

Abstract
Large skeletal discrepancies are sometimes only minimised but not eliminated by orthognathic surgeries. Administration of Botox has been advocated as an effective minimally invasive procedure to tackle aesthetic compromises like gummy smile and the like. This article elaborates on the surgical management of a case of severe vertical maxillary excess with Botox as an adjunct therapy.
Keywords: Gummy smile, Botox, Lefort I osteotomy
Introduction
A paramount objective of modern cosmetic surgery is improvement in facial aesthetics [1]. A major reason for seeking professional help is dissatisfaction with the facial appearance in addition to functional problems [2]. The display of excessive gingival tissue in maxilla on smiling has been described as ‘gummy smile’. Patients with excessive gingival exposure are self-conscious and embarrassed about it and some others, psychologically affected [3, 4]. Various surgical and non-surgical modalities have been described in the treatment of gummy smile which includes Lefort I osteotomy, crown lengthening procedures, maxillary incisor intrusions, microimplants, headgears, self curing silicone implant injected at ANS with myectomy and partial resection of levator labii superioris with muscle repositioning. However, these procedures do not help in reducing the hyperactivity of the muscles and therefore, non surgical treatment may be a desirable option [5].
If the gummy smile is skeletal, as in vertical maxillary excess, then, a Lefort I osteotomy is warranted. However, very large discrepancies have their surgical limitations. Horse-shoe osteotomy, a modification of Lefort I osteotomy has been described in literature to target major movements in maxilla [6]. However, it is not commonly practised.
Botox has been in clinical use since three decades for the treatment of several conditions associated with excessive muscle contraction [7] such as strabismus [8], cervical dystonia [9], blepharospasm and hemi-facial spasm [10] and the like. In the last two decades, botox has been widely used for cosmetic treatment of hyper-functional facial lines [11]. More recently, botox has emerged as an effective, minimally invasive tool to combat gummy smile for patients with hyper-functional upper lip [4].
This paper presents a case of severe vertical maxillary excess which was jointly treated with Lefort I osteotomy, V–Y plasty for lip lengthening and Botox in an effort to recreate smile.
Case
A 26-year-old male presented to the Department of Orthodontics and Dentofacial Orthopaedics with increased gingival exposure during smile and proclined teeth. The patient had a convex profile with incompetent lips; short & hypertonic upper lip and increased lower anterior facial height. On smiling, the patient had a gingival exposure of over 9 mm (Fig. 1) with multiple teeth missing in the posterior segment. It was diagnosed as a mutilated case having a class II canine relation with an overjet of 10 mm. Cephalometric analysis revealed a skeletal Class II pattern with a prognathic maxilla with anterior vertical excess of 10 mm and a posterior excess of 4 mm. The patient had increased lower facial height of 12 mm and a retrognathic chin (Fig. 2).
Fig. 1.
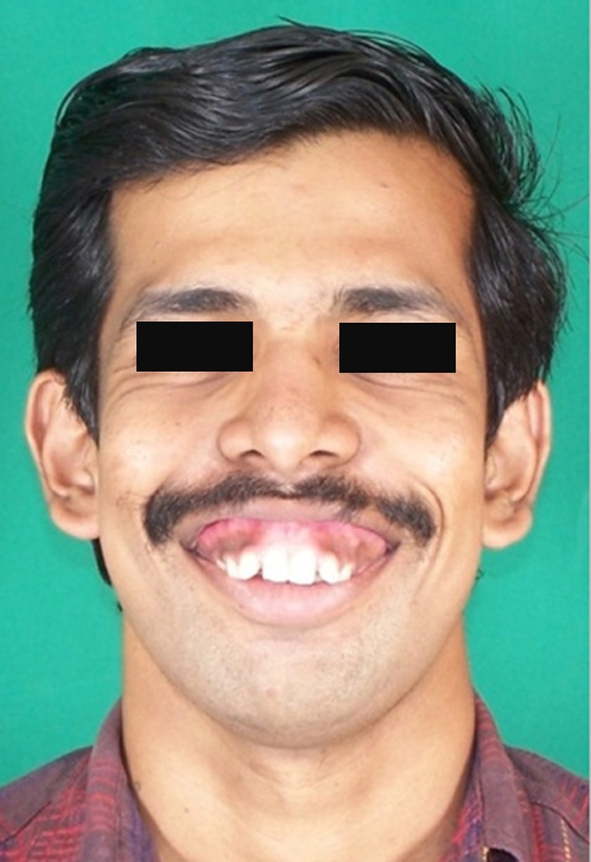
Pre-surgical gingival exposure
Fig. 2.

