

Abstract
CYP2C19 is one of the principal enzymes involved in the bioactivation of the antiplatelet prodrug clopidogrel. A common loss-of-function allele, CYP2C19*2 (c.681G>A; rs4244285), is associated with increased risk for serious adverse cardiovascular events in both heterozygous and homozygous patients (~25–50% of the population) with acute coronary syndromes (ACSs) who are receiving clopidogrel, particularly among those undergoing percutaneous coronary intervention (PCI). We provide evidence from published literature and guidelines for CYPC19 genotype–directed antiplatelet therapy (periodically updated at http://www.pharmgkb.org).
The purpose of these guidelines is to provide information regarding the clinical use of CYP2C19 genotype test results in patients requiring antiplatelet therapy. Detailed guidelines for use of other laboratory tests, such as platelet function monitoring, as well as a discussion of cost effectiveness, are beyond the scope of this article. The article does not focus on demographic and other clinical variables, such as adherence to therapy, age, diabetes mellitus, obesity, smoking, and concomitant use of other drugs, that may influence clopidogrel efficacy and clinical decision making. The Clinical Pharmacogenetics Implementation Consortium of the National Institutes of Health’s Pharmacogenomics Research Network develops peerreviewed gene/drug guidelines that are published and updated periodically at http://www.pharmgkb.org on the basis of new developments in the field.1
FOCUSED LITERATURE REVIEW
A systematic literature review was conducted on CYP2C19 genotype and clopidogrel (see Supplementary Data online). Guidelines for antiplatelet therapy were developed based on interpretation of the literature by authors and experts in the field.
Gene: CYP2C19
Background
The hepatic CYP2C19 enzyme contributes to the metabolism of many clinically relevant drugs such as antidepressants, benzodiazepines, mephenytoin, some proton pump inhibitors, and clopidogrel. Like many other CYP450 super-family members, the CYP2C19 gene is highly polymorphic, having more than 25 known variant alleles (http://www.cypalleles.ki.se/cyp2c19.htm). The CYP2C19*1 allele is associated with functional CYP2C19-mediated metabolism. The most common CYP2C19 loss-of-function allele is *2 (c.681G>A; rs4244285), with allele frequencies of ~15% in Caucasians and Africans, and 29–35% in Asians (Supplementary Tables S3 and S4 online). Other CYP2C19 variant alleles with reduced or absent enzymatic activity have been identified (e.g., *3–*8); however, their allele frequencies are typically <1%, with the exception of CYP2C19*3 (c.636G>A; rs4986893) in Asians (2–9%; Supplementary Data online).
CYP2C19*2 is inherited as an autosomal co-dominant trait; platelet responsiveness to clopidogrel in heterozygotes (*1/*2) lies somewhere between the responsiveness in individuals with the *1/*1 genotype and that in those with the *2/*2 genotype.2-7 Therefore, based on identified CYP2C19 genotypes, individuals can be categorized as extensive metabolizers (e.g., *1/*1), intermediate metabolizers (e.g., *1/*2), or poor metabolizers (e.g., *2/*2). The frequencies of CYP2C19 poor metabolizers are ~2–5% among Caucasians and Africans and ~15% in Asians (Supplementary Data online).
In contrast, the CYP2C19*17 allele (c.-806C>T; rs12248560) results in increased activity as a consequence of enhanced transcription, with average multi-ethnic allele frequencies of ~3–21% (Supplementary Tables S3 and S4 online). Individuals who carry this allele may be categorized as ultra-rapid metabolizers (e.g., *17/*17). Some studies indicate that this allele results in enhanced platelet inhibition and clopidogrel response,6,8-10 and possibly an increased risk of bleeding complications.11 However, other studies have not identified an effect of CYP2C19*17 (refs. 7,12,13), and adequate evidence for an independent effect of this allele on clinical outcomes is lacking.
Genetic test interpretation
Clinical genotyping tests are available that interrogate variant CYP2C19 alleles and predict an individual’s CYP2C19 metabolizer phenotype (Supplementary Data online). Each named star (*) allele is defined by the genotype at one or more specific single-nucleotide polymorphisms (Supplementary Table S1 online) and is associated with a level of enzyme activity (Supplementary Table S2 online). Table 1 and Supplementary Table S5 online summarize the assignment of the likely CYP2C19 phenotype based on common star allele diplotypes, and these assignments are used to link genotypes with personalized antiplatelet therapy.
