

Abstract
Objective and Background:
Measures to promote patient satisfaction are important components of the assessment of outcome and strategies for the delivery of health care. In this article, we assess satisfaction among inpatients and the impact of demographics on satisfaction levels.
Materials and Methods:
This cross-sectional survey adapted from previously used survey tools and validated in our patient group included questions on demographics, communication skills, hospital environment, and the patients’ overall evaluation of the hospital. Inpatients from acute wards of five different specialties who stayed for at least 2 days were enrolled.
Results:
There were 988 respondents with a mean age of 39.1 years (25.9%) and the mean length of stay (LOS) of 10.0 days (24.1%). Illiteracy rate was 42.4%, and 43.1% were male. The overall satisfaction scores—out of five—were 4.3 (0.6%) for communication with nurses, 4.4 (0.4%) for communication with doctors, and 4.1 (0.3%) for hospital environment; 98.9% of the patients would recommend the hospital to their family and friends. The lowest score was for the “room environment” (3.99, 0.8%) and the highest for overall services of the hospital (4.7, 0.5%). Satisfaction levels drop significantly with LOS of more than 4 days (P < 0.006). The satisfaction was higher in females than males across all the three domains of care assessed (P < 0.005). The highest satisfaction seen in the obstetrics service could be explained by the nature of the condition normally seen in this department and the normally good outcome. There was higher satisfaction in the medical than surgical services but this reached a significant level for the overall center score domain only (4.1, 0.3% versus 4.0, 0.3%; P < 0.0001).
Conclusion:
The factors with positive impact on satisfaction were the female gender and shorter LOS. There was higher satisfaction in the medical than surgical services for all three domains reaching significant levels for center score only.
Keywords: Patient satisfaction, Saudi Arabia
INTRODUCTION
Patient satisfaction is an important element in patient management.[1,2] The more satisfied patients are with their experience as inpatients; fewer complaints are there from patients and their relatives. Satisfaction among patients has been shown to result in better quality of work and less burnout of healthcare providers.[2–5] Satisfaction and positive experience in a health service goes beyond the narrow confines of medical care issues and involves personal relationships, attention to pain, and health education and the status of the hospital environment.[6–10] Recurrent reasons for dissatisfaction in many studies from different parts of the world have been related to a long wait for attention and unmet expectations.[7,8,11,12]
The quality of care could be monitored and assessed in a number of ways.[6,13] One way that is not fully used and monitored is what the patients themselves think of the services they are given. Assessments and perceptions of healthcare providers and administrators of the quality and standard of the service provided may often differ completely from the patients’ perceptions of the same services.[14]
Many hospitals now believe in a culture of patient centeredness which is cultivated and nurtured at the highest level of management. Measurement of satisfaction is thought to be an essential component in quality improvement.[14]
In this article, we aim at investigating the experience and degree of satisfaction of patients in a Saudi tertiary care hospital with their physicians, nurses, and hospital center as a whole and to investigate the factors that determine this satisfaction.
MATERIALS AND METHODS
This is a cross-sectional survey-based study. We adopted a modified tool that combines the Hospital Consumer Assessment of Healthcare Providers and Systems survey approved by the National Quality Forum,[14] and the US Health and Human Services Survey Health Center Patient Satisfaction Survey. These tools were developed as standard for assessing patients’ experience and the comparison of hospitals.[15]
The survey instrument consisted of three sections:
The first section gathered demographic data on the respondents.
-
The second section assessed three domains of care:
- Communication with nurses (four questions).
- Communication with doctors (four questions).
- Hospital environment (seven questions).
The third section was designed to evaluate the overall hospital assessment by the patient. (three questions).
The tool was translated into Arabic and then back into English by independent persons to check the accuracy of translation. The survey was tested initially on a group of 50 patients to see if it was comprehensible. Reliability analysis was performed using Cronbach's alpha test.
Patients included were those admitted to acute beds staying for at least 2 days and willing and able to understand the questions. Written consents were obtained from all respondents. Consent was given by either the patients themselves or one of their relatives. Wards covering the following specialties were included: medicine, pediatrics, surgery, obstetrics and the business center. All questionnaires were completed by one research assistant not involved in the care of the patients who directly interviewed the respondents. The ethical approval was granted by the institutional review board at King Abdulaziz Medical City.
Statistical analysis
Data collected in this study were entered into a Microsoft Access database specifically structured for this study. It was then transferred to the Statistical Analysis Software, version 9.2 used for data cleaning, management, and analyses.
