

Abstract
Objective:
To measure the radiation exposure to nuclear medicine personnel during synthesis and injection to the patients of Ga-68 1,4,7,10-tetraazacyclododecane-N,N′,N″,N″′-tetraacetic acid (DOTA)-1-Nal3-octreotide (NOC)- (DOTA-NOC) using ring thermoluminescence dosimeters (TLDs).
Materials and Methods:
Synthesis of Ga-68 DOTA-NOC was done on a semi-automated system. Finger doses were measured during synthesis and injection of Ga-68 DOTA-NOC. The occupational workers wore TLDs at the base of ring finger of both hands. The finger doses of two radio chemists were measured during synthesis of Ga-68 DOTA-NOC while that of a physician during its injection to the patients.
Results:
Duration of the study was eight months and a total of 20 samples were prepared. During synthesis, the mean dose to base of left ring finger was 3.02 ± 1.01 mSv and to base of right ring finger was 1.96 ± 0.86 mSv. Mean dose to base of left ring finger was 1.26 ± 0.35 mSv while that to base of right ring finger was 1.03 ± 0.13 mSv during injection. The mean dose was observed to be higher during synthesis than injection. However, the difference was not significant (P = 0.27 and P = 0.18, respectively). Overall mean finger dose of left hand was 2.43 ± 1.21 mSv, whereas for the right hand the same was 1.65± 0.82 mSv.
Conclusion:
Finger doses to radio chemists during semi-automated synthesis of Ga-68 DOTA-NOC and that to the physician involved in injection of Ga-68 DOTA-NOC were found to be within permissible limits. Ring dosimeters must be worn for the safety of the nuclear medicine personnel involved in synthesis and injection of Ga-68 DOTA-NOC.
Keywords: Ga-68 DOTA-NOC, radiation dose, ring dosimeter, TLD
INTRODUCTION
Expressions of SSTR subtype 2 (SSTR-2) has been found in various human neuroendocrine tumors (NETs).[1] Somatostatin receptor scintigraphy (SRS) has been integrated into the diagnostic work-up of patients with neuroendocrine tumors (NET).[2] However, significant rate of false negative results was observed with conventional SRS using 111In-diethylenetriaminepentaacetic acid (DTPA)-octreotide, with sensitivities ranging between 55%-75%.[3–6] This lower sensitivity may be attributed to inherently lower spatial resolution of single photon emitted computed tomography (SPECT) as compared to positron emission tomography (PET). These findings attracted the attention of researchers to develop peptides labeled with positron emitters. Among these, Ga-68 labeled peptide (DOTA-TOC, DOTA-NOC, DOTA-TATE) deserves special attention,[1,3,7] because it is Ge-68/Ga-68 generator produced which obviates the use of cyclotron. In a recent study, Ambrosini et al have confirmed that Ga-68 DOTA-NOC PET/CT could change the management in a significant number of NET patients.[8]
The parent Ge-68 has long half-life of 270.8 days, which allows use of the generator for one year or longer. The Ga-68 radio pharmacy is independent of an onsite medical cyclotron facility. Ga-68 has a half-life (t½) of 67.7 min and it decays by 89% through positron emission (βmax. 1.92 MeV) and 11% orbital electron capture.[9] Handling of high gamma photon energy (511 keV) leads to higher radiation dose to occupational workers as compared to conventional Tc-99m/In-111 based radiopharmaceuticals. Several studies have been reported on radiation dose to technologist working with F-18 Flurodeoxyglucose (FDG).[10,11] However, similar studies are lacking in the field of Ga-68 peptide imaging. Evaluation of radiation dose to occupational workers involved in synthesis and injection is vital as Ga-68 labeled peptide synthesis takes relatively longer time of about 20 minutes.[12] Though a dosimetric study using Ga-68 DOTA-NOC in NET patients was reported by Pettinato et al,[13] till date no study has evaluated radiation dose to personnel involved in synthesis and injection of Ga-68 DOTA-NOC. It is an essential part of the regulatory, as well as good practice, to have the information on the finger dosimetry for this agent during synthesis and injection. Thermoluminescence dosimeters (TLDs) are used to measure radiation doses to the fingers of staff involved in handling radioactivity.[14,15] At our institute, occupational workers are always monitored for their effective whole body doses by using chest and extremities doses by using wrist TLD badges.