Pre-surgical Cephalogram
After successful completion of pre-surgical orthodontics which basically consisted of decompensation of upper and lower arches with 0.022″ MBT appliance, the patient was referred to the Department of Oral & Maxillofacial Surgery. A conventional Lefort I osteotomy with a superior impaction of 6 mm in the anterior and 4 mm in the posterior region along with a segmental osteotomy in the anterior maxilla was done to combat the prognathic maxilla. A V–Y plasty was performed on table in order to lengthen the lip. A genioplasty to advance the chin was also done simultaneously. Post surgery, although there was significant improvement in the patient profile and smile, there was still about 5 mm gingival exposure during smile (Figs. 3, 4). The dissatisfaction expressed by the patient led us to consider another treatment option, Botox. The pros and cons of injecting Botox were discussed with the patient who was very receptive to the idea which targeted his chief complaint of gummy smile.
Fig. 3.
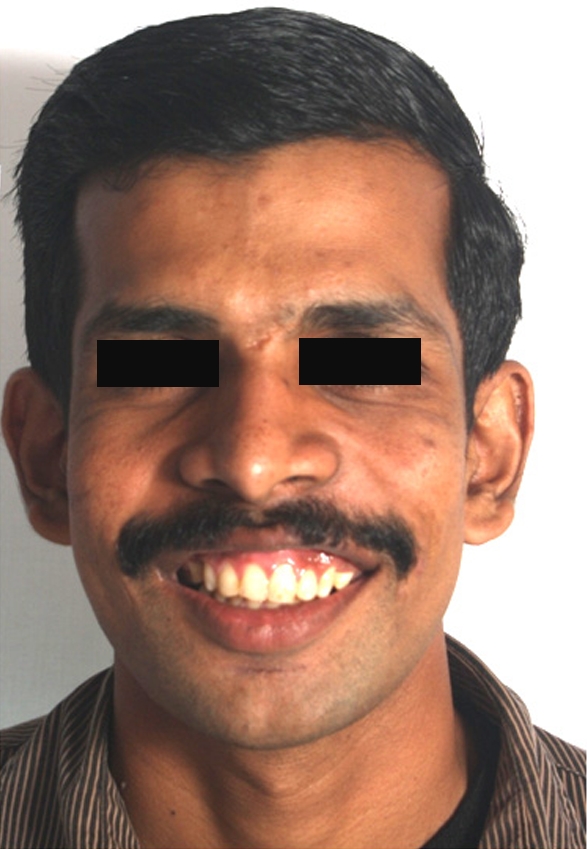
Post-surgical gingival exposure
Fig. 4.

Post-surgical Cephalogram
Botox and Injection Technique
BOTOX (BTX-A: purified botulinum Toxin Type A), is a sterile, vacuum dried neurotoxin complex produced from fermentation of hall strain clostridium botulinum toxin type A, grown in a medium containing casein hydrolysate, glucose and yeast extract.
BTX-A was diluted according to the manufacturer’s recommendations to yield 2.5 units per 0.1 ml by adding 4.0 ml 0.9% Normal Saline to 100 units of vacuum dried BTX-A. Under sterile conditions, 2.5 units were injected at two sites per side (Table 1).
Table 1.
Site of Injection
| S. No. | Site of injection |
|---|---|
| 1 | Overlapping area of levator labii superioris alaeque nasi and levator labii superioris muscles. |
| 2 | Overlapping area of levator labii superioris and zygomaticus minor muscles. |
The patient had a gummy smile associated with prominent nasolabial fold. Therefore, the injection was given at the labial component of the levator labii superioris alaeque nasii, at the bulge of the uppermost part of the nasolabial fold [12]. The injection sites were determined by muscle animation (smiling) and palpation on contraction to ensure precise muscle location before injection [13] (Figs. 5, 6).