Descriptive statistics was carried out by calculating the mean and standard deviation for the continuous variables, and the number and percentage for the categorical variables. Inferential statistics was carried out by using the Student's t-test to compare the means between groups. The means of responses for each domain of care were averaged and compared using independent sample t-test. Moreover, multivariate regression analyses were used to assess the effects of potentially confounding variables on the satisfaction scores.
RESULTS
Demographics
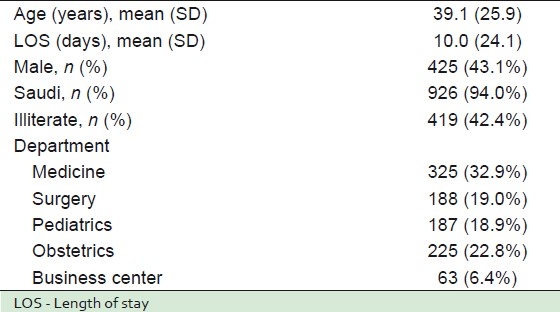
Nine hundred eighty-eight consecutive respondents completed the survey (91.2% response rate). Those who refused did not differ in characteristics from those who took part. The mean age was 39.1 years (25.9%) and the mean length of stay (LOS) was 10.0 days (24.1%) with an illiteracy rate of 42.4%; 43.1% were male. Important demographic data are shown in Table 1.
Table 1.
Demographic data (n = 988)
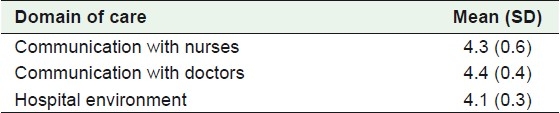
Overall scores in the three domains of care
This is shown in Table 2. For this part of the survey, the respondents were asked to grade their responses to the questions according to the following Likert score: 1 = very bad, 2 = bad, 3 = satisfactory, 4 = good, and 5 = excellent. In other words, the higher the score, the higher the satisfaction.
Table 2.
Overall scores (out of 5)
Overall hospital evaluation
Table 3 shows the overall hospital evaluation by the respondents. This is based on their responses to the following three questions:
Table 3.
Overall hospital evaluation

Would you recommend this hospital to your family and friends?
How do you rate this hospital?
Would you use this hospital again even if you had resources to go to another hospital inside or outside the Kingdom?
Scoring of satisfaction to each of the questions in the three domains
The percentages of respondents who gave the answer (good, excellent, or both) are shown in Table 4. In addition, the mean scores ± STD are shown for each question. The lowest score was for “how was your room”: 3.99 (0.8%) and the highest for “rating the overall services of the hospital”: 4.7 (0.5%).
Table 4.
“Good” and “Excellent” responses to all the questions asked
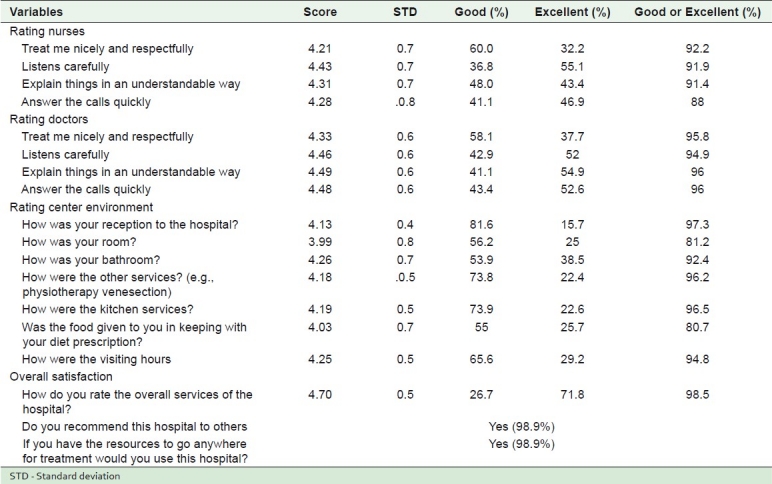
The highest percentage of those who answered “excellent” only was for the question “how do you rate the overall services of the hospital? (71.8%) and the lowest was for the question “how was your reception to the hospital? (15.7%).