In the present study, we measured equivalent doses to fingers of two radio chemists during synthesis and a physician during injection of Ga-68 DOTA-NOC. Dosimetry study was carried out to verify and to demonstrate compliance with the regulatory prescribed dose limits (500mSv/y).
MATERIALS AND METHODS
This was a prospective study and approved by institutional review board. The study was carried out between December 2006 and July 2007. Our experimental work was two-fold. First, we sought to find the annealing temperature of TL pellets during standardization of pellets. Second, we sought to find the finger doses during synthesis (radio chemists- synthesis group), and injection (physician-injection or dose administration group) of Ga-68 DOTA-NOC.
Ge-68/Ga-68 generator and Ga-68 DOTA-NOC synthesis
Commercial Ge-68/Ga-68 radionuclide generator (50 mCi/1.85 GBq) based on TiO2 column was obtained from Cyclotron Co. Ltd, Obininsk, Russia. Ga-68 DOTA-NOC was syn-thesised as described in the literature and is briefly summarised here.[12] 50mCi, Ge-68/Ga-68 generator was eluted using 0.1 M HCl. The eluent was loaded onto a cation exchange cartridge to pre concentrate and pre purify (using 80% acetone/0.15 M HCL). Purified Ga-68 (half-life, 68.3 min) was directly eluted with 97.7% acetone/0.05 M HCL into the reaction vial containing 30-50 μg of DOTA-NOC. Synthesis was carried out at approximately 100-126°C for 10-15 minutes. This was followed by removal of labelled peptide from unlabelled peptide using reverse phase C-18 column, using 400 μl of ethanol. This was further diluted with normal saline and passed through 0.22 μm filter to get sterile preparation for injection.
Standardization of TL pellets and dose measurements
Ring dosimeters consisting of thermoluminiscent (TL) pellets (CaSO4:Dy) measuring 4.5 mm in diameter and 0.9 mm in thickness were used in this study for measuring finger doses during the preparation and dose administration of Ga-68 DOTA-NOC [Figure 1]. TL was recorded on Harshaw Model 3500 TLD reader (Thermo Fisher Scientific Inc., Erlangen, Germany) which is capable of recording TL upto 400°C. Thermolyne model 47900 box furnace (Barnstead/Thermolyne Corp., IA, USA) (0-1200°C) was used for annealing. Radioactive wastes generated during the work were stored properly for decay to near background level. Radiation dose was measured using TL pellets (ring dosimetry) in the base of ring finger in both hands. Duration of the study was eight months and a total of 20 samples were prepared. Synthesis was done on a semi-automated system according to method described elsewhere.[12]
Figure 1.
(a) Ring dosimeters; (b) TL pellet (CaSO4: Dy) used in ring dosimeter
Initially, 64 TL pellets were used for standardization. All pellets were irradiated to known amount of exposure and were read in TLD reader. Those having dose variations more than 5% were discarded. Twenty TL pellets having dose variations within ±5 % and were used for the study. To find appropriate annealing temperature, all 20 TL pellets were annealed for two hours at 200°C and were irradiated with 100 mCi of F-18 FDG for 1 hour. Same pellets were again annealed for 2 hour at 400°C and then irradiated with 100 mCi of F-18 FDG for 1 hour. Response was recorded with respect to dose using the TLD reader. Annealed TL pellets were kept in a circular bowl and then irradiated with Cs-137 (dose rate: 1.13mGy/ h). Keeping heating rate at 1°C/ sec, the TL of samples was taken immediately. Data was recorded for each pellets and glow curve were found for each. A typical glow curve is shown of CaSO4: Dy used in this study [Figure 2].
