

Abstract
The Glissonean pedicle approach in liver surgery provides new knowledge of the surgical anatomy of the liver and advances the technique of liver surgery. The Glissonean pedicles are wrapped by a connective tissue referred to as the Glisson’s capsule and include the hepatic artery, portal vein and bile duct. The Glissonean pedicles can be approached intrahepatically or extrahepatically. The extrahepatic approach at the hepatic hilus was referred to as the extra-fascial access by Couinaud. In summary, the secondary Glissonean pedicles are encircled and ligated at the hepatic hilus without liver dissection. The angle of approach should be over the hilar plate so that the surgeon does not have to consider any variations in the arteries or bile ducts. The tertiary branches can be approached through the hepatic hilus extrahepatically or intrahepatically on the border between the sections which are fed by the secondary Glissonean pedicles. This procedure is suitable for liver cancer without hilar invasion, particularly for hepatocellular carcinoma (HCC). Patients with HCC usually have liver dysfunction and HCC easily invades the peripheral portal vein; therefore, patients with HCC should only undergo small anatomical hepatectomies such as sectionectomy or segmentectomy. Any anatomical hepatectomy can be performed using this technique which allows simple, safe and easy liver resection. Liver surgeons should, therefore, know the fundamental concept of the Glissonean pedicle transection method.
Electronic supplementary material
The online version of this article (doi:10.1007/s00534-011-0443-0) contains supplementary material, which is available to authorized users.
Keywords: Anatomical hepatectomy, Surgical anatomy of the liver, Hepatic lobectomy, Hepatocellular carcinoma, Anterior approach
Introduction
Liver surgical techniques have advanced considerably with increased knowledge of the surgical anatomy of the liver. Partial liver resection and non-anatomical liver resection were common before 1950; however, Lortat-Jacob and Robert [1] and Honjo and Araki [2] performed anatomical right hepatectomy with dissection of the hepatic artery, portal vein and bile duct in the hepatoduodenal ligament around 1950 [3]. This procedure has been referred to as a controlled hepatectomy method. By contrast, Lin et al. [4] and Tung and Quang [5] initially dissected the liver parenchyma and then approached and ligated the portal pedicles intrahepatically. These two procedures of right hepatectomy were recognized as the basic anatomical liver resection techniques [6].
The Glissonean pedicle approach at the hepatic hilus was reported by Takasaki et al. in 1986 [7]. Couinaud [8] had also previously described a simplified left hepatectomy with the Glissonean pedicle approach at the hepatic hilus similar to Takasaki’s procedure in 1985. The approaches of Couinaud and Takasaki et al. to the Glissonean pedicles are extrahepatic approaches without liver dissection, and are completely different from those of Lin et al. [4] and Tung and Quang [5]. Launois and Jamieson [9] described the intrahepatic Glissonean pedicle approach to liver resection in 1992. This new Glissonean pedicle approach has provided in-depth knowledge of the surgical anatomy of the liver and has made different types of hepatectomy possible including not only hemihepatectomy but also small anatomical hepatectomies, such as sectionectomy and Couinaud’s segmentectomy in a cirrhotic liver.
In this section, we will describe the surgical anatomy of the liver and the surgical technique that surgeons must know to be able to apply Takasaki’s Glissonean pedicle transection method.
The Glisson’s capsule and the hilar plate
Couinaud [10] referred to the vasculo-biliary sheath as the most important structure of the liver in his book entitled Surgical Anatomy of the Liver Revisited. This sheath was discovered by Johannis Walaeus in 1640. Francis Glisson published his book entitled Anatomia Hepatis in 1654 and accurately portrayed the essential anatomy of the major vessels of the liver. In his book entitled Introduction to Hepatic Surgery, Henry Gans [11] stated that there is no explanation for the remarkable fact that only Glisson’s name has been preserved in connection with the hepatic capsule. The Glisson’s capsule wraps the portal vein, hepatic artery and bile duct and these three structures are therefore regarded as forming one morphological system, which since then has been referred to as the Glissonean system [11]. The hepatic vein system is another system in the liver. Specifically, the Glisson’s capsule connects to the capsule of the liver and the hepatoduodenal ligament. The Glisson’s capsule forms a thick plate at the inferior part of the liver, which is referred to as the hilar plate. The hilar plate connects to the cystic plate, umbilical plate and Arantian plate. The hilar plate can be detached from the quadrate lobe because no branch originates from along the anterior margin or the upper surface of the hilar plate [10]. The small caudate branches originate from along the posterior margin of the hilar plate. When the hilar plate is pulled down after detaching the liver parenchyma of the quadrate lobe, the right and left Glissonean pedicles can be easily approached [10].
