neonatal Screening/*methods, Congenital/complications/*diagnosis Oximetry
Introduction
The incidence of congenital heart diseases (CHD) is 8-10 per 1,000 live births.1,2,3,4,5 Early diagnosis of CHD is important because the delayed diagnosis of severe CHD can lead to cardiac failure, cardiovascular collapse and even death. Many infants died without the diagnosis of CHD.6 Routine neonatal examinations fails to detect more than 50% of infants with CHD.7,8,9,10,11 Many neonates with CHD have no signs that can be detected by clinical examination. Critical congenital heart diseases (CCHD) in the newborn may have borderline low oxygen saturations unrecognized clinically. This fact has led some to explore the possibility of screening all newborn babies with pulse oxygen oximetry in addition to the usual routine physical examination.12,13,14 In developing countries with inadequate medical personnel, this method can be very helpful in early detection of CCHD. Our study is designed to determine the incidence of clinically unrecognized CCHD by using pulse oximetric screening.
Methods
All infants born aged 24-48 hours at Synphaet Hospital during September 2004 to September 2006 were clinically evaluated. Only clinically normal newborns were included in the study. Exclusion criteria were any of the following abnormalities on physical examination: cyanosis, tachypnea, grunting, nasal flaring, chest retraction, significant heart murmur, active precordium, and diminished pulse. Pulse oximetry was performed using the Masimo Set pulse oximeter model Radical. Measurements were performed by the nurses on the right hand and one foot. O2 saturation (SpO2) below 95% underwent additional evaluation by echocardiography. CCHD was defined as a lesion that would likely require surgical correction during the first few months of life.
Results
During the study period there were 1,881 live born infants at Synphaet Hospital. Twenty-six neonates who met the exclusion criteria were excluded. Eight of these neonates had CHD (Figure 1).
Figure 1.
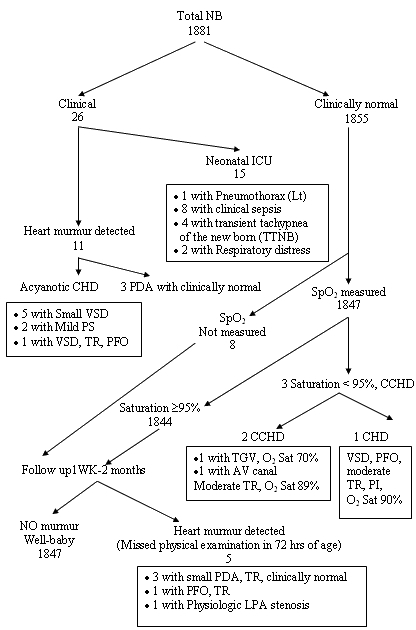
Lists of patients, type of CCHD, and method of detection
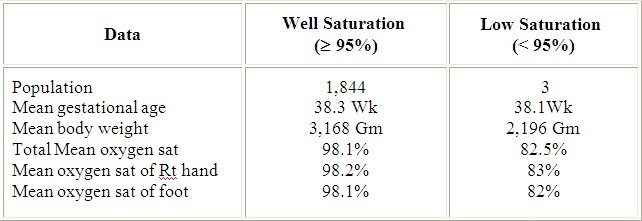
There were 8 neonates no SpO2 measurement. All of them were well on our well baby follow up record. Oximetry screening was performed on 1,847 clinically normal born infants. There were three infants with SpO2 below 95%. Two of them had CCHD, including one patient with transposition of the great vessels (TGV), one patient with complete atrioventricular canal (AV canal) & moderate tricuspid regurgitation (TR). The mean O2 saturation of normal newborns (SpO2 ≥ 95%) was 98.1% and was 82.5% in the low SpO2 group (Table 1).
Table 1.
Comparision of Results of Pulse Oximetry Screening between well Saturation (≥95%) and low Saturation (<95%) groups
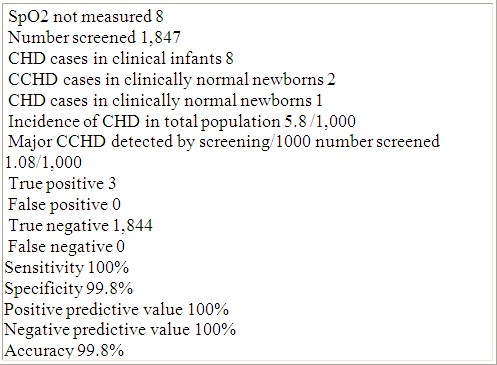
There were 11 infants with congenital heart disease in this group of infant during this study period, the incidence of CHD was 5.8 per 1000 live births and CCHD was 1.08 per 1000. A pulse oximetry cut-off value of below 95% showed 100% sensitivity, 99.8% specificity, 100% positive predictive value, 100% negative predictive value and accuracy of 99.8% in identifying CCHD (Table 2).
Table 2.