Table 1.
Assigning likely CYP2C19 phenotypes based on genotypes
| Likely phenotype | Genotypes | Examples of diplotypes |
|---|---|---|
| Ultrarapid metabolizer: normal or increased activity (~5–30% of patients) | An individual carrying two increased-activity alleles (*17), or one functional allele (*1) plus one increased-activity allele (*17) | *1/*17, *17/*17 |
| Extensive metabolizer: homozygous wild-type or normal activity (~35–50% of patients) | An individual carrying two functional (*1) alleles | *1/*1 |
| Intermediate metabolizer: heterozygote or intermediate activity (~18–45% of patients) | An individual carrying one functional allele (*1) plus one loss-of-function allele (*2–*8) | *1/*2, *1/*3 |
| Poor metabolizer: homozygous variant, mutant, low, or deficient activity (~2–15% of patients) | An individual carrying two loss-of-function alleles (*2–*8) | *2/*2, *2/*3, *3/*3 |
For some rare genotype combinations metabolic phenotypes are difficult to predict; see Supplementary Table S3 online.
Available genetic test options
A number of academic and commercial clinical laboratories offer genetic testing for CYP2C19*2 and other CYP2C19 variant alleles (Supplementary Data online). However, at the time of this writing, only the CYP2C19*2 allele has been adequately studied with respect to clinical outcomes on clopidogrel; other variants are too rare, have not been studied, or have resulted in inconclusive findings.
Incidental findings
There are no diseases or conditions that have been convincingly linked to variations in the CYP2C19 gene independent of drug metabolism and response.
Other considerations
CYP2C19 loss-of-function alleles do not account for all of the variability in clopidogrel response. Some studies have implicated variants in other genes associated with clopidogrel response (Supplementary Data online); however, these have not been consistently replicated.
Drug: clopidogrel
Background
Clopidogrel is a thienopyridine prodrug that requires hepatic biotransformation to form an active metabolite that selectively and irreversibly inhibits the purinergic P2RY12 receptor, and thereby platelet aggregation, for the platelet’s life span (~10 days). Only 15% of the prodrug is available for transformation to the active agent; the other 85% is hydrolyzed by esterases to inactive forms. Conversion of clopidogrel to its active metabolite requires two sequential oxidative steps involving several CYP450 enzymes (e.g., CYP1A2, CYP2B6, CYP2C9, CYP2C19, and CYP3A4/5; Supplementary Figure S1 online). A recent study suggested that paraoxonase 1 (PON1) may also be involved in clopidogrel activation.14
Linking genetic variability to variability in drug-related phenotypes
Clopidogrel is commonly prescribed for ACSs and/or following PCI. However, responses to clopidogrel vary widely, with inhibition of adenosine diphosphate–induced platelet aggregation being normally distributed across a broad range.7 Many studies have shown that CYP2C19*2 carriers have lower levels of active clopidogrel metabolites and higher on-treatment platelet aggregation as compared to noncarriers.2-4,6,7,15 Moreover, substantial evidence exists linking CYP2C19 genotype with clinical response among clopidogrel-treated ACS patients,2,5-7,13,16,17 probably as a result of decreased formation of the active clopidogrel metabolite. For example, large meta-analyses (Supplementary Table S7 online) have shown that CYP2C19*2 carriers treated with clopidogrel have a higher risk for major adverse cardiovascular events as compared to noncarriers (hazard ratio (HR) 1.55, 95% confidence interval (CI) 1.11–2.17 for heterozygotes; HR 1.76, 95% CI 1.24–2.50 for homozygotes), and higher risks of stent thrombosis (HR 2.67, 95% CI 1.69–4.22 for heterozygotes; HR 3.97, 95% CI 1.75–9.02 for homozygotes).18
The growing body of literature implicating CYP2C19*2 (and perhaps other loss-of-function alleles) in adverse clopidogrel responses prompted the US Food and Drug Administration to implement a boxed warning on the clopidogrel label describing the relationship between CYP2C19 pharmacogenetics and drug response, particularly noting the drug’s diminished effectiveness in poor metabolizers. However, because the agency’s warning is not accompanied by a requirement for compulsory genetic testing before initiating clopidogrel therapy, if a patient’s genotype is not known, the decision to perform CYP2C19 testing is up to the individual clinician and patient.
