

Abstract
Context:
Health promotion is the most important element of primary health care. Therefore, it is essential for the health team to apply such activity.
Objective:
To describe a newly established health promotion clinic at primary health care centers, in Abha city, KSA.
Materials and Methods:
The study was conducted during the year 2009. The files of 429 individuals were reviewed after one year from attending the health promotion clinics in Abha city, KSA. Master sheet was designed based on the relevant items of the file. The health promotion services used in the study were based on the recommendation of the relevant guidelines. Data entry and analysis was carried out using Statistical Program for the Social Sciences (SPSS). P-values less than 0.05 were selected for statistical significance.
Results:
After one year, the percentage of the individuals who intake imbalanced diet and did not perform any type of physical activity was more than 90% while 8% are currently smokers and 14% had depression. Clinical examination and investigation revealed that more than one quarter of our subjects were overweight. Obesity was 42% in males versus 51% in females (P<0.04). Pre-hypertension and hypertension were detected among 44 and 12% respectively. About one fifth of our subjects had pre-diabetes 21% and 3% were confirmed to have diabetes mellitus. Diet and physical activity counseling was given to all participants while referral to concerned clinics was done for individuals who suffer from high blood sugar, abnormal lipid profile, obesity and depression.
Conclusion:
This study demonstrated that health promotion clinics provided by trained professional health care team can be used as a new approach for early detection and management of the common health problems in primary health care centers.
Keywords: Health promotion, primary health care center, services
INTRODUCTION
Health promotion is one important element of primary health care and family practice.[1] It could be defined as the process of enabling individuals to practice the healthy behaviors in order to keep individuals in healthy status.[2] To have healthy community, individuals should be provided with relevant knowledge and skills to practice healthy attitude and behaviors. Health promotion is based on three pillars: positive attitude of community, availability of resources and skillful people.[2] Most of the people in Saudi Arabia are young with average survival expectancy of 73 years.[3] However, this community was found to be physically inactive,[4] has high prevalence of obesity, hypertension, diabetes and hyperlipidemia.[5–8] Those problems arise as a result of sedentary life and western life styles behaviors particularly in taking fast food, high calories and fatty meals.[4,6]
To reduce the burden of these serious problems and their sequels, it is very vital to implement health promotion programs in the community through the huge network of PHC centers as the first gate for health services in the Kingdom. The current practice of health promotion include immunization, well baby care and antenatal care services,[9] but there is no established program for periodic health examination or screening for adults in spite of good evidence for practicing many preventive measures such as screening for hypertension, diabetes, obesity, some tumors and chronic infections.[10–12]
The objective of the current study is to describe a newly established health promotion clinic in Abha city after one year of implementation at PHC centers.
MATERIALS AND METHODS
This descriptive study involved reviewing all records of people attending health promotion clinics at Abha City, the capital of Aseer region, southwest Saudi Arabia. The total population of Abha city is estimated to be 150,000 inhabitants. They are served through six PHC centers and few private dispensaries. All Saudis could get preventive and curative services from those PHC centers free of charge. The health promotion services include screening (history, physical examination, and investigation), counseling, immunization and chemoprophylaxis based on the recommendation of the relevant guidelines.[10,11] Training course was conducted to provide the physicians and nurses with relevant knowledge and skills that enable them for implementation. This course consisted of two lectures regarding the principles and role of health promotion in PHC and practical training through three workshops about communication skills, counseling skills and how to approach health promotion in different age groups. The training course was conducted under the supervision of two researchers. One clinic in each center was equipped with essential items (weight scale, stethoscope, sphygmomanometer, health education materials, registers and special files). In order to make the clinic consumers aware about these services, all PHC centers announced through medical record departments, posters attached to all clinics in the centers and distribution of many pamphlets for all attendants to primary care centers. To make our services as practical as possible, special file was designed for this purpose. The file consists of three pages: the first one was for the relevant bio-data and history including risk factors, the second page included the list of recommendations according to age group while the third page contained the clinical findings, management and future plan. After one year, we evaluated the process of care by reviewing all the relevant files. Master sheet was designed based on the items of the file. Regarding diagnostic criteria, we depended on that criteria used by relevant guidelines as following: Overweight is considered if the body mass index is 25-29.9 kg/m2, obesity if BMI≥30 kg/m2. Prehypertension (BP=120-139/80-89 mmHg, hypertension (BP≥140/90 mmHg). Pre-diabetes (fasting blood=100-125 mg/dl, Diabetes (fasting blood glucose≥126 mg/dl on two separate occasions). Hypercholesterolemia was diagnosed if fasting plasma cholesterol was≥200 mg/dl. Depression was screened by question regarding mood and anhedonia over the past two weeks and those with positive test was confirmed according to Diagnostic Statistical Manual (DSM-IV).Individuals who were found to have high blood sugar, abnormal lipid profile, obesity and depression were referred to chronic diseases clinics at the concerned PHC centers for further management and follow up.