The Glissonean pedicles enter the liver wrapped in the Glisson’s capsule which forms one ductular system. The most important point is that any variation, particularly in the arteries and bile ducts, occurs under the hilar plate. Therefore, dissection under the hilar plate is difficult and unsafe. The elements of the segmental or sectional pedicle must supply the segment or section into which the pedicles enter. There is no need to consider any injury to the elements that supply the remaining liver segments when the pedicles above the hilar plate are interrupted [10].
Ramifications of the Glissonean pedicle and liver anatomical classification
The classification of liver anatomy and resections was defined in the International Hepato-Pancreatico-Biliary Association (IHPBA) Brisbane 2000 terminology and was reviewed by Strasberg in 2005 [12]. The second-order division of the classification in the IHPBA Brisbane 2000 terminology is based on the ramification of the hepatic artery and bile duct. On the other hand, the classification according to the Glissonean pedicles is different from that according to the IHPBA Brisbane 2000 terminology (Table 1). Specifically, the secondary Glissonean pedicles divide into 3 branches at the hepatic hilus. These pedicles can be approached extrahepatically without liver dissection. Therefore, the liver can be divided into 3 segments according to the ramification of the secondary Glissonean pedicles (Fig. 1). This classification is called Takasaki’s classification [13–15]. By comparison, the left segment in Takasaki’s classification corresponds to the left medial and left lateral sections in the Brisbane 2000 system. In Takasaki’s segmentations, there are hepatic veins between segments. For example, the middle hepatic vein is located between the left and middle segments, and the right hepatic vein is found between the middle and right segments.
Table 1.
Comparison of classification systems of liver anatomy and resection
| Healey | Couinaud | Takasaki | Brisbane 2000 system |
|---|---|---|---|
| Right lobe | Right liver | Right liver | |
| Posterior segment | Right lateral sector | Right segment | Right posterior section |
| (S6S7) | (S6S7) | (S6S7) | (S6S7) |
| Anterior segment | Right paramedian sector | Middle segment | Right anterior section |
| (S5S8) | (S5S8) | (S5S8) | (S5S8) |
| Left lobe | Left liver | Left liver | |
| Medial segment | Left paramedian sector | Left segment | Left medial section |
| (S4) | (S3S4) | (S2S3S4) | (S4) |
| Lateral segment | Left lateral sector | Left lateral section | |
| (S2S3) | (S2) | (S2S3) | |
| Caudate lobe | Caudate lobe | Caudate area | Segment 1 |
| (S1) | (S1) | (S1) | (S1) |
S Couinaud’s segment
Fig. 1.