Studies linking CYP2C19 genotype with variability in clopidogrel response are summarized in Supplementary Tables S6 and S7 online; it is this body of evidence, rather than randomized clinical trials involving pharmacogenetic testing that provides the basis for the therapeutic guidelines in Table 2. Importantly, the most definitive studies showing a relationship between CYP2C19 genotype and clopidogrel response have been conducted in patients with ACSs, most of whom underwent PCIs. As such, these findings may not apply to all indications for clopidogrel, including atrial fibrillation, stroke, peripheral artery disease, and chronic stable angina.19,20 The guidelines set forth here, therefore, apply largely to patients taking clopidogrel in whom invasive PCIs have been performed with drug-eluting or bare-metal stents.
Table 2.
Clopidogrel therapy based on CYP2C19 phenotype for ACS/PCI patients initiating antiplatelet therapy
| Phenotype (genotype) | Implications for clopidogrel | Therapeutic recommendations | Classification of recommendationsa |
|---|---|---|---|
| Ultrarapid metabolizer (UM) (*1/*17, *17/*17) and extensive metabolizer (EM) (* 1/*1) | Normal (EM) or increased (UM) platelet inhibition; normal (EM) or decreased (UM) residual platelet aggregationb | Clopidogrel label-recommended dosage and administration | Strong |
| Intermediate metabolizer (IM) (*1/*2) | Reduced platelet inhibition; increased residual platelet aggregation; increased risk for adverse cardiovascular events | Prasugrel or other alternative therapy (if no contraindication) | Moderate |
| Poor metabolizer (PM) (*2/*2) | Significantly reduced platelet inhibition; increased residual platelet aggregation; increased risk for adverse cardiovascular events | Prasugrel or other alternative therapy (if no contraindication) | Strong |
ACS, acute coronary syndrome; PCI, percutaneous coronary intervention.
See Supplementary Data online, Strength of Therapeutic Recommendations.
The CYP2C19*17 allele may be associated with increased risk of bleeding.11
CYP2C19 genetic test interpretation and suggested clinical actions
Who should be genotyped for CYP2C19? Recently, the American College of Cardiology Foundation/American Heart Association outlined possible actions by clinicians in response to the Food and Drug Administration’s boxed warning.21 The article fell short of recommending CYP2C19 genetic testing, citing the absence of prospective randomized clinical outcomes trials of genotype-directed antiplatelet therapy. However, such a clinical trial will take several years to perform; given the substantial body of evidence from the current literature (reviewed above) and potentially more efficacious antiplatelet therapy alternatives (see below), some physicians may choose to modify therapy based on genotype.
One option is to genotype all patients who undergo PCI and thereafter require antiplatelet therapy. Given the excellent clinical course generally observed among the majority of PCI patients treated with clopidogrel, another approach is to target patients who are considered to be at moderate or high clinical risk for poor outcomes in the setting of suboptimal antiplatelet therapy. This includes, for example, patients undergoing high-risk multi-vessel PCI procedures, those who have already had an adverse outcome (e.g., stent thrombosis), and/or those with other high-risk clinical (e.g., ACS, diabetes mellitus, and chronic kidney failure) or angiographic features.
How should CYP2C19 genotype results be acted upon? Optimal individualized antiplatelet treatment should maximize benefit by reducing risk of recurrent cardiovascular events while minimizing adverse effects such as bleeding. Prasugrel is a new antiplatelet agent that does not depend on CYP2C19 for activation and that was found to be superior to clopidogrel with respect to cardiovascular events (HR for prasugrel vs. clopidogrel 0.81, 95% CI 0.73–0.90, P < 0.001).22 However, it may not represent a substitute for clopidogrel in all patients because of (i) a higher associated risk of bleeding (HR 1.32, 95% CI 1.03–1.68, P = 0.03), including fatal bleeding (prasugrel 0.4% vs. clopidogrel 0.1%, P = 0.002)22; (ii) the fact that its use at full dose is not recommended, and lower doses of prasugrel have not been adequately studied; (iii) the larger number of conditions for which clopidogrel is approved; and (iv) the lower expense of clopidogrel as it progressively comes off patent worldwide. In addition to prasugrel, ticagrelor23 has been approved in Europe, and other antiplatelet alternatives are being developed. Older alternatives to clopidogrel include ticlopidine and cilostazol.