The relevant data were coded, entered and analyzed by using SPSS version 15. Descriptive statistics (mean, standard deviation and percentage) were used to quantify the study and outcome variables. Chi-square test and student's t test were used to observe the association between categorical variables. P-value of less than 0.05 was considered as statistically significant.
RESULTS
The total number of attendants who came to health promotion clinics was 429. Their mean (SD) age was 36.2 (13.6) years. Males and females attended almost equal, 50.6 and 49.4% respectively. Most of the attendees were married (69%), about one third (32.4%) was housewives, 25% were students and the majority (79%) was educated with secondary and university level as shown in Table 1.
Table 1.
Socio-demographic characteristic of individuals attending health promotion clinics, Aseer, 2009
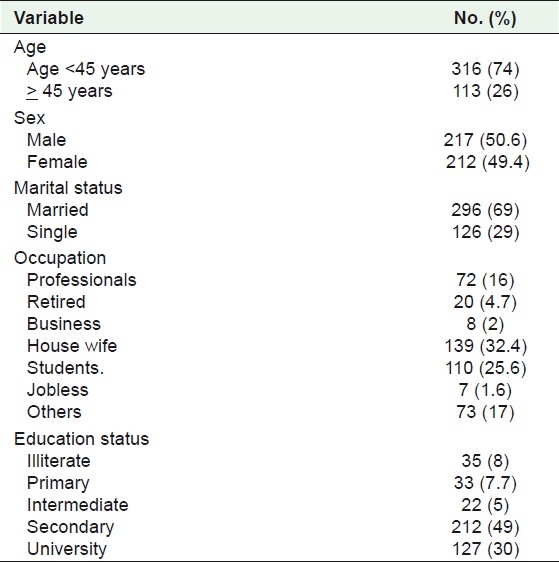
Table 2 shows the number and percentage of each risk factor among attendees. More than 90% intake imbalanced diet that is rich in saturated fat and carbohydrates, almost all participants did not perform any type of physical activity while 8% are currently smokers. Depression was detected among 14% of participants.
Table 2.
Patterns of risk factors/morbidities detected among attendants of health promotion clinics
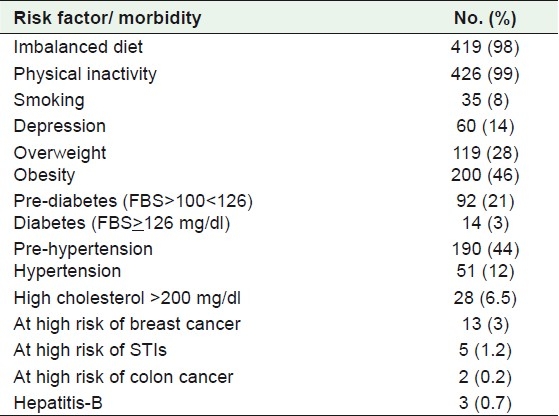
Clinical examination and investigations revealed that more than one fourth suffers from overweight and 46% had obesity. Pre-hypertension and hypertension were detected among 44 and 12% respectively. About one fifth was found to have pre-diabetes (21%) and 3% were confirmed to have diabetes mellitus.
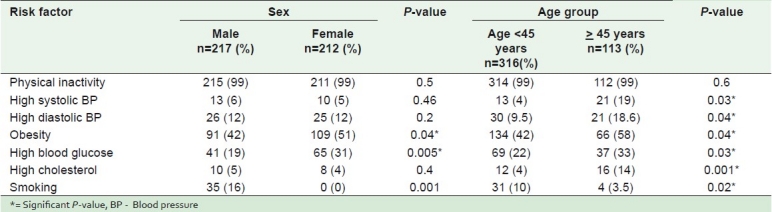
Table 3 illustrates the association between independent variables (gender, age group) and dependant variables (risk factors). There was a high percentage with significant statistical difference of obesity (P=0.04) and high fasting blood glucose (P=0.005) among females. Regarding age group, it was found that those above 45 years old had high percentage with significant statistical difference of hypertension(P=0.04), obesity(P=0.04), high glucose(P=0.03) and cholesterol(P=0.001). On the other hand, those younger than 45 years smoke more than those above 45 years old(P=0.02). Depression was more among males (15% vs 13%) but insignificant (P=0.4), married than single (16.5% vs 8%) but insignificant (P=0.07), smoker than non-smoker (31% vs 12%, P=0.004). Regarding the other independent variables (marital status, occupation and education) there was no significant association with the risk factors (P>0.05).