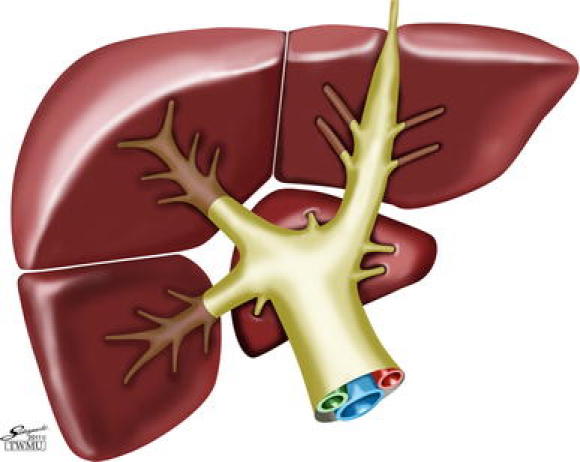
The liver is divided into 3 segments and a caudate area according to the ramification of the Glissonean pedicles
Operative techniques
Extra-fascial approach to the secondary Glissonean pedicles at the hepatic hilus
Couinaud [10] described three approaches to the hepatic hilus in his book entitled Surgical Anatomy of the Liver Revisited. Conventional dissection in the hepatoduodenal ligament is referred to as the intra-fascial approach. This procedure has also been referred to as a controlled hepatectomy method. In this approach, dissection is performed under the hilar plate, making this procedure unsafe, and surgeons have to consider variations in the hepatic artery and bile ducts. In the extra-fascial approach, the Glissonean pedicles can be dissected from the liver parenchyma extrahepatically at the hepatic hilus. The main portal fissure or left supra-hepatic fissure is opened after dissecting the liver parenchyma and surgeons must confirm the pedicles that arise from the hilar plate or umbilical plate. This procedure is referred to as the extra-fascial and transfissural approach introduced by Lin et al. [4] and Tung and Quang [5].
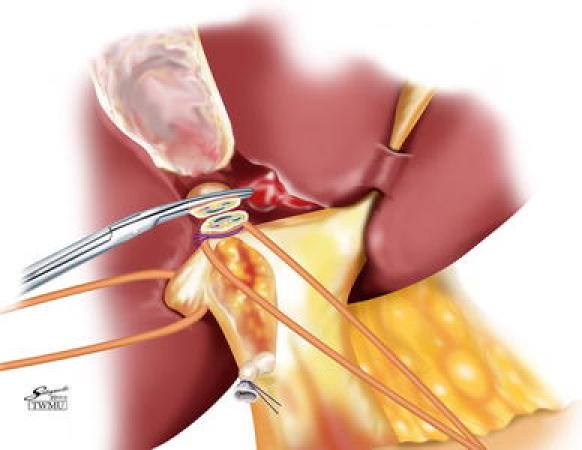
After cholecystectomy, the cystic plate is dissected. Behind the cystic plate, the right anterior Glissonean pedicle can be recognized. The hilar plate is detached from the liver parenchyma and the right anterior Glissonean pedicle is approached carefully. The right anterior pedicle is dissected completely around the pedicle and the posterior surface of the pedicle should be confirmed (Fig. 2). The pedicle is then taped and clamped to confirm the area that is fed by the pedicle. The right posterior pedicle can be taped after the right main pedicle is taped. Thereafter, the tape is pulled at the ramification point between the right anterior pedicle and the right posterior pedicle (Fig. 3). During the pedicle clamping, the color of the area changes and tumor location is confirmed by ultrasonography. When the pedicle is ligated, the tape should be extracted strongly and the pedicle near the liver parenchyma must be ligated to avoid injuring the elements that enter another section. The pedicle should be double ligated by transfixing the suture to avoid slippage of the ligated string from the pedicle stump (Fig. 4). The pedicle can be dissected before liver dissection or, after obtaining a good surgical view, during liver dissection (Fig. 5).
Fig. 2.
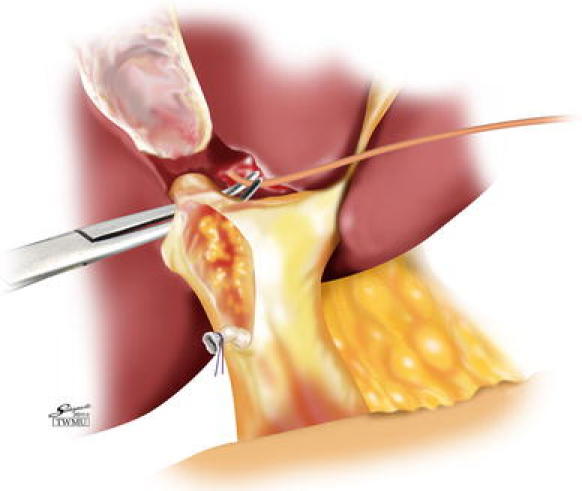
The hilar plate is detached from the quadrate lobe. The right anterior Glissonean pedicle is taped without liver dissection
Fig. 3.