Table 2 and Figure 1 summarize the therapeutic guidelines for clopidogrel based on CYP2C19 phenotype. Standard dosing of clopidogrel, as recommended in the product insert, is warranted among patients with a CYP2C19 extensive metabolizer or ultra-rapid metabolizer phenotype (i.e., *1/*1, *1/*17, and *17/*17).24 If clinical genotyping identifies a patient as a CYP2C19 poor metabolizer (i.e., *2/*2), current literature supports the use of an alternative agent (e.g., prasugrel, ticagrelor), provided it is not contraindicated clinically.6,22,25-28
Figure 1.
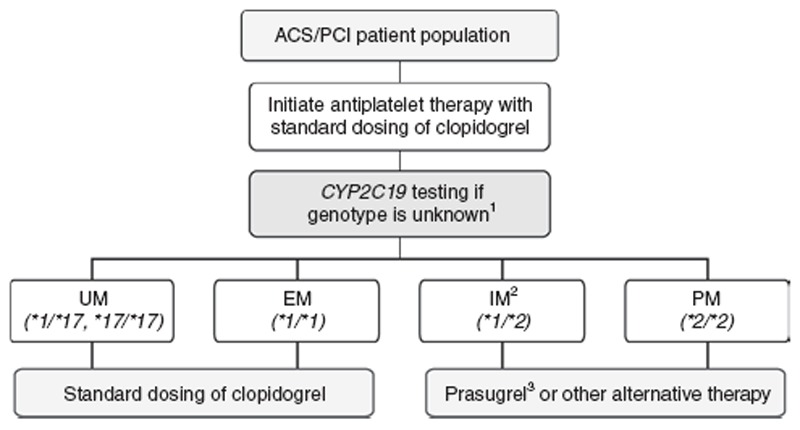
Algorithm for suggested clinical actions based on CYP2C19 genotype in patients with acute coronary syndromes initiating antiplatelet therapy. ACS, acute coronary syndrome; EM, extensive metabolizer; IM, intermediate metabolizer; PCI, percutaneous coronary intervention; PM, poor metabolizer; UM, ultrarapid metabolizer. 1Other rare CYP2C19 genotypes exist apart from those illustrated (see Supplementary Data online for other genotypes and frequencies). 2Higher-dose clopidogrel has not been adequately studied at the time of this writing but may improve platelet function in a subset of IMs and PMs (Supplementary Table S8 online).3Note that prasugrel is recommended only when its use is not clinically contraindicated.
The most challenging patient population to address is the CYP2C19 intermediate metabolizer phenotype (e.g., *1/*2). Intermediate metabolizers have higher on-treatment residual platelet activity on average as compared to extensive metabolizers, 2-4,6,7 and CYP2C19*2 heterozygous patients with ACSs who receive treatment with clopidogrel have higher risks for adverse cardiovascular outcomes including stent thrombosis18 (see Supplementary Data online). These data support switching to an alternative antiplatelet agent for intermediate metabolizers if there is no contraindication. Given the wide interindividual variability in residual platelet activity observed among intermediate metabolizers receiving clopidogrel, and taking into account other factors that may place intermediate metabolizer patients at increased risk of a cardiovascular (or adverse bleeding) event, clinical judgment should be exercised to determine the most effective individualized therapy.
In recent pilot studies, increasing the clopidogrel maintenance dose from 75 to 150 mg/day increased platelet inhibition in some, but not all, patients who were CYP2C19*2 heterozygotes (ref. 29 and Supplementary Table S8 online). However, given that dose escalation was recently reported to produce no benefit among post-PCI patients with high on-treatment platelet reactivity, 30 it is currently premature to support a recommendation for an increased maintenance dose of 150 mg/day in CYP2C19 intermediate metabolizers. Equally controversial is the use of platelet function testing alone (e.g., GRAVITAS and TRIGGERPCI trial results) or in combination with CYP2C19 genotype information. Future versions of these guidelines (updated at http://www.pharmgkb.org) will incorporate results from ongoing clinical trials that are designed to address these and other emerging issues.