Figure 2.
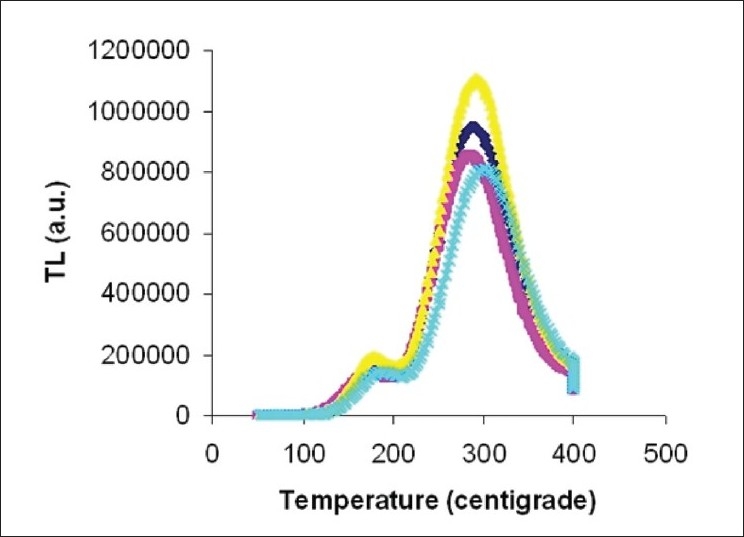
Glow curve of CaSO4: Dy TL pellets, showing four peaks of Ga-68 DOTA-NOC exposure of TLD (a.u- arbitrary units)
Injection of Ga-68 DOTA-NOC
After preparation of Ga-68 DOTA-NOC, the physician injected 111-222 MBq (3-6 mCi) of Ga-68 DOTA-NOC through an intravenous cannula. During the injection, the physician followed the time, distance and shielding approach to minimize the radiation exposure. The time of contact with the patients was kept to a minimum. The patients were taken for PET/CT, 30-45 minutes after radiotracer injection.
Radiation doses to fingers
The TL pellets were inserted in a plastic ring holder that could be adjusted for any finger size. The occupational workers wore them at the base of ring finger of both hands during synthesis and dose administration. In our study ring finger was chosen to wear ring dosimeters as it was convenient during synthesis as well as dose administration and also it gives good estimation of dose.[16,17]TLDs were kept in a low-background-radiation area when not in use.
In this study, the occupational workers were divided into two groups: Group 1 or the synthesis group (consisting of two radio chemists) and Group 2 or the injection/dose administration group (consisting of a physician). The nature of work of group 1 was different from that of group 2. Finger doses were measured in two groups, and in each group two measurements were taken. These measurements were considered as independent samples. The finger doses of group 1 were estimated during synthesis while that of group 2 were estimated during injection of Ga-68 DOTA-NOC.
While wearing the ring dosimeters, none of the workers used a syringe shield during handling radioactivity. Although the use of a syringe shield is recommended from a radiation safety standpoint, it is not mandatory in India. A control ring was kept in a low-background-radiation area for measuring the background response of the TLD. The TL pellets exposed to Ga-68 DOTA-NOC were placed in the TLD reader to obtain their response in relation to radiation dose. Results of TLD reader were recorded as a unit of charge [(nanocoulomb/ microcoulomb (nC/μC)] and then converted to unit of dose (mSv/μSv). The radiation weighting factor for the γ-photons Ga-68 was taken as 1. The TL pellets were given numbers to maintain their identity throughout the work.
Statistical analysis
In the descriptive analysis, doses were reported as mean ± standard deviation (SD). Coefficient of variation was calculated using [SD/mean]*100 for observing dose variation at different temperatures. Due to small sample size, non-parametric tests were used for comparisons. Kruskal Wallis test was used to compare the dose to the base of left ring finger and right hand finger between the two groups (radio chemists and physician). Comparison was also made between the workers within a group (e.g. radio chemist 1 and 2). For post hoc analysis, Mann-Whitney test was applied between group 1 and group 2. To observe the change of dose to left ring finger and right ring finger between the groups, Wilcoxon signed rank test was applied. A P < 0.05 was considered as significant. All statistical analysis was carried out using SPSS 15 (SPSS Inc., Illinois, USA).