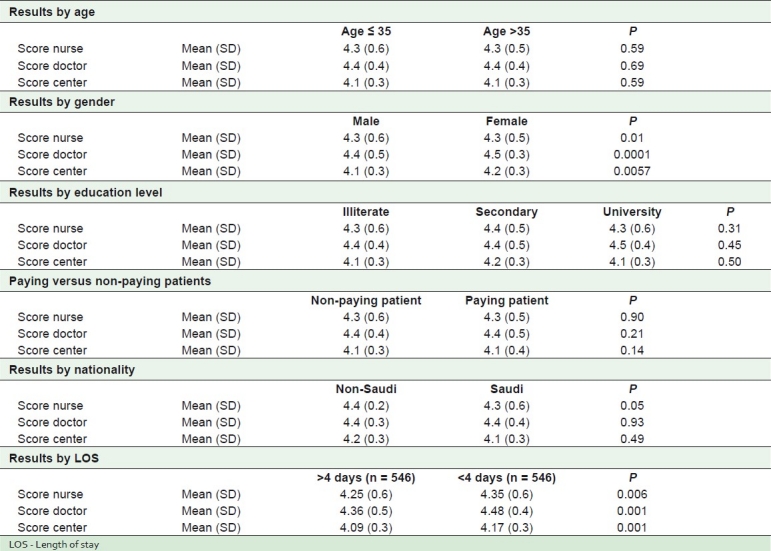
Table 5 shows a significant impact of gender and LOS, but none by educational level, payment of fees or nationality, and LOS.
Table 5.
Impact of age, gender, educational level, paying for treatment, nationality, and LOS
Results in the three domains in the medical, obstetrics, and surgical wards
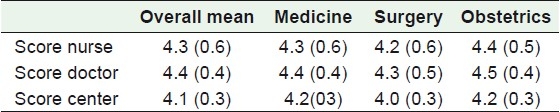
Table 6 shows the mean satisfaction scores overall and in medicine, obstetrics, and surgery. Service by obstetrics scored the highest followed by service in the medical department. Services given by surgery had the lowest scores, but this reached a significant level for the center score only (4.1, 0.3% versus 4.0, 0.3%; P < 0.0001).
Table 6.
Mean satisfaction scores overall and in medicine, obstetrics, and surgery
To certify that the higher satisfaction scores for obstetrics service were not merely the result of gender bias, the mean scores (SD) by female patients only were compared for the departments of medicine, surgery, and obstetrics [Table 7 and Figure 1]. This showed that obstetrics still scored significantly higher than the other departments.
Table 7.
Mean scores (SD) by female patients only in the three domains of care in the departments of medicine, surgery, and obstetrics

Figure 1.
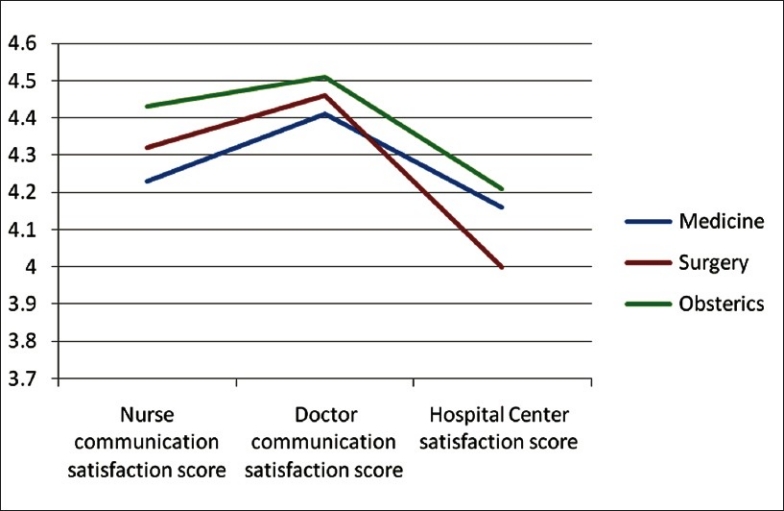
Mean scores (SD) by female patients only in the three domains of care in the departments of medicine, surgery, and obstetrics
DISCUSSION
It has been well documented that patient-centered approach to patient care results in a better outcome in both clinical and emotional health and minimizes the need for expensive diagnostic tests.[1] It has also been shown that patients’ satisfaction is associated with clinician satisfaction[2,3] and less burnout.[4,5] Patient satisfaction is also known to be positively influenced by friendliness and the provision of information on the part of the physician.[16]
We had an excellent response rate of 91.2%. This was largely due to the approach of using the help of a dedicated research assistant who spoke to the respondents directly. The small percentage of respondents was similar demographically to those who responded and, therefore, this presented no concerns of bias.