Other considerations
Diabetes mellitus, increased age, and higher body mass index are associated with high on-treatment residual platelet aggregation, and the use of certain proton pump inhibitors may also affect clopidogrel response. In addition, although these guidelines have been limited to the CYP2C19*2 allele, many clinical genotyping platforms include other variant alleles (*3–*8, *17) that may alter the interpretation of a patient’s predicted metabolizer phenotype (Supplementary Table S3 online). There are reports that variants in other genes such as ABCB1, P2YR12, and PON1 may affect clopidogrel metabolism and/or efficacy, but the body of evidence does not support genotyping for these variants at the present time.
Potential benefits and risks for the patient
The potential benefits of CYP2C19 testing are that patients with genotypes associated with a higher risk of adverse cardiovascular events during clopidogrel therapy can be identified, and an alternative antiplatelet strategy can be instituted. Although there is mounting evidence associating deficient CYP2C19 with increased risks of adverse cardiovascular outcomes in patients on clopidogrel therapy, there are potential risks in making changes in a patient’s therapy on the basis of CYP2C19 genotype in the absence of randomized clinical trial evidence. CYP2C19 genotyping is straightforward and reliable when performed in qualified laboratories. However, as with any laboratory test, an additional possible risk to the patient is an error in genotyping. Because genotype test results are applied life-long, any such error could have adverse health implications throughout the lifetime of the patient.
Caveats: appropriate use and/or potential misuse of genetic tests
One of the challenges for clinical pharmacogenetic testing is the need for rapid turnaround time and quick reporting of results. When a decision is made to pursue CYP2C19 testing, it would be advantageous to have the results prior to initiating antiplatelet therapy because most potentially preventable recurrent events occur early; however, in the acute PCI setting, this is not easily achievable. Therefore, if CYP2C19 genotype is not already known from prior testing, every effort should be made to initiate CYP2C19 testing as early as possible and to emphasize the need for expedited results. These recommendations apply only to patients with coronary disease; e.g., those with ACSs or undergoing PCI, especially those with stent placements. Current data do not support the use of CYP2C19 genotyping in other patient populations receiving clopidogrel.19,20
Supplementary Material
Acknowledgments
We acknowledge the critical input of W. Herzog, J. Knowles, M. Relling, J. Shin, and members of the Clinical Pharmacogenetics Implementation Consortium (CPIC) of the Pharmacogenomics Research Network, funded by the National Institutes of Health (NIH). This work was supported by NIH KL2 RR029885 (S.A.S.), U01 JL65962 (C.M.S), U01 GM074492 (J.A.J.), U19 HL065962-10 (D.M.R.), R24 GM61374 (K.S. and T.E.K.), and U01 HL105198 (A.R.S.). CPIC guidelines reflect expert consensus based on clinical evidence and peer-reviewed literature available at the time they are written and are intended only to assist clinicians in decision making and to identify questions for further research. New evidence may have emerged since the time a guideline was submitted for publication. Guidelines are limited in scope and are not applicable to interventions or diseases not specifically identified. Guidelines do not account for all individual variations among patients and cannot be considered inclusive of all proper methods of care or exclusive of other treatments. It remains the responsibility of the health-care provider to determine the best course of treatment for a patient. Adherence to any guideline is voluntary, with the ultimate determination regarding its application to be made solely by the clinician and the patient. CPIC assumes no responsibility for any injury to persons or damage to persons or property arising out of or related to any use of CPIC’s guidelines or for any errors or omissions.
S.A.S. receives support from NIH for antiplatelet pharmacogenomics research and is a consultant to USDS, Inc. J.-S.H. has received research grant support from Fondation de France, INSERM, Fédération Francaise de Cardiologie, Biotronik, and Medco Research Institute; consulting fees from Biotronik and Medco Health Solutions; and lecture fees from Daiichi Sankyo, Eli Lilly, and Bristol-Myers Squibb. J.A.J. receives support from NIH for cardiovascular pharmacogenomics research, including clopidogrel. D.M.R. receives support from NIH for pharmacogenomics research and is a consultant to Merck, Novartis, Dai-ichi, Sanofi, and Astellas. A.R.S. receives support from NIH for antiplatelet pharmacogenomics research and is consultant to Bristol-Myers Squibb and USDS, Inc.
Footnotes
SUPPLEMENTARY MATERIAL is linked to the online version of the paper at http://www.nature.com/cpt
CONFLICT OF INTEREST The other authors declared no conflict of interest.