RESULTS
Optimal annealing temperature of TL pellets
In our study, it was observed that the coefficient of variation of TL pellets during annealing was 8.18 at 400°C which was less compared to 35.44 at 200°C. Hence, the optimum temperature for annealing was considered as 400°C.
Radiation doses to fingers
It was observed that the mean finger dose was higher to left ring finger base for radio chemist 1 (P = 0.18), whereas dose was observed higher to right finger base for radio chemist 2 (P = 0.66) during synthesis. Although higher dose was observed to left ring finger than right ring finger base in physician, as shown in Table 1, the difference was not statistically significant (P = 0.18). No statistically significant difference was observed between the dose to base of left ring finger among 2 radio chemists and physician (P = 0.10). Also, no statistically significant difference in doses to right ring finger base, was seen among radio chemist 1, radio chemist 2 and physician (P = 0.37). However, if more measurements were taken the difference might have been statistically significant. Overall, physician had lower mean radiation dose than radio chemists in both hands Table 1.
Table 1.
Finger doses to nuclear medicine personnel during handling Ga-68 DOTA-NOC

The mean finger dose to base of left ring finger was observed 3.02 ± 1.01 mSv and to the base of right ring finger was 1.96 ± 0.86 mSv during synthesis i.e. group 1, as shown in Table 2. Mean dose to base of left ring finger was observed 1.26 ± 0.35 mSv while that to the base of right ring finger was 1.03 ± 0.13 mSv during injection i.e. group 2 [Figure 3]. The mean dose observed was higher during synthesis than during injection [Figure 3]. Also, mean dose was higher for left hand in both synthesis and injection group. However, the difference was not significant in either group (P = 0.27 and P = 0.18, respectively). The difference was near significant (P = 0.06) higher in left hand for synthesis group in comparison to injection group. However, no significant (P = 0.35) difference was found in right hand in both groups. Overall mean finger dose of left hand was 2.43± 1.21 mSv whereas for right hand was 1.65 ± 0.82 mSv.
Table 2.
Finger doses in both hands ring finger base during synthesis (radio chemists) and injection (physician) groups

Figure 3.
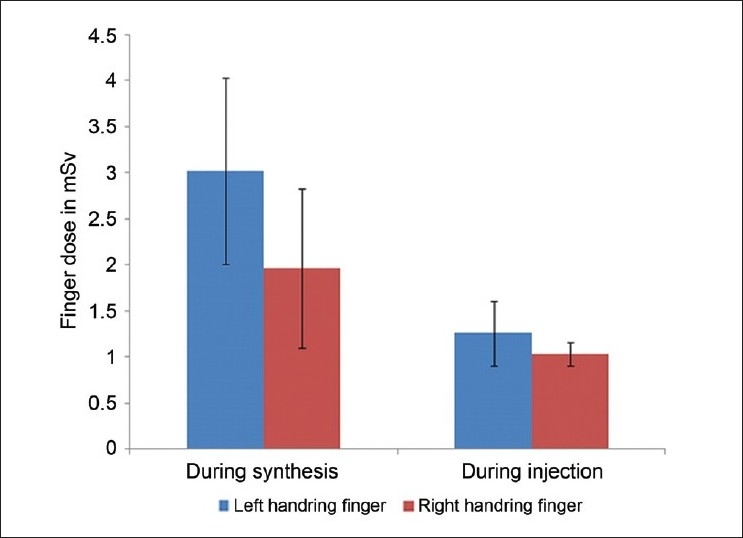
Finger doses (mSv) in both hands ring finger base during synthesis and injection
DISCUSSION
While working with radioactive substance, one is invariably subjected to radiation exposure. Internal exposure occurs due to the inhalation, ingestion, contamination through wounds. Internal radiation dosimetry deals with the determination of the amount and spatial and temporal distribution of radiation energy deposited in tissue by radionuclides within the body, while the external exposure occurs due to the radiation striking a part or whole of body. Occupational workers preparing and administering radiopharmaceuticals in nuclear medicine may receive significant radiation doses to their hands, particularly the fingers. Ring dosimeters are very useful for measuring doses at either the base or the tip of the fingers of personnel handling radioactivity.[14]