Our study showed that the mean score for nurses in this area was 86.2% and for doctors 88.8%. The mean overall score for hospital environment was 83%. The highest score was for the convenience of the visiting hours (85%) and the lowest score was for the room environment (79.8%).
The rating for the overall services of the hospital was high (94%) with 71.8% of the respondents rating it as excellent and almost 99% saying they would recommend it to others and would use it again even if they had the resources to seek treatment anywhere else inside or outside the country. The recommendation rate of 98.8% by our patients is higher than the average seen in US hospitals (68%).[15]
Our female patients had higher satisfaction scores than the male patients. Other reports did not show gender differences in satisfaction scores.[17] It is possible that our females learn to expect less and are, therefore, more likely to be satisfied by services than men. Alternatively, it is conceivable that females are indeed treated with more empathy and courtesy than the male patients and are thus truly more satisfied. In a study in another university hospital in Riyadh, it was also found that females were more satisfied than males.[18]
Obstetrics service scored the highest followed by medicine. Surgical services scored the lowest in all three domains, but reached significant level for center score only. The high score for obstetrics may simply be a reflection of the higher scores given by females in general that we observed. However, on scrutinizing the scores by the female patients only in all the services, it was found that obstetrics still scored significantly higher than the other services when it came to the female patients only. This suggests that this was not a biased result due simply to the fact that ObGyn has female patients only. One could speculate that this could be explained by a few factors including peri-partum family support. Indeed, Nohara and Miyagi[19] showed that husbands’ and parents’ support for pregnant women after birth strongly correlates with better quality of life, in addition to improving mothers’ child care and conditions of health. The manifestation of this psychosocial support varies from one culture to another. In Mexico, for example, a female companion (known as “doula”) offers continuous support to her pregnant friend. A randomized clinical trial by Langer et al[20] confirmed that psychosocial support by "doulas" had a positive effect on both duration of labor and subsequent events. Furthermore, breastfeeding itself, especially for new mothers, may be an exhilarating experience filled with emotional satisfaction,[21] explaining further the higher rate of patient satisfaction seen in the obstetrics wards. It is interesting to note that a study done at another university hospital in Riyadh also showed that the highest mean satisfaction score was for obstetrics and the lowest was for surgery.[18]
Business center scores were similar to those of the other services. Business center patients are fee-paying patients, while other patients are treated free of charge. Thus, being a private patient does not affect the degree of satisfaction one way or the other. One study showed that while fee-paying patients had similar levels of satisfaction in center and nursing services to non-paying patients, they were more satisfied with their physicians than non-fee-paying patients.[22] This could simply be due to the fact that they determine which doctors should treat them. Our fee-paying patients were significantly older and better educated than non-fee-paying patients with a predominance of males. This confirms previous findings from Saudi Arabia.[23] A comparison of fee-paying and non-fee-paying patients in some public and private hospitals in Riyadh showed that the former were the most dissatisfied with all aspects of the care they received.[24]
Age had no impact on satisfaction scores. In a study on walk-in general medicine clinic in the United States, it was found that patients over the age of 65 years were more likely to be satisfied.[12] In a study in Vietnam, it was also found that older patients were more likely to be satisfied, but there was no difference in satisfaction levels between males and females. This was attributed to the lower levels of education in older patients.[25] Educational level had no impact on satisfaction in our study. Other reports from Saudi Arabia, however, indicated that the more educated the patients were, the more likely they were to be satisfied.[24,26]
The longer LOS was associated with significantly lower levels of satisfaction. This might be because the empathy of healthcare providers and attention wanes as the patients’ hospital stay lengthens. Besides, a long stay makes a patient more critical. In addition, longer hospital stays are generally associated with more serious illnesses, which reduce the degree of satisfaction. In a study on walk-in general medicine clinic in the United States, it was reported that while 52% of the patients were fully satisfied with their care after the outpatient visit, this rose to 59% at 2 weeks.[12] In the same vein, in a study from Saudi Arabia, it was reported that patients attending outpatient clinics had higher satisfaction scores than inpatients.[26] Unlike inpatients, walk-in outpatients were more likely to have less severe illnesses and symptoms that are quickly resolved, which probably increases satisfaction.