References
- 1.Relling MV, Klein TE. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin Pharmacol Ther. 2011;89:464–467. doi: 10.1038/clpt.2010.279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hulot JS, et al. Cytochrome P450 2C19 loss-of-function polymorphism is a major determinant of clopidogrel responsiveness in healthy subjects. Blood. 2006;108:2244–2247. doi: 10.1182/blood-2006-04-013052. [DOI] [PubMed] [Google Scholar]
- 3.Brandt JT, et al. Common polymorphisms of CYP2C19 and CYP2C9 affect the pharmacokinetic and pharmacodynamic response to clopidogrel but not prasugrel. J Thromb Haemost. 2007;5:2429–2436. doi: 10.1111/j.1538-7836.2007.02775.x. [DOI] [PubMed] [Google Scholar]
- 4.Umemura K, Furuta T, Kondo K. The common gene variants of CYP2C19 affect pharmacokinetics and pharmacodynamics in an active metabolite of clopidogrel in healthy subjects. J Thromb Haemost. 2008;6:1439–1441. doi: 10.1111/j.1538-7836.2008.03050.x. [DOI] [PubMed] [Google Scholar]
- 5.Collet JP, et al. Cytochrome P450 2C19 polymorphism in young patients treated with clopidogrel after myocardial infarction: a cohort study. Lancet. 2009;373:309–317. doi: 10.1016/S0140-6736(08)61845-0. [DOI] [PubMed] [Google Scholar]
- 6.Mega JL, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009;360:354–362. doi: 10.1056/NEJMoa0809171. [DOI] [PubMed] [Google Scholar]
- 7.Shuldiner AR, et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA. 2009;302:849–857. doi: 10.1001/jama.2009.1232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Frére C, Cuisset T, Gaborit B, Alessi MC, Hulot JS. The CYP2C19*17 allele is associated with better platelet response to clopidogrel in patients admitted for non-ST acute coronary syndrome. J Thromb Haemost. 2009;7:1409–1411. doi: 10.1111/j.1538-7836.2009.03500.x. [DOI] [PubMed] [Google Scholar]
- 9.Sibbing D, et al. Isolated and interactive impact of common CYP2C19 genetic variants on the antiplatelet effect of chronic clopidogrel therapy. J Thromb Haemost. 2010;8:1685–1693. doi: 10.1111/j.1538-7836.2010.03921.x. [DOI] [PubMed] [Google Scholar]
- 10.Tiroch KA, et al. Protective effect of the CYP2C19 *17 polymorphism with increased activation of clopidogrel on cardiovascular events. Am Heart J. 2010;160:506–512. doi: 10.1016/j.ahj.2010.06.039. [DOI] [PubMed] [Google Scholar]
- 11.Sibbing D, et al. Cytochrome 2C19*17 allelic variant, platelet aggregation, bleeding events, and stent thrombosis in clopidogrel-treated patients with coronary stent placement. Circulation. 2010;121:512–518. doi: 10.1161/CIRCULATIONAHA.109.885194. [DOI] [PubMed] [Google Scholar]
- 12.Geisler T, et al. CYP2C19 and nongenetic factors predict poor responsiveness to clopidogrel loading dose after coronary stent implantation. Pharmacogenomics. 2008;9:1251–1259. doi: 10.2217/14622416.9.9.1251. [DOI] [PubMed] [Google Scholar]
- 13.Simon T, et al. French Registry of Acute ST-Elevation and Non-ST-Elevation Myocardial Infarction (FAST-MI) Investigators. Genetic determinants of response to clopidogrel and cardiovascular events. N Engl J Med. 2009;360:363–375. doi: 10.1056/NEJMoa0808227. [DOI] [PubMed] [Google Scholar]
- 14.Bouman HJ, et al. Paraoxonase-1 is a major determinant of clopidogrel efficacy. Nat Med. 2011;17:110–116. doi: 10.1038/nm.2281. [DOI] [PubMed] [Google Scholar]
- 15.Kim KA, Park PW, Hong SJ, Park JY. The effect of CYP2C19 polymorphism on the pharmacokinetics and pharmacodynamics of clopidogrel: a possible mechanism for clopidogrel resistance. Clin Pharmacol Ther. 2008;84:236–242. doi: 10.1038/clpt.2008.20. [DOI] [PubMed] [Google Scholar]