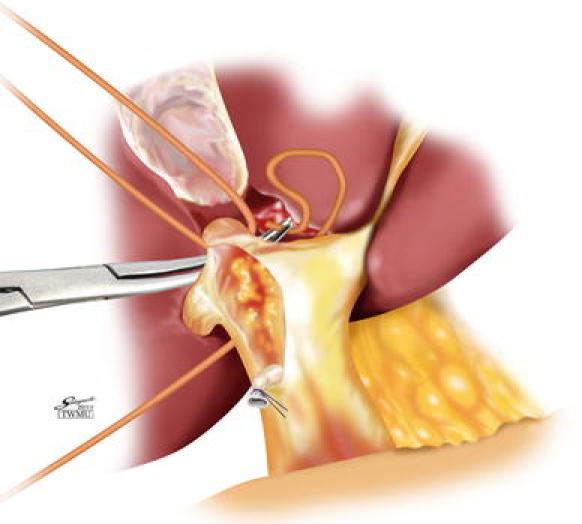
The right posterior pedicle can be taped after the right main pedicle is taped
Fig. 4.
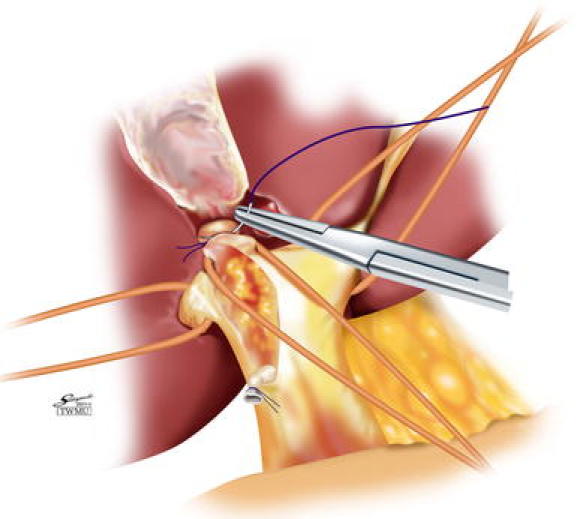
The pedicle should be double ligated by transfixing the suture to avoid slippage of the ligated string from the pedicle stump
Fig. 5.
The pedicle can be dissected before liver dissection or, after obtaining a good surgical view, during liver dissection
The left pedicle can be approached at the left end of the hilar plate (Fig. 6). This approach was described by Couinaud in 1985 [8]. In brief, the hilar plate is detached from the liver parenchyma. Then, the Arantius duct is confirmed and the left pedicle is dissected along the left pedicle at the ventral side of the Arantius duct. The lesser omentum is not necessarily divided. The tertiary branch of the caudate lobe and the right posterior bile duct branch from the left hepatic duct at the dorsal side of Arantius’ duct. Therefore, surgeons do not have to consider any variations of the hepatic bile duct.
Fig. 6.

The left pedicle can be approached at the left end of the hilar plate
After dissection around the pedicle, the pedicle is encircled and clamped. The left pedicle is divided following the same procedure of the right side pedicle transection. However, the left pedicle is the thickest of the pedicles and therefore requires careful transection. A stapler is occasionally useful for transecting the left pedicle.
How to approach the tertiary branches
One secondary Glissonean pedicle has 6–8 tertiary branches. The territory of a single tertiary branch does not correspond to Couinaud’s segment [10]. We therefore refer to the area fed by 1 tertiary branch as a cone unit of the liver [13–15] (Fig. 7). Couinaud’s segments consist of 3 or 4 cone units. The tertiary branches in the left liver can easily be approached because they can be observed along the umbilical portion without liver dissection. However, in the right liver, the tertiary branches cannot be observed at the hepatic hilus. We should therefore clamp the pedicle of the right anterior section at the hepatic hilus and confirm the border between the sections. The tertiary branches close to the hepatic hilus can be approached around the secondary pedicle near the hepatic hilus. However, the tertiary branches that originate from the deep portions of the secondary pedicles cannot be approached from the hepatic hilus. These deep branches can be approached after initially dissecting the liver parenchyma on the border between the sections. The border between the sections can be confirmed by clamping the secondary pedicle at the hepatic hilus. If the tertiary branch that possibly feeds the territory which includes the tumor is found, the tertiary branch is clamped and the territory is confirmed. Following this procedure, we can evaluate the tumor located in the territory by intraoperative ultrasonography.
