

ABSTRACT
Massive vaginal bleeding represents one of the emergencies that the gynecologists have to deal with. When unresponsive to the haemostatic treatment (local or iv), the bleeding can be stopped by using the uterine artery embolization. It provides visualization of the bleeding site and enables targeted, minimally invasive therapy to achieve hemostasis. We present a case of a patient with cervical cancer associated with massive vaginal bleeding and the beneficial effects of the uterine artery embolization in the therapy management.
Keywords: cervical cancer, pelvic hemorrhage, embolization
INTRODUCTION
There are many interventional tehniques that can be used to aid the gynecologists/oncologists in caring for their patients in the acute setting. Bleeding related to cervical cancer is amenable to embolization.
Uterine artery embolization is a tehnique used by interventional radiologists that has been available for 20 years in the treatment of various gynecologic and obstetric conditions with massive, uncontrolable hemorrhage. The eficiency of selective embolization of one or both uterine arteries, is clinicaly proven by the hemorrhage's cease (1).
We present the case of a patient with cervical cancer and hemorrhage treated with the uterine artery embolization. ❑
CASE REPORT
A 35 year old patient was admitted in our hospital for a cervical tumor associated with massive vaginal bleeding and pelvic pain. Two month prior to the hospital admission the patient started having abnormal vaginal bleeding. The patient had no significant personal or family history of cervical cancer. Investigations performed two weeks earlier in another clinical setting (clinical examination and cervical biopsies) had led to the diagnosis of cervical squamos cancer.
The current clinical examination showed massive cervical bleeding without blood clotting.
The blood pressure was 90/50 mmHg and the heart rate was 100 beats per minute.
Laboratory tests showed a severe secondary anemia (hemoglobin 7 mg/dl).
Transvaginal ultrasound and the MRI suggested the presence of a 32x45x27 mm intramural mass on the posterior wall of the cervix with infiltrative prolongations in the lateral and anterior walls of the cervix without secondary determinations in the abdominal organs and with 2 images of external iliac lymph nodes present (13 mm on the right side and 14 mm on the left side). The current clinical examination and the paraclinic investigations led us to the suspicion of IIB stage cervical cancer.
A cervix biopsy was performed under local anesthesia and a hemostatic treatment (local and iv adrenostasine, fitomenadione, ethampsilat) was started.
The blood transfusion (2 units) was initiated in order to correct the anemia.
After two days of hemostatic treatment, the vaginal bleeding was still present, so the embolization of the uterine artery was performed until stasis of blood flow was demonstrated. The uterine artery embolization is an interventional radiology technique, minimum invasive, with a short post embolization recovery time (Figure 1). In this case the radiologist decided to use an unilateral brachial approach, which has as advantages the fact that the patient can be mobilized immediately after the intervention and only one punction is needed. After a local anesthezia with xiline, the embolospheres associated with a contrast substance were injected, over selectively catheterizing every vessel that fed the tumor.
Figure 1. Pelvic arteriography: before and after embolization.
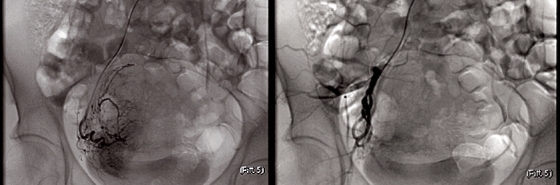
The vaginal bleeding stopped within 24 hours after the intervention.
The conservative treatment described proved efficient in relieving the patient's symptoms and was assisted by the good collateral blood supply which characterizes the pelvic region. The patient accused pelvic pain, treated with anti-inflamatory and antibiotic drugs.
External radiotherapy was afterwords performed using 26,2 GY, associated with curietherapy.
Six weeks after the radiotherapy, we were able to proceed to the surgical treatment, represented by a complete lymphadenocolpohysterectomy (Wertheim technique). The hystopathological result highlighted the presence of a squamos cervical cancer. ❑
DISCUSSION
Cervical hemorrhage can be a difficult problem during cervical cancer management. The cervical bleeding can increase the morbidity either by a secondary anemia and its complications either by haemorrhagic shock.
A standard pocedure was the ligation of the hypogastric artery, which has proved its efficiency in controlling massive bleeding in cervical carcinoma, postoperative bleeding, trauma and obstetric bleeding refractory to local therapy. The reported succes rates of hypogastric artery ligation have been widely variable, ranging from 40% to 100% in contemporary series (2-5). The procedure's limits are represented by the highly deformed pelvic anatomy (due to radiotherapy or to the recurrence of cancerous tissue) and the critically ill patients. In these cases, the morbidity can be increased by the difficult situations that can appear during the operation and the anesthetic complications (6).
The first reported use of transcatheter arterial embolization in obstetrics and gynecology was the control of intractable pelvic hemorrhage in patients with gynecologic malignancies in the mid 1970s (7,8). This procedure was accepted in a short period of time because of its low mortality and morbidity rates. The embolization of anterior branch of the internal iliac artery may easily prevent the bleeding in the pelvic region, but presents several undesirable complications such as: bladder ischemia, vesicovaginal fistula, necrosis of the gluteus and neurological deficiencies in lower extremities. This complications may only be reduced via superselective embolization of uterine artery.