- 16.Giusti B, et al. Relation of cytochrome P450 2C19 loss-of-function polymorphism to occurrence of drug-eluting coronary stent thrombosis. Am J Cardiol. 2009;103:806–811. doi: 10.1016/j.amjcard.2008.11.048. [DOI] [PubMed] [Google Scholar]
- 17.Sibbing D, et al. Cytochrome P450 2C19 loss-of-function polymorphism and stent thrombosis following percutaneous coronary intervention. Eur Heart J. 2009;30:916–922. doi: 10.1093/eurheartj/ehp041. [DOI] [PubMed] [Google Scholar]
- 18.Mega JL, et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: a meta-analysis. JAMA. 2010;304:1821–1830. doi: 10.1001/jama.2010.1543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Paré G, et al. Effects of CYP2C19 genotype on outcomes of clopidogrel treatment. N Engl J Med. 2010;363:1704–1714. doi: 10.1056/NEJMoa1008410. [DOI] [PubMed] [Google Scholar]
- 20.Wallentin L, et al. PLATO investigators. Effect of CYP2C19 and ABCB1 single nucleotide polymorphisms on outcomes of treatment with ticagrelor versus clopidogrel for acute coronary syndromes: a genetic substudy of the PLATO trial. Lancet. 2010;376:1320–1328. doi: 10.1016/S0140-6736(10)61274-3. [DOI] [PubMed] [Google Scholar]
- 21.Holmes DR, Jr, Dehmer GJ, Kaul S, Leifer D, O’Gara PT, Stein CM. ACCF/AHA clopidogrel clinical alert: approaches to the FDA “boxed warning”: a report of the American College of Cardiology Foundation Task Force on clinical expert consensus documents and the American Heart Association endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2010;56:321–341. doi: 10.1016/j.jacc.2010.05.013. [DOI] [PubMed] [Google Scholar]
- 22.Wiviott SD, et al. TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357:2001–2015. doi: 10.1056/NEJMoa0706482. [DOI] [PubMed] [Google Scholar]
- 23.Wallentin L, et al. PLATO Investigators. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361:1045–1057. doi: 10.1056/NEJMoa0904327. [DOI] [PubMed] [Google Scholar]
- 24.Sorich MJ, Vitry A, Ward MB, Horowitz JD, McKinnon RA. Prasugrel vs. clopidogrel for cytochrome P450 2C19-genotyped subgroups: integration of the TRITON-TIMI 38 trial data. J Thromb Haemost. 2010;8:1678–1684. doi: 10.1111/j.1538-7836.2010.03923.x. [DOI] [PubMed] [Google Scholar]
- 25.Wallentin L, et al. Prasugrel achieves greater and faster P2Y12receptor-mediated platelet inhibition than clopidogrel due to more efficient generation of its active metabolite in aspirin-treated patients with coronary artery disease. Eur Heart J. 2008;29:21–30. doi: 10.1093/eurheartj/ehm545. [DOI] [PubMed] [Google Scholar]
- 26.Mega JL, et al. Cytochrome P450 genetic polymorphisms and the response to prasugrel: relationship to pharmacokinetic, pharmacodynamic, and clinical outcomes. Circulation. 2009;119:2553–2560. doi: 10.1161/CIRCULATIONAHA.109.851949. [DOI] [PubMed] [Google Scholar]
- 27.Pena A, et al. Can we override clopidogrel resistance? Circulation. 2009;119:2854–2857. doi: 10.1161/CIRCULATIONAHA.108.857722. [DOI] [PubMed] [Google Scholar]
- 28.Montalescot G, et al. Prasugrel compared with high-dose clopidogrel in acute coronary syndrome. The randomised, double-blind ACAPULCO study. Thromb Haemost. 2010;103:213–223. doi: 10.1160/TH09-07-0482. [DOI] [PubMed] [Google Scholar]
- 29.Bonello L, et al. Clopidogrel loading dose adjustment according to platelet reactivity monitoring in patients carrying the 2C19*2 loss of function polymorphism. J Am Coll Cardiol. 2010;56:1630–1636. doi: 10.1016/j.jacc.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 30.Price MJ, et al. GRAVITAS Investigators. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305:1097–1105. doi: 10.1001/jama.2011.290. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.