Results of Pulse Oximetry Screening for CCHD. Synphaet Hospital
Discussion
The reported incidence of CHD was 8-10 per 1000 live births.1,2,3,4,5 The incidence CCHD is agreeable with the previous study.13 To determine the sensitivity, specificity, predictive value, and accuracy of a program of pulse oximetry screening in asymptomatic newborns for CCHD , the previous study reported of the effectiveness of pulse oximetry screening for CHD in asymptomatic newborns (Sensitivity: 60%; specificity: 99.95%; positive predictive value: 75%; negative predictive value: 99.98%; accuracy: 99.97%).13 The low sensitivity in this study was because they had included non critical CHD in their calculation. However, other study revealed that systematic screening for CCHD with high accuracy required a new generation oximeter, and comparison of saturation values from the right hand and one foot substantially improves the detection of CCHD (Sensitivity: 98.5%; specificity: 96.0%; positive predictive value: 89.0%; negative predictive value: 99.5%).15 Our efficacy data is very closed to the number of other study.15 The cost of pulse oximetry screening is minimal. Although the same disposable probe was used on multiple cases, alcohols cleaning between cases were emphasized and yet no evidence of infection was found. One limitation of the study is that the number of screened neonates are too small and no case of coarctation of aorta to validate the difference of oxygen saturation in the right arm and leg.
Conclusion
This study demonstrated the use of noninvasive, cost-effectiveness tool which is pulse oximetry screening adjunct to routine neonatal examination for detecting CCHD in clinically normal newborns that were born at Synphaet Hospital during 24 months period.
References
- 1.Aroonsodsai A, Pongpanich B. The incidence of congenital heart disease born at Ramathibodi Hosp. Mahidol University Annual Research Abstract. 1993 [Google Scholar]
- 2.Payne RM, Johnson MC, Grant JW, Strauss AW. Toward a molecular understanding of congenital heart disease. Circulation. 1995;91:494–504. doi: 10.1161/01.cir.91.2.494. [DOI] [PubMed] [Google Scholar]
- 3.Ainsworth SB, Wyllie JP, Wren C. Prevalence and clinical significance of cardiac murmurs in neonates. Arch Dis Child Fetal Neonatal. 1999;80:43–45. doi: 10.1136/fn.80.1.f43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wren C, Richmond S, Donaldson L. Presentation of congenital heart disease in Infancy: implications for routine examination. Arch Dis Child Fetal Neonatal. 1999;80:49–53. doi: 10.1136/fn.80.1.f49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Richmond S, Wren C. Early diagnosis of congenital heart disease. Semin Neonatal. 2001;6:27–35. doi: 10.1053/siny.2000.0028. [DOI] [PubMed] [Google Scholar]
- 6.Kuehl KS, Loffredo CA, Ferencz C. Failure to diagnose congenital heart disease in infancy. Pediatrics. 1999;103:743–747. doi: 10.1542/peds.103.4.743. [DOI] [PubMed] [Google Scholar]
- 7.Cartlidge PH. Routine discharge examination of babies: is it necessary? Arch Dis Child. 1992;67:1421–1422. doi: 10.1136/adc.67.12.1421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abu Harb M, Hey E, Wren C. Death in infancy from unrecognized congenital heart disease. Arch Dis Child. 1994;71:3–7. doi: 10.1136/adc.71.1.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Abu Harb M, Wyllie J, Hey E, Richmond S, Wren C. Presentation of obstructive left heart malformation in infancy. Arch Dis Child Fetal Neonatal. 1994;76:179–83. doi: 10.1136/fn.71.3.f179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ainsworth SB, Wyllie JP, Wren C. Prevalence and clinical significance of cardiac murmurs in neonates. Arch Dis Child Fetal Neonatal. 1999;80:43–45. doi: 10.1136/fn.80.1.f43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wren C, Richmond S, Donaldson L. Presentation of congenital heart disease in infancy: implications for routine examination. Arch Dis Child Fetal Neonatal. 1999;80:49–53. doi: 10.1136/fn.80.1.f49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Richmond S, Reay G, Abu Harb M. Routine pulse oximetry in the asymptomatic newborn. Arch Dis Child Fetal Neonatal. 2002;87:83–88. doi: 10.1136/fn.87.2.F83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Koppel RI, Druschel CM, Carter T, Goldberg BE, Mehta PN, Talwar R, Bierman FZ. Effectiveness of pulse oximetry screening for congenital heart disease in asymptomatic newborns. Pediatrics. 2003;111:451–455. doi: 10.1542/peds.111.3.451. [DOI] [PubMed] [Google Scholar]
- 14.Arlettaz R, Bauschatz AS, Mönkhoff M, Essers B, Bauersfeld U. The contribution of pulse oximetry to the early detection of congenital heart disease in newborns. Eur J Pediatr. 2006;165:94–98. doi: 10.1007/s00431-005-0006-y. [DOI] [PubMed] [Google Scholar]
- 15.de Wahl Granelli A, Mellander M, Sunnegardh J, Sandberg K, Ostman-Smith I. Screening for duct-dependant congenital heart disease with pulse oximetry : a critical evaluation of strategies to maximize sensitivity. Acta Pediatric. 2005;94:1590–1596. doi: 10.1111/j.1651-2227.2005.tb01834.x. [DOI] [PubMed] [Google Scholar]