Table 3.
Percentage of modifiable CHD risk factors according to sex and age group among attendants of health promotion clinics
All participants were counseled about the well balanced diet and physical activities. Different vaccines (e.g. influenza) were given to about 13%, while all smokers were counseled about cessation of smoking then given follow up in the smoking cessation clinic for further intervention and follow up. Aspirin and folic acid were prescribed for 6 and 2% of attendants respectively.
DISCUSSION
Health promotion is considered as one of the most cost-effective methods of practicing preventive measures in the community. It stresses on the vital roles of individuals, families and community concerning healthy behavior to maintain good health and control diseases.[1]
To our knowledge, this is the first report from Aseer region dealing with adults’ health promotion services introduced through primary health care settings.
In this study, it is obvious that all adult age groups and both sexes and jobs attended the clinics equally which reflects the good response of community to this initiative. Most of the participants had unhealthy life styles such as in taking imbalanced diet and physical activities. These findings are in agreement with those reported by Al-Hazzaa, in which the physical inactivity ranged from 43.3% to 99.5%.[4]
Although smoking is a major problem in Saudi Arabia, ranging from 2.4 to 52.3%,[13] only 8% was reported as male smokers in the current study. This low figure may be due to better awareness of the smoking hazards by the community in Aseer region.
Our results revealed high percentage of obesity and overweight among the participants (46%, 28%),which is higher than the report published by Al-Nozha et al (35.5% for obesity and 36.9% for overweight).[6] This major problem was higher among women and those above 45 years old who are at high risk of coronary heart disease. Contributing factors for this common morbidity include lack of regular exercise and imbalanced diet which were reported by 99 and 98% of attendants respectively. To overcome this serious problem, it is necessary to screen for obesity and to conduct counseling for those with BMI>25kg/m2.
In the present study, it was found that pre-diabetes percentage was about 21% while diabetes was (3%) among asymptomatic individuals. These figures indicate that our community has high proportion of individuals with high risk to develop diabetes which mandate the periodic checking for diabetes. The low percentage of diabetes in this study compared with other published study[7] could be due to the difference in the methodology and the age groups.
The other important health problems detected was hypertension. It was found that (12 %) had persistent hypertension. This figure was less than reported by Al-Nozha et al (26%).The percentage of pre-hypertension was very high (44%) compared to those reported by Al-Asmary et al (17.3%) and A-Zahrani (18%).[14,15] These findings indicate the importance of regular check- up of blood pressure as recommended recently by national organization.[16]
Percentage of high cholesterol was low (6.5%) compared to previous studies.[8,17] This low figure is very difficult to explain in presence of high percentage of other contributing factors such as unhealthy diet, sedentary life, diabetes, obesity and hypertension, but it may be due to the young age of our participants, the mean (SD) age was 36.2 (13.6) years.
Most of the participants were found to have more than three or more risk factors for coronary heart diseases (73% among males and 69% among females). These multiple risk factors should be managed appropriately in order to minimize the heart attacks and strokes.
The percentage of depression was about 14%. This figure is lower than that reported from Riyadh (28.5%) and Kuwait (37%).[18,19] In our community, it is difficult to diagnose depression due its vague symptoms and reluctancy to attend to psychiatric hospital. These facts indicate the importance of health promotion clinics to detect such common psychiatric disorder in our community.
Different interventions were done to care for attendees. All participants were counseled about healthy diet, exercise. Smokers were given counseling about smoking cessation and those with high risk for communicable diseases were counseled and referred to the concerned specialists accordingly. Drugs were prescribed for those in need such as patients with depression or those needs vaccines or aspirin for primary or secondary preventions.
CONCLUSION
In the light of the findings of the present study, it is concluded that the people attending health promotion clinics at Abha City were suffering from asymptomatic health problems such as diabetes, hypertension, obesity and depression. The findings point to the need for the health promotion clinic as a new approach for early detection and management of the common health problems in PHC centers.