Fig. 5.
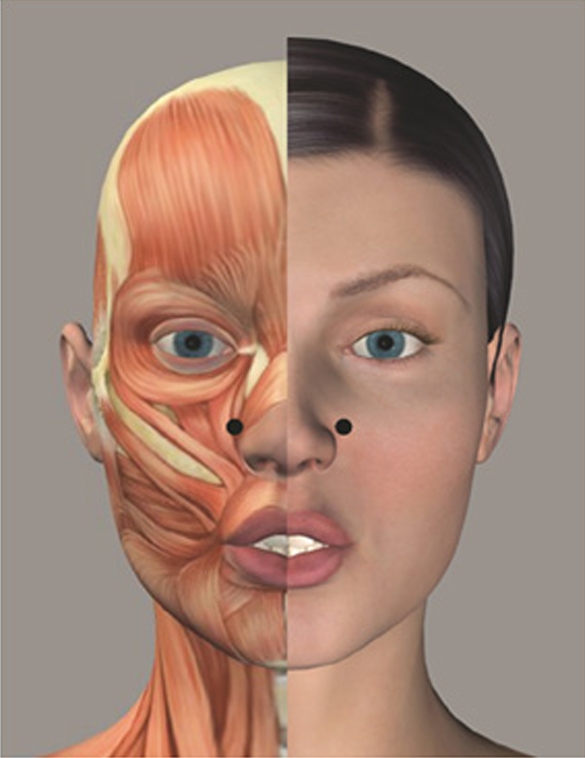
Overlapping area of levator labii superioris alaeque nasi and levator labii superioris muscles
Fig. 6.

Overlapping area of levator labii superioris and zygomaticus minor muscles
Reference points used for the measurements were [13]:
A—Lowest margin of upper lip perpendicular and superior to the mid portion of maxillary central incisor gingival margin
B—The maxillary central incisors gingival margin at its midpoint
C—The midpoint of the incisal edge of the maxillary central incisor (Fig7)
Fig. 7.
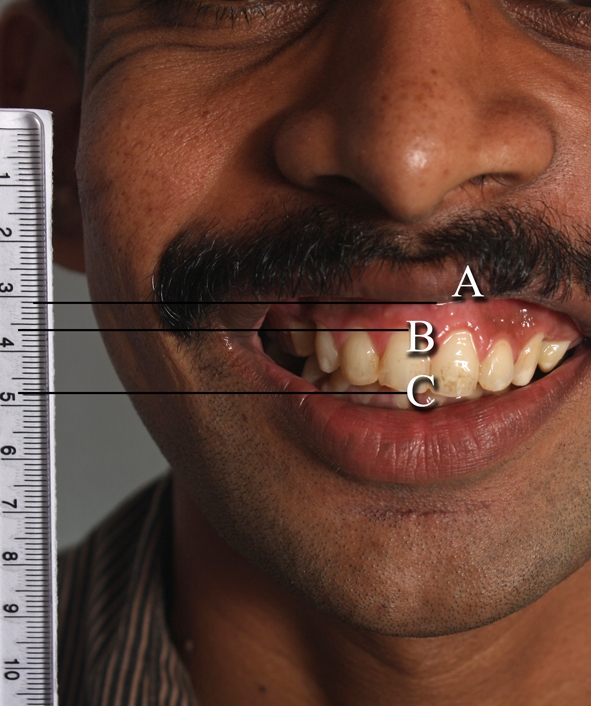
Reference points used for measurements
A–B—5 mm & A–C—17 mm
Patient was recalled at 2, 4 weeks and then, once every month for 4 months to record the changes.
Results
The results were markedly noticeable at 2 weeks. At A–B i.e. from the lowest margin of the upper lip to the gingival margin, there was no exposure of gingiva. At A–C, there was a 5 mm reduction in exposure from the lowest margin of the upper lip to the incisal edge (Fig. 8). The results were consistent for 2 months. However, relapse was noted by the 3rd month (Table 2).