Fig. 7.
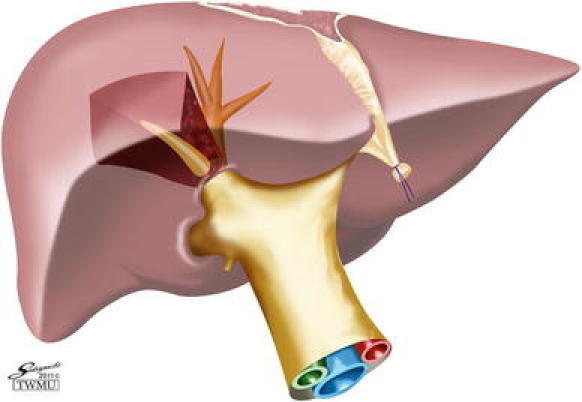
One secondary Glissonean pedicle has 6–8 tertiary branches. The territory of a single tertiary branch does not correspond to Couinaud’s segment
Discussion
Anatomical hepatectomy has been performed more easily using the Glissonean approach than by using controlled hepatectomy methods, which are exemplified by the intra-fascial approach of Couinaud. In particular, small anatomical hepatectomies such as sectionectomy or Couinoud’s segmentectomy are difficult to perform using controlled hepatectomy methods. When surgeons plan to carry out anterior sectionectomy using controlled hepatectomy methods, it takes a long time to dissect and confirm each branch of the hepatic artery, the portal vein and the bile duct to the anterior section. False confirmation of the hepatic artery or bile duct occasionally occurs. Makuuchi et al. [16] indicated anterior sectionectomy as the most difficult type of hepatic resection. However, surgeons can determine the area of the anterior section when one of the secondary Glissonean pedicles to the anterior section is dissected and clamped using the Glissonean pedicle approach. This procedure will shorten the operation time and reduce the stress on surgeons because they do not have to consider any anomalies of the arteries and bile ducts using this procedure.
Anatomical hepatectomy is different from partial hepatectomy, which does not consider the area that is fed by the sectional or segmental portal pedicle. In anatomical hepatectomy, the surgeon first ligates the portal pedicle and then confirms the area fed by the portal pedicle. After this, the surgeon identifies the tumor location and dissects the liver parenchyma along the border between the area fed and the area not fed by the portal pedicle. This anatomical hepatectomy approach is appropriate for liver tumors that invade the peripheral portal tract such as hepatocellular carcinoma (HCC). Because liver tumors invade the portal vein, tumor cells are disseminated to the sinusoids around the tumor and spread through the area which is fed by the portal vein. Therefore, anatomical hepatectomy is indicated for HCC. The advantages of anatomical hepatectomy for HCC have been indicated in previous studies [17, 18].
The advantage of the Glissonean pedicle approach is that it is a simple method which can separate the liver into 3 sections by simply clamping the secondary Glissonean pedicle extrahepatically without liver dissection at the hepatic hilus. The main hepatic vein, either the right hepatic vein or the middle hepatic vein, is present on the border between the sections. The relationship between the area of the section and the tumor location can be easily noted perioperatively by the Glissonean pedicle approach. Sectionectomy is considered as fundamental anatomical hepatectomy; however, when liver function is insufficient for sectionectomy, changing to smaller anatomical resections, such as cone unit resection, can be achieved by using the tertiary branches. Therefore, liver surgeons should know the Glissonean pedicle approach and should be able to perform any type of anatomical hepatectomy.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Conflict of interest
The authors declare that they have no conflict of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Footnotes
This article is based on studies first reported in Highly Advanced Surgery for Hepato-Biliary-Pancreatic Field (in Japanese), Tokyo: Igaku-Shoin, 2010.