In a recent study, dosimetry of Ga-68 DOTA-NOC for patients of NETs was carried out.[18] This group has reported that Ga-68 DOTA-NOC can be used extensively for diagnosis of somatostatin receptor positive tumors as it has got many advantages over the 111In-labelled ligand. Another study has reported that the Ga-68 DOTA-TOC was found to be superior to conventional imaging, and even F-18 FDG PET/CT scanning in detecting NETs.[19] However there is paucity of literature regarding occupational exposure during synthesis of Ga-68 DOTA peptides. It is maiden attempt to prepare the finger dosimeters and do the dosimetry with Ga-68 labeled peptide (DOTA-NOC) during synthesis and injection.
In our study, CaSO4: Dy, TL pellets were used because this material has a high TL sensitivity, negligible fading effect and its dose response was observed to be linear in the range from 10-5 to 10 Gy. Our group observed that annealing temperature for CaSO4:Dy disk is 400°C for two hours which is consistent with the literature for the same material.[20] A general overview on extremity dosimeters and the dose distribution on the hands during various nuclear medicine procedures are discussed elsewhere.[21] In our study, location of ring dosimeters was ring finger base as suggested by previous studies.[18,19] Several groups have used syringe shield in order to minimize radiation doses to fingers.[22,23] However, syringe shield is not mandatory in India. We didn’t use syringe shield in present study. In our setup, it is a regular practice to use short-tubing butterfly cannula inserted into the vein of patients before radiopharmaceutical administration, which also reduces the dose to finger during injection as reported in literature.[24]
For all personnel involved in this study, overall mean dose of left hand was 2.43 ± 1.21 mSv whereas that for right hand was 1.65 ± 0.82 mSv that might cross the annual limit of 500 mSv if the same person continued to perform the same type of work throughout the year. Therefore, it is suggested that occupational workers should work on rotation. If more than one synthesis is required on the same day different radiation worker should perform the synthesis. Similarly, physicians injecting the activity should also be on rotation to follow ALARA (as low as reasonably achievable) principle. In our study, higher finger doses were observed during synthesis of Ga-68 DOTA-NOC compared to injection, though not statistically significant. This is because the time taken for synthesis is much longer compared to the time taken during injecting the agent. However, as the radiation workers at our centre worked in shifts, it is unlikely that exposure would exceed the permissible annual limit. Automated system of synthesis for Ga-68 DOTA-NOC is currently in developing stage and its routine use may reduce the finger doses to a greater extent in future.[25] Although preparation of ring dosimeter is a cumbersome process, its use is strongly recommended under circumstances where exposure is expected to high. Finger doses can serve as a guide to suggest any needed modification in work practice to minimize radiation doses to the extremities.
The present study has certain limitations. Firstly, we measured extremity doses (hand) in regards to Ga-68 manipulation and could not examine whole body doses. Secondly, limited number of finger dose measurements was taken because of the limited amount of peptide availability, initially.
CONCLUSION
Fingers doses to radio chemists during semi-automated synthesis of Ga-68 DOTA-NOC and that to physician involved in injection of Ga-68 DOTA-NOC to the patients are within permissible limits. With use of automatic synthesis module in future there is a scope of further reduction of finger dose to radio chemist. Ring dosimeters must be worn for the safety of the nuclear medicine personnel involved in synthesis and injection of Ga-68 DOTA-NOC.