It should be noted that our satisfaction rates were very high in comparison with reputable international centers and might carry undetermined biases. Indeed, the patient population in our institution is very homogeneous (mostly National Guard members and their families) who could only get medical care in National Guard facilities. We can speculate that they were careful in selecting their answers on satisfaction questions. Furthermore, with the high illiteracy rate, it is safe to say that these patients might have had difficulty differentiating a scientific survey conducted by a research coordinator from audit conducted by an authority figure. Our findings should be further investigated in future prospective studies.
Using multivariate analysis, we found no independent effect on overall doctors’ response on account of age or educational level, but there was an independent effect by gender (P = 0.000) and department (P = 0.05). For the overall response on nurses, the only independent factor was department (P = 0.025) and for center score; gender was the only independent factor influencing response (P= 0.004)
CONCLUSION
There was good satisfaction in a tertiary care university hospital that advocates patient centeredness as a central part of its strategy. The factors that affected satisfaction positively were the female gender, being in the obstetrics service, and shorter LOS. Age, educational level, paying for treatment, and nationality had no impact on satisfaction.
Although the results indicate an overall good satisfaction score, it is necessary to find out why the “reception” experience failed to achieve similar level of satisfaction. All avenues should be explored to find out what could be done to improve the ambiance of the rooms.
We need to examine what we can learn from the higher satisfaction levels—particularly for doctors—among female patients. We also need to investigate why satisfaction levels were lowest in the surgical wards and with longer LOS.
ACKNOWLEDGMENT
All authors would like to thank Mr. Hani Fannoush for his valuable contribution.
Footnotes
Source of Support: Nil,
Conflict of Interest: Nil.
REFERENCES
- 1.Stewart M, Brown JB, Donner A, McWhinney I, Oates J, Weston W, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49:796–804. [PubMed] [Google Scholar]
- 2.Scotti DJ, Harmon J, Behson SJ. Links among high-performance work environment, service quality, and customer satisfaction: An extension to the healthcare sector. J Healthc Manag. 2007;52:109–24. [PubMed] [Google Scholar]
- 3.Glickman SW, Baggett KA, Krubert CG, Peterson ED, Schulman KA. Promoting quality: The health care organization from a management perspective. Int J Qual Health Care. 2007;19:341–8. doi: 10.1093/intqhc/mzm047. [DOI] [PubMed] [Google Scholar]
- 4.Vahey DC, Aiken LH, Sloane DM, Clarke SP, Vargas D. Nurse burnout and patient satisfaction. Medical Care. 2004;42(2 Suppl):II57–66. doi: 10.1097/01.mlr.0000109126.50398.5a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Argentero P, Dell’Olivo B, Ferretti MS. Staff burnout and patient satisfaction with the quality of dialysis care. Am J Kidney Dis. 2008;51:80–92. doi: 10.1053/j.ajkd.2007.09.011. [DOI] [PubMed] [Google Scholar]
- 6.Cowing M, Davino-Ramaya C, Ramaya K, Szmerekovsky J. Health care delivery performance: Service, outcomes, and resource stewardship. Perm J. 2009;13:72–8. doi: 10.7812/tpp/08-100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berenson RA, Cassel CK. Consumer-driven health care may not be what patients need–caveat emptor. JAMA. 2009;301:321–3. doi: 10.1001/jama.2008.994. [DOI] [PubMed] [Google Scholar]
- 8.Cohen RA, Martinez ME. Consumer-directed health care for persons under 65 years of age with private health insurance: United States, 2007. NCHS Data Brief. 2009;15:1–8. [PubMed] [Google Scholar]
- 9.Hibbard JH, Greene J, Tusler M. Plan design and active involvement of consumers in their own health and healthcare. Am J Manag Care. 2008;14:729–36. [PubMed] [Google Scholar]