References
- 1.Lortat-Jacob JL, Robert HG. Hepatectomie droite reglee. Presse Med. 1952;60:549–551. [PubMed] [Google Scholar]
- 2.Honjo I, Araki C. Total resection of the right lobe of the liver. J Int Coll Surg. 1955;23:23–28. [PubMed] [Google Scholar]
- 3.Foster JH, Berman MM. Highlights in the history of liver tumors and their resection. Solid liver tumors. Philadelphia: WB Saunders Company; 1977. pp. 9–27. [Google Scholar]
- 4.Lin TY, Chem KM, Liu TK. Total right hepatic lobectomy for primary hepatoma. Surgery. 1960;48:1048–1060. [PubMed] [Google Scholar]
- 5.Tung TT, Quang ND. A new technique for operating on the liver. Lancet. 1963;26:192–193. doi: 10.1016/S0140-6736(63)91210-8. [DOI] [Google Scholar]
- 6.Bismuth H. Surgical anatomy and anatomical surgery of the liver. World J Surg. 1982;6:3–9. doi: 10.1007/BF01656368. [DOI] [PubMed] [Google Scholar]
- 7.Takasaki K, Kobayashi S, Tanaka S, Muto H, Watayo T, Saito A, et al. Newly developed systematized hepatectomy by Glissonean pedicle transection method. Shujutsu. 1986;40:7–14. [Google Scholar]
- 8.Couinaud C. A simplified method for controlled left hepatectomy. Surgery. 1985;97:358–361. [PubMed] [Google Scholar]
- 9.Launois B, Jamieson GG. The importance of Glisson’s capsule and its sheath in the intrahepatic approach to resection of the liver. Surg Gynecol Obstet. 1992;174:7–10. [PubMed] [Google Scholar]
- 10.Couinaud C. The vasculo-biliary sheaths. Surgical anatomy of the liver revisited. Paris: Self-printed; 1989. pp. 29–39. [Google Scholar]
- 11.Gans H. On the subdivision of the liver. Introduction to hepatic surgery. Houston: Elsevier; 1955. pp. 1–39. [Google Scholar]
- 12.Strasberg SM. Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. J Hepatobiliary Pancreat Surg. 2005;12:351–355. doi: 10.1007/s00534-005-0999-7. [DOI] [PubMed] [Google Scholar]
- 13.Takasaki K, Kobayashi S, Tanaka S, Saito A, Yamamoto M, Hanyu F. Highly anatomically systematized hepatic resection with Glissonean sheath cord transection at the hepatic hilus. Int Surg. 1990;75:73–77. [PubMed] [Google Scholar]
- 14.Takasaki K. Glissonean pedicle transection method for hepatic resection: a new concept of liver segmentation. J Hepatobiliary Pancreat Surg. 1998;5:286–291. doi: 10.1007/s005340050047. [DOI] [PubMed] [Google Scholar]
- 15.Takasaki K. Glissonean pedicle transection method for hepatic resection. Tokyo: Springer; 2007. [DOI] [PubMed] [Google Scholar]
- 16.Makuuchi M, Hashikura Y, Kawasaki S, Tan D, Kosuge T, Takayama T. Personal experience of right anterior segmentectomy (segments V and VIII) for hepatic malignancies. Surgery. 1993;114:52–58. [PubMed] [Google Scholar]
- 17.Yamamoto M, Takasaki K, Ohtsubo T, Katsuragawa H, Fukuda C, Katagiri S. Effectiveness of systematized hepatectomy with Glisson’s pedicle transection at the hepatic hilus for small nodular hepatocellular carcinoma: retrospective analysis. Surgery. 2001;130:443–448. doi: 10.1067/msy.2001.116406. [DOI] [PubMed] [Google Scholar]
- 18.Hasegawa K, Kokudo N, Imamura H, Matsuyama Y, Aoki T, Minagawa M, et al. Prognostic impact of anatomic resection for hepatocellular carcinoma. Ann Surg. 2005;242:252–259. doi: 10.1097/01.sla.0000171307.37401.db. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.