ACKNOWLEDGEMENTS
The authors would like to thank Prof. Frank Roesch, Institut fuer Kernchemie, Johannes Gutenberg-Universitaet Mainz, Germany for his valuable suggestions.
*Preliminary data presented previously at 9th AOFNMB conference and published as abstract in Indian J Nucl Med 2008;23:121.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Reubi JC. Peptide receptors as molecular targets for cancer diagnosis and therapy. Endocr Rev. 2003;24:389–427. doi: 10.1210/er.2002-0007. [DOI] [PubMed] [Google Scholar]
- 2.van Eijck CH, Kwekkeboom DJ, Krenning EP. Somatostatin receptors and breast cancer. Q J Nucl Med. 1998;42:18–25. [PubMed] [Google Scholar]
- 3.Srirajaskanthan R, Kayani I, Quigley AM, Soh J, Caplin ME, Bomanji J. The role of 68Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111In-DTPA-octreotide scintigraphy. J Nucl Med. 2010;51:875–82. doi: 10.2967/jnumed.109.066134. [DOI] [PubMed] [Google Scholar]
- 4.Gibril F, Reynolds JC, Doppman JL, Chen CC, Venzon DJ, Termanini B, et al. Somatostatin receptor scintigraphy: Its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas: A prospective study. Ann Intern Med. 1996;125:26–34. doi: 10.7326/0003-4819-125-1-199607010-00005. [DOI] [PubMed] [Google Scholar]
- 5.Krausz Y, Keidar Z, Kogan I, Even-Sapir E, Bar-Shalom R, Engel A, et al. SPECT/CT hybrid imaging with 111In-pentetreotide in assessment of neuroendocrine tumours. Clin Endocrinol (Oxf) 2003;59:565–573. doi: 10.1046/j.1365-2265.2003.01885.x. [DOI] [PubMed] [Google Scholar]
- 6.Lebtahi R, Cadiot G, Mignon M, Le Guludec D. Somatostatin receptor scintigraphy: A first-line imaging modality for gastroenteropancreatic neuroendocrine tumors. Gastroenterology. 1998;115:1025–7. [PubMed] [Google Scholar]
- 7.Hofmann M, Maecke HR, Börner AR, Weckesser E, Schöffski P, Oei ML, et al. Biokinetics and imaging with the somatostatin receptor PET radioligand 68Ga-DOTATOC: Preliminary data. Eur J Nucl Med. 2001;28:1751–7. doi: 10.1007/s002590100639. [DOI] [PubMed] [Google Scholar]
- 8.Ambrosini V, Campana D, Bodei L, Nanni C, Castellucci P, Allegri V, et al. 68Ga-DOTANOC PET/CT clinical impact in patients with neuroendocrine tumors. J Nucl Med. 2010;51:669–73. doi: 10.2967/jnumed.109.071712. [DOI] [PubMed] [Google Scholar]
- 9.Maecke HR, Hofmann M, Haberkorn U. 68Ga-labeled peptides in tumor imaging. J Nucl Med. 2005;46:172S–8S. [PubMed] [Google Scholar]
- 10.Chiesa C, De Sanctis V, Crippa F, Schiavini M, Fraigola CE, Bogni A, et al. Radiation dose to technicians per nuclear medicine procedure: Comparison between technetium-99m, gallium-67, and iodine-131 radiotracers and fluorine-18 fluorodeoxyglucose. Eur J Nucl Med. 1997;24:1380–9. doi: 10.1007/s002590050164. [DOI] [PubMed] [Google Scholar]
- 11.Benatar NA, Cronin BF, O’Doherty MJ. Radiation dose rates from patients undergoing PET: Implications for technologists and waiting areas. Eur J Nucl Med. 2000;27:583–89. doi: 10.1007/s002590050546. [DOI] [PubMed] [Google Scholar]