Several studies have been performed in order to underline the beneficial role of this procedure. Pisco et al (9) performed transcatheter embolization of the internal iliac arteries in 108 patients with uncontrolable bleeding in pelvic neoplasm (uterus in 39, ovary in 16, urinary bladder in 50 and prostate in 3). This study results show complete control of the hemorrhage in 69 % of the patients and partial control in 21% of the patients. They were unable to reduce the need for transfusion in 11 patiens, 6 of whom had only unilateral embolization due to anatomic reasons. Yamashita et al (5) reported 100% temporary control of bleeding in 17 patients with malignant neoplasm. Mihmanli et al (10) showed successful cessation of vaginal hemorrhage by arterial embolization in 6 patient with gynecologic malignancies. Serdac and others (11) reported 100% temporary control of bleeding in 8 patients with terminal stage cervical cancer, 2 of whom had developed vesicovaginal fistula (it was not clear whether it was due to the embolization or recurring invasion of the cervical cancer).
Based on this limited reports, it appears that arterial embolization plays a significant role in urgent control of massive bleeding in gynecologic malignancies.
Transcatheter arterial embolization is a safe and effective treatment for massive bleeding in cervical cancer (12,13). Immediate postembolization clinical examinations demonstrated that the bleeding effectively stopped in all cases. After this procedure, the need for blood transfusion was eliminated in all of the cases while the potential complications related to blood transfusion are prevented.
Artherial embolization advantages:
the ability to achieve rapid control of hemorrhage,
lower incidence of rebleeding (this technique produces more distal occlusions than the surgical ligation),
improvement in general condition of the patients,
the decreased in tumor size gradually appears due to declined feeding of the tumor.
reduced intraoperatory bleeding during the consecutive surgical intervention and implies minumum risks and unwanted effects.
The most common side effects observed are severe pain related to the ischemia of tumor tissue. These side-effects are temporary and can be stopped by administrating simple analgesics to the patient. ❑
CONCLUSIONS
Genital bleeding is a major cause of morbidity and mortality in many gynecological disorders and its management represents a challenge for gynecologists. The purpose of arterial embolization is to raise the quality of life and betterment of those patients by minimizing surgical morbidity through the use of less invasive method of arterial embolization.
References
- 1.Carol C Wu, Lee MH. Transcatheter Arterial Embolotherapy: A Therapeutic Alternative in Obstetrics and Gynecologic Emergencies. Seminars in Interventional Radiology. 2006;23:240–248. doi: 10.1055/s-2006-948761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chattopadhyay SK, Deb Roy B, Edrees YB. Surgical control of obstetrics hemorrhage: hypogastric artery ligation or hysterectomy ? Int J Gynecolog Obstet. 1990;32:345–351. doi: 10.1016/0020-7292(90)90112-x. [DOI] [PubMed] [Google Scholar]
- 3.Evans S, McShane P. The efficacy of internal iliac artery ligation in obstetrics hemorrhage. Surg Gyncol Obstet. 1985;160:250–253. [PubMed] [Google Scholar]
- 4.Thavarasah AS, Sivalingam N, Almohdzar SA. Internal iliac and ovarian artery ligation in control of pelvic hemorrhage. Aust N Z J Obstet Gyneecol. 1989;29:22–25. doi: 10.1111/j.1479-828x.1989.tb02870.x. [DOI] [PubMed] [Google Scholar]
- 5.Yamashita Y, Harada M, Yamamoto H, et al. Transcatheter arterial embolization of obstetrics and gynecological bleeding: efficacy and clinical outcome. Br J Radiol. 1994;67:530–534. doi: 10.1259/0007-1285-67-798-530. [DOI] [PubMed] [Google Scholar]
- 6.Higgins CB, Bookstein JJ, Davis GB, et al. Therapeutic embolization for chronic bleeding. Radiology. 1977;122:473–478. doi: 10.1148/122.2.473. [DOI] [PubMed] [Google Scholar]
- 7.Miller FJ Jr, Mortel R, Mann WJ, et al. Selective arterial embolization for control of hemorrhage in pelvic malignancy: femoral and brachial catheter approaches. AJR Am J Roentgenol. 1976;126:1028–1032. doi: 10.2214/ajr.126.5.1028. [DOI] [PubMed] [Google Scholar]
- 8.Schwartz PE, Goldstein HM, Wallace S, et al. Control of arterial hemorrhage using percutaneous arterial catheter techniques in patients with gynecologic malignancies. Gynecol Oncol. 1975;3:275–288. doi: 10.1016/0090-8258(75)90035-9. [DOI] [PubMed] [Google Scholar]
- 9.Pisco JM, Martins JM, Correia MG. Internal iliac artery: embolization to control hemorrhage from pelvic neoplasm. Radiology. 1989;172:337–339. doi: 10.1148/radiology.172.2.2748811. [DOI] [PubMed] [Google Scholar]
- 10.Mihmanli I, Cantasdemir M, Kantarci F, et al. Percutaneous embolization in the management of intractable vaginal bleeding. Arch Gynecol Obstet. 2001;264:211–214. doi: 10.1007/s004040000119. [DOI] [PubMed] [Google Scholar]
- 11.Serdar Y, Fulya K, Nurettin B, et al. Embolization of uterine artery in terminal stage cervical cancer. Cancer Investigation. 2002;20:754–758. doi: 10.1081/cnv-120003543. [DOI] [PubMed] [Google Scholar]
- 12.Shawky ZA, Badaw, Amr E, et al. Uterine artery embolization: The role in obstetrics and gynecology. Journal of Clinical Imaging. 2001;25:288–295. doi: 10.1016/s0899-7071(01)00307-2. [DOI] [PubMed] [Google Scholar]
- 13.Shellie C Josephs, MD. Obstetric and Gynecologic Emergencies: A Review of Indications and Interventional Techniques. Seminars in Interventional Radiology. 2008;25:337–346. doi: 10.1055/s-0028-1102992. [DOI] [PMC free article] [PubMed] [Google Scholar]