Fig. 8.

Post botox
Table 2.
Measurements of gingival exposures pre and post botox
| Sl. No | Measurements | Pre treatment | 2 weeks | 4 weeks | 2 months | 3 months | 4 months |
|---|---|---|---|---|---|---|---|
| 1 | A–B | 5 mm | 0 mm | 0 mm | 0 mm | 2 mm | 3 mm |
| 2 | A–C | 17 mm | 12 mm | 12 mm | 12 mm | 14 mm | 15 mm |
Discussion
Esthetic improvement is paramount to functional aspects in orthognathic cases as the patient is more concerned with the former. Many adjunctive soft tissue procedures can be used to preclude this problem [14]. Lefort I osteotomy with superior impaction is most commonly adopted to treat skeletal vertical maxillary excess coupled with gingivectomies [4].However, conventional Lefort I has a limitation of congesting the nasal airway function if performed in very severe cases of vertical maxillary excess. A modification of Lefort I, a Horse-shoe osteotomy is indicated when major superior repositioning of 5–15 mm is required which leaves the nasal floor intact [6, 15]. This is however, not commonly practised. Also, the principle is to under-correct in the vertical dimension, for, the incisal edges hidden beneath the upper lip causes the patient to appear prematurely aged and edentulous [16]. The V–Y lengthening done for a short upper lip, however, increases the length only by 2–3 mm which is marginal [14]. In the case under discussion, however, even correcting the vertical dimension to the desired extent would still leave a gummy smile due to the hypertonic lip.
The use of Botox for various cosmetic procedures have been described extensively in literature [7–10, 17]. Botox blocks the neuromuscular transmission by binding to acceptor sites on motor or sympathetic nerve terminals, thereby, inhibiting the release of acetylcholine. This inhibition occurs as Botox cleaves the synaptosomal–associated protein (SNAP-25). Therefore, when injected intramuscularly at therapeutic doses, it produces partial chemical denervation of the muscle resulting in localised reduction in muscle activity [18]. Levator labii superioris, zygomatic major and superior fibres of buccinators muscles under the nasolabial fold are responsible for the production of full smile. The gummy smile is dominated by the excessive contractions of the levator labii superioris muscles. By injecting at the predetermined sites, Botox brings about reduction in gingival exposure by weakening the contractibility of the upper lip elevator muscles and also, a marked effacement of the nasolabial fold [13]. Partial to complete upper lip drooping, due to hypotony or atony of the central elevators may lead to excessive upper lateral pulling of the zygomaticus major and as a consequence, a ‘joker smile’ may result [19]. Although, the results began to reverse by the 4th month, the exposure, however, never returned to the original values [13]. Since the dose injected was minimal, there was no perceivable hypokinesis at 8 months follow-up (Fig. 9).
Fig. 9.

At 8 months follow-up
Conclusion
As opposed to various other surgical procedures, Botox has proven to be a minimally invasive, effective alternate for the correction of gummy smile caused by upper lip elevator muscles. It, therefore, can be a useful adjunct to enhance the aesthetics and improve patient satisfaction where orthognathic surgery alone may prove inadequate.