- 12.Zhernosekov KP, Filosofov DV, Baum RP, Aschoff P, Bihl H, Razbash AA, et al. Processing of generator-produced 68Ga for medical application. J Nucl Med. 2007;48:1741–8. doi: 10.2967/jnumed.107.040378. [DOI] [PubMed] [Google Scholar]
- 13.Pettinato C, Sarnelli A, Di Donna M, Civollani S, Nanni C, Montini G, et al. 68Ga-DOTANOC: Biodistribution and dosimetry in patients affected by neuroendocrine tumors. Eur J Nucl Med Mol Imaging. 2008;5:72–9. doi: 10.1007/s00259-007-0587-y. [DOI] [PubMed] [Google Scholar]
- 14.Williams ED, Laird EE, Forster E. Monitoring radiation dose to the hands in nuclear medicine: Location of dosimeters. Nucl Med Commun. 1987;8:499–503. doi: 10.1097/00006231-198707000-00006. [DOI] [PubMed] [Google Scholar]
- 15.Mackenzie A. Reduction of extremity doses in the radiopharmacy. Nucl Med Commun. 1997;18:578–81. doi: 10.1097/00006231-199706000-00014. [DOI] [PubMed] [Google Scholar]
- 16.Gallet JM, Reed MH. Paediatric personnel extremity dose study. Br J Radiol. 2002;75:249–52. doi: 10.1259/bjr.75.891.750249. [DOI] [PubMed] [Google Scholar]
- 17.Pant GS, Sharma SK, Rath GK. Finger doses for staff handling radiopharmaceuticals in nuclear medicine. J Nucl Med Technol. 2006;34:169–73. [PubMed] [Google Scholar]
- 18.Hartmann H, Zöphel K, Freudenberg R, Oehme L, Andreeff M, Wunderlich G, et al. Radiation exposure of patients during 68Ga-DOTATOC PET/CT examinations. Nuklearmedizin. 2009;48:201–7. doi: 10.3413/nukmed-0214. [DOI] [PubMed] [Google Scholar]
- 19.Naswa N, Bal CS, Lata S, Malhotra A, Nadig MR. Evaluation of patients with neuroendocrine tumors (NETs) by 68Gallium-DOTATOC PET/CT (GPET) J Nucl Med. 2007;48:153. [Google Scholar]
- 20.Salah N, Sahare PD. The influence of high-energy 7Li ions on the TL response and glow curve structure of CaSO4:Dy. J Phys D Appl Phys. 2006;39:26–31. [Google Scholar]
- 21.Vanhavere F, Berus D, Buls N, Covens P. The use of extremity dosemeters in a hospital environment. Radiat Prot Dosimetry. 2006;118:190–5. doi: 10.1093/rpd/ncl017. [DOI] [PubMed] [Google Scholar]
- 22.Whitby M, Martin CJ. Investigation using an advanced extremity gamma instrumentation system of options for shielding the hand during the preparation and injection of radiopharmaceuticals. J Radiol Prot. 2003;23:79–96. doi: 10.1088/0952-4746/23/1/305. [DOI] [PubMed] [Google Scholar]
- 23.Hastings DL, Hillel PG, Jeans SP, Waller ML. An assessment of finger doses received by staff while preparing and injecting radiopharmaceuticals. Nucl Med Commun. 1997;18:785–90. doi: 10.1097/00006231-199708000-00013. [DOI] [PubMed] [Google Scholar]
- 24.Batchelor S, Penfold A, Aric I, Huggins R. Radiation dose to the hands in nuclear medicine. Nucl Med Commun. 1991;12:439–44. doi: 10.1097/00006231-199105000-00008. [DOI] [PubMed] [Google Scholar]
- 25.Bauwens M, Chekol R, Vanbilloen H, Bormans G, Verbruggen A. Optimal buffer choice of the radiosynthesis of 68Ga-Dotatoc for clinical application. Nucl Med Commun. 2010;31:753–8. doi: 10.1097/MNM.0b013e32833acb99. [DOI] [PubMed] [Google Scholar]