ACKNOWLEDGMENT
My special thanks to the administration and staff of Joint program of Family Medicine, Aseer region in facilitating this work.
Footnotes
Source of Support: Nil,
Conflict of Interest: Nil.
REFERENCES
- 1.Al-Gelban KS, Al-Khaldi YM, Diab MM. 2nd ed. USA: Trafford Publishing; 2010. Family Medicine A Practical Approach; pp. 105–50. [Google Scholar]
- 2.World Health Organization, Regional office for Eastern Mediterranean Region. A strategy for Health Promotion in Eastern Mediterranean Region-2006-2013. WHO-EM/HLP/036/E: 9-23. [Google Scholar]
- 3.Review of the Health Situation. Ministry of Health. Health Statistical Book for the year 2008; pp. 31–4. [Google Scholar]
- 4.Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: A brief review. East Mediterr Health J. 2004;10:663–70. [PubMed] [Google Scholar]
- 5.Al-Nozha MM, Al-Mazrou YY, Al-Maatouq MA, Arafah MR, Khalil MZ, Khan AH, et al. Obesity in Saudi Arabia. Saudi Med J. 2005;26:824–9. [PubMed] [Google Scholar]
- 6.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou Y, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28:77–84. [PubMed] [Google Scholar]
- 7.Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS, Arafah MR, Khalil MZ, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25:1603–10. [PubMed] [Google Scholar]
- 8.Al-Nozha MM, Al-Mazrou, Arafah MR, Al-Maatouq MA, Khalil MZ, Khan Al-Marzouki K, et al. Hyperlipidemia in Saudi Arabia. Saudi Med J. 2008;29:282–7. [PubMed] [Google Scholar]
- 9.Quality assurance in primary health care manual. Riyadh, Saudi Arabia: Ministry of Health and World health Organization Regional office for Eastern Mediterranean; 1994. The scientific committee of quality assurance in primary health care; pp. 71–128. 241-314. [Google Scholar]
- 10.US Preventive Services Task Force. Guide to clinical preventive services. 2009. [Last accessed on 2010 Dec 26]. Available from: http://www.uspreventiveservicestaskforce.org/
- 11.The Royal Australian College of General Practitioners. South Melbourne, Victoria: Palmerston Crescent; 2009. Guidelines for preventive activities in general practice; pp. 22–6. [Google Scholar]
- 12.American diabetes Association. Standards of medical care in diabetes-2009. Diabetes care. 2009;32(Suppl 1):13–49. [PubMed] [Google Scholar]
- 13.Bassiony M. Smoking in Saudi Arabia. Saudi Med J. 2009;30:876–81. [PubMed] [Google Scholar]
- 14.Al-Asmary SM, Al-Shehri AA, Farahat FM, Abdel-Fattah MM, Al-Shahrani MM, Al-Omari FK, et al. Community- based screening for pre-hypertension among military active duty personnel. Saudi Med J. 2008;29:1779–84. [PubMed] [Google Scholar]
- 15.Al-Zahrani MS. Prehypertension and undiagnosed hypertension in a sample of dental school female patients. Int J Dent Hyg. 2011;9:74–8. doi: 10.1111/j.1601-5037.2009.00441.x. [DOI] [PubMed] [Google Scholar]
- 16.Saudi Hypertension Management Group and National Commission for Hypertension. Saudi Hypertension Management guidelines. 2007 [Google Scholar]
- 17.Al-Humaidi MA, Suleiman SA, Abolfotouh MA, Khattab MS, Al-Kadomi OF, Al-Khaldi Y, et al. Hypercholesterolemia and other risk factors of coronary artery disease among patients of primary health care centers(PHCCs) in southwest Saudi Arabia. J Bahrain Med Soc. 1999;11:15–22. [Google Scholar]
- 18.Abdel-Rahman A, Asal, Abdel-Fattah MM. Prevalence, symptomatology, and risk factors for depression among high school students in Saudi Arabia. Neurosciences. 2007;12:8–16. [PubMed] [Google Scholar]
- 19.Al-Otaibi B, Al-Weqayyan A, Taher A, Sarkhou E, Gloom A, Aseeri F, et al. Depressive Symptoms among Kuwaiti population attending primary health care setting: Prevalence and influence of socio demographic factors. Med Princ Pract. 2007;16:384–8. doi: 10.1159/000104813. [DOI] [PubMed] [Google Scholar]