References
- 1.Flannary C. The psychology of appearance and psychological impact of surgical alteration of the face. In: Bell WH, editor. Orthognathic and reconstructive surgery. 1. Philadelphia: W B Saunders; 1992. pp. 2–21. [Google Scholar]
- 2.Nurminen L, Pietila T, Vinkka Puhakka H. Motivation for and satisfaction with orthodontic surgical treatment: a retrospective study of 28 patients. Eur J Ortho. 1999;21(1):78–87. doi: 10.1093/ejo/21.1.79. [DOI] [PubMed] [Google Scholar]
- 3.Hwang Woo-Sang, Hun Mi-Su, Kyung-Seol Hu, Song Wu-Chul. Surface anatomy of lip elevator muscles for the treatment of gummy smile using botulinum toxin. Angle Orthod. 2009;99(1):70–76. doi: 10.2319/091407-437.1. [DOI] [PubMed] [Google Scholar]
- 4.Polo M. Botulinum toxin type A for neuromuscular correction of excessive gingival display on smiling. Aust J Orthod Dentofac Orthop. 2005;127(2):214–218. doi: 10.1016/j.ajodo.2004.09.013. [DOI] [PubMed] [Google Scholar]
- 5.Sandler PJ, Alsayer F, Davies SJ. Botox: a possible new treatment for gummy smile. Virtual J Orthod. 2007;20:30–34. [Google Scholar]
- 6.Malik NA. Text book of oral and maxillofacial surgery. 3. New Delhi: Jaypee; 2008. pp. 307–308. [Google Scholar]
- 7.Brin MF, Hallett M, Jankovis J. Preface. In: Brin MF, Hallett M, Jankovis J, editors. Scientific and therapeutic aspects of botulinum toxin. Philadelphia: Lippincott William and Wilkins; 2002. pp. 5–6. [Google Scholar]
- 8.Scott AB. The role of botulinum toxin type A in the management of strabismus. In: Brin MF, Hallett M, Jankovis J, editors. Scientific and therapeutic aspects of botulinum toxin. Philadelphia: Lippincott William and Wilkins; 2002. pp. 189–195. [Google Scholar]
- 9.Comella CL. Cervical dystonia: treatment with botulinum toxin serotype A as Botox or Dysport. In: Brin MF, Hallett M, Jankovis J, editors. Scientific and therapeutic aspects of botulinum toxin. Philadelphia: Lippincott William and Wilkins; 2002. pp. 359–364. [Google Scholar]
- 10.Mauriello JA. The roles of botulinum toxin type A (Botox) in the management of blepherospasm and hemifacial spasm. In: Brin MF, Hallett M, Jankovis J, editors. Scientific and therapeutic aspects of botulinum toxin. Philadelphia: Lippincott William and Wilkins; 2002. pp. 197–206. [Google Scholar]
- 11.Sposito MM. New indications for botulinum toxin type A in treating facial wrinkles of the mouth and neck. Aesthetic Plast Surg. 2002;26:89–98. doi: 10.1007/s00266-002-1491-2. [DOI] [PubMed] [Google Scholar]
- 12.De Maio M. Gummy smile. Botulinum toxin in aesthetic medicine. New York: Springer; 2007. pp. 78–79. [Google Scholar]
- 13.Polo Mario. Botulinum toxin types A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile) Am J Orthod Dentofacial Orthop. 2008;133(2):195–203. doi: 10.1016/j.ajodo.2007.04.033. [DOI] [PubMed] [Google Scholar]
- 14.Sarver DM, Rousso D. Plastic surgery combined with orthodontic and orthognathic procedures. Am J Orthod and Dentofacial Orthop. 2004;126(3):305–307. doi: 10.1016/j.ajodo.2004.06.004. [DOI] [PubMed] [Google Scholar]
- 15.Wardbooth P. Maxillofacial surgery. Edinburgh: Churchill Livingstone; 2006. p. 1239. [Google Scholar]
- 16.Mathes SJ. Plastic surgery. In: Mathes SJ, Hentz VR, editors. Head and neck Part I. 2. Philadelphia: Saunders; 2007. p. 675. [Google Scholar]
- 17.Kane MA. The effect of Botulinum toxin injections on the nasolabial fold. Plast Reconstr Surg. 2003;112(suppl):67–725. doi: 10.1097/01.PRS.0000082195.44980.10. [DOI] [PubMed] [Google Scholar]
- 18.Binder WJ, Blitzer A, Brin MF. Treatment of hyper-functional lines of face with botulinum toxin A. Dermatol Surg. 1998;24:1198–1205. doi: 10.1016/S1076-0512(98)00181-2. [DOI] [PubMed] [Google Scholar]
- 19.De Maio M, Rzany B (2007) Chapter 5: the most common indications, 5.7-6 complications. Botulinum toxin in aesthetic medicine, Springer, Berlin, p 69