- 10.Fung CH, Lim YW, Mattke S, Damberg C, Shekelle PG. Systematic review: The evidence that publishing patient care performance data improves quality of care. Ann Intern Med. 2008;148:111–23. doi: 10.7326/0003-4819-148-2-200801150-00006. [DOI] [PubMed] [Google Scholar]
- 11.Pitrou I, Lecourt A, Bailly L, Brousse B, Dauchet L, Ladner J. Waiting time and assessment of patient satisfaction in a large reference emergency department: A prospective cohort study, France. Eur J Emerg Med. 2009;16:177–82. doi: 10.1097/MEJ.0b013e32831016a6. [DOI] [PubMed] [Google Scholar]
- 12.Jackson JL, Chamberlin J, Kroenke K. Predictors of patient satisfaction. Soc Sci Med. 2001;52:609–20. doi: 10.1016/s0277-9536(00)00164-7. [DOI] [PubMed] [Google Scholar]
- 13.Kleefstra SM, Kool RB, Veldkamp CM, Winters-van-der MA, Mens M, Blijham G, et al. A core questionnaire for the assessment of patient satisfaction in academic hospitals in The Netherlands: development and first results in a nationwide study. Qual Saf Health Care. 2010;19:e24. doi: 10.1136/qshc.2008.030825. [DOI] [PubMed] [Google Scholar]
- 14.Goldstein E, Farquhar M, Crofton C, Darby C, Garfinkel S. Measuring hospital care from the patients’ perspective: An overview of the CAHPS hospital survey development process. Health Serv Res. 2005;40:1977–95. doi: 10.1111/j.1475-6773.2005.00477.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.US HHS US Department of Health and Human Resources. [last accessed on 2010 Sept 5]. Available from: http://www.hospitalcompare.hhs.gov/Graphs/hospital-Graph.aspx?hid=240061,240010,161318andstype=GENERALandmCode=HCAHPSandgraphState=MNandtab=HCAHPSandAspxAutoDetectCookieSupport=1 .
- 16.Comstock LM, Hooper EM, Goodwin JM, Goodwin J. Physician behaviors that correlate with patient satisfaction. J Med Educ. 1982;57:105–12. doi: 10.1097/00001888-198202000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Schmittdiel J, Grumbach K, Selby JV, Quesenberry C. Effect of Physician and Patient Gender Concordance on Patient Satisfaction and Preventive Care Practices. J Gen Intern Med. 2000;15:761–9. doi: 10.1046/j.1525-1497.2000.91156.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Al-Doghaither AH. Inpatient satisfaction with physician services at King Khalid University Hospital, Riyadh, Saudi Arabia. East Mediterr Health J. 2004;10:358–64. [PubMed] [Google Scholar]
- 19.Nohara M, Miyagi S. Family support and quality of life of pregnant women during pregnancy and after birth. Nippon Koshu Eisei Zasshi. 2009;56:849–62. [PubMed] [Google Scholar]
- 20.Langer A, Campero L, Garcia C, Reynoso S. Effects of psychosocial support during labour and childbirth on breastfeeding, medical interventions, and mothers’ wellbeing in a Mexican public hospital: A randomised clinical trial. Br J Obstet Gynaecol. 1998;105:1056–63. doi: 10.1111/j.1471-0528.1998.tb09936.x. [DOI] [PubMed] [Google Scholar]
- 21.Mulder PJ, Johnson TS. The Beginning Breastfeeding Survey: Measuring mothers’ perceptions of breastfeeding effectiveness during the postpartum hospitalization. Res Nurs Health. 2010;33:329–44. doi: 10.1002/nur.20384. [DOI] [PubMed] [Google Scholar]
- 22.Carmel S, Halevy J. Patient satisfaction and hospital services evaluation: Comparison of and private patients. Harefuah. 1999;137:363–70. [PubMed] [Google Scholar]
- 23.Al-Doghaither AH, Abdelrhman BM, Saeed AA, Magzoub ME. Factors influencing patient choice of hospitals in Riyadh, Saudi Arabia. J R Soc Promot Health. 2003;123:105–9. doi: 10.1177/146642400312300215. [DOI] [PubMed] [Google Scholar]
- 24.Alaiban KM, Al-Omar B, Narine L, Al-Assaf AF, Javed F. A survey assessing patient satisfaction at public and private healthcare facilities in Riyadh, Saudi Arabia. Ann Saudi Med. 2003;23:417–9. doi: 10.5144/0256-4947.2003.417. [DOI] [PubMed] [Google Scholar]
- 25.Nguyen Thi PL, Lê TG, Empereur F, Briançon S. Satisfaction of patients hospitalized in Ho Chi Minh City, Vietnam. Sante Publique. 2002;14:345–60. [PubMed] [Google Scholar]
- 26.Saeed AA, Mohammed BA, Magzoub ME, Al-Doghaither AH. Satisfaction and correlates of patients’ satisfaction with physicians’ services in primary health care centers. Saudi Med J. 2001;22:262–7. [PubMed] [Google Scholar]