

Abstract
AIM: To study the response to infliximab in pediatric inflammatory bowel disease (IBD), as reflected in fecal calprotectin levels.
METHODS: Thirty-six pediatric patients with IBD [23 Crohn’s disease (CD), 13 ulcerative colitis (UC); median age 14 years] were treated with infliximab. Fecal calprotectin was measured at baseline, and 2 and 6 wk after therapy, and compared to blood inflammatory markers. Maintenance medication was unaltered until the third infusion but glucocorticoids were tapered off if the patient was doing well.
RESULTS: At introduction of infliximab, median fecal calprotectin level was 1150 μg/g (range 54-6032 μg/g). By week 2, the fecal calprotectin level had declined to a median 261 μg/g (P < 0.001). In 37% of the patients, fecal calprotectin was normal (< 100 μg/g) at 2 wk. By week 6, there was no additional improvement in the fecal calprotectin level (median 345 μg/g). In 22% of the patients, fecal calprotectin levels increased by week 6 to pretreatment levels or above, suggesting no response (or a loss of early response). Thus, in CD, the proportion of non-responsive patients by week 6 seemed lower, because only 9% showed no improvement in their fecal calprotectin level when compared to the respective figure of 46% of the UC patients (P < 0.05).
CONCLUSION: When treated with infliximab, fecal calprotectin levels reflecting intestinal inflammation normalized rapidly in one third of pediatric patients suggesting complete mucosal healing.
Keywords: Crohn’s disease, Ulcerative colitis, Surrogate markers, Pediatrics, Monoclonal antibodies, Infliximab
INTRODUCTION
The recent development of easily applicable fecal surrogate markers for intestinal inflammation has provided new means for objective assessment of disease activity and treatment response in chronic inflammatory bowel disease (IBD), a disease becoming more prevalent among children[1]. This is especially important in pediatric patients with limited possibility for follow-up endoscopy due to invasiveness. The fecal levels of neutrophil-derived markers, such as fecal calprotectin or lactoferrin, reflect the mucosal influx of inflammatory cells in the intestine, thus associating with the presence of active inflammation. In IBD, fecal calprotectin levels relate to the findings in endoscopy but also with the grade of histological inflammation[1-4]. When compared to clinical scores and serum inflammatory markers, fecal calprotectin is the most accurate tool to detect the presence of active mucosal inflammation in the colon[4-6]. The negative predictive value for the presence of active inflammation is high (87%)[4]. In children, it has been shown that the level of fecal calprotectin[2,3,7,8] or lactoferrin[6,9] may guide the need for endoscopy.
The data on fecal markers during therapy of IBD are sparse. We showed recently that during glucocorticoid therapy in pediatric patients, fecal calprotectin levels rarely declined below the limit of a raised value, suggesting ongoing mucosal inflammation. However, in those clinically responding to therapy, fecal calprotectin values fell markedly during the first month of therapy[10]. In children presenting with clinically quiescent IBD, only one third of the patients have fecal calprotectin levels below the upper normal limit, whereas the others have raised values, although not reporting subjective symptoms[11]. In adults, fecal calprotectin values are associated with mucosal healing in Crohn’s disease (CD) patients who respond to therapy with tumor necrosis factor (TNF)-α antagonists or other IBD medication[12,13]. In a pilot study by Buderus et al[14], the levels of fecal lactoferrin were measured in five children on infliximab therapy, who showed a decline after the first infusion in each case. The pattern of fecal calprotectin levels during introduction of TNF-α antagonist therapy in children has not yet been described.
In pediatric patients, TNF-α antagonists have emerged for therapy of severe IBD that does not respond to conventional treatment[15-17]. Fecal calprotectin provides a non-invasive means to assess the presence of intestinal inflammation, therefore, we conducted a prospective study in pediatric patients treated with TNF-α antagonist infliximab. Our aim was to study the pattern of fecal calprotectin concentrations during the early phase of therapy.
MATERIALS AND METHODS
Study population
We prospectively studied 36 children (median age 14 years, range 5.6-17.6 years; 20 boys 20, 16 girls) diagnosed with IBD according to the Lennard-Jones criteria[18], and consecutively introduced to therapy with infliximab. In two cases, the diagnosis of CD was based on extensive aphthous ulceration visualized by wireless capsule endoscopy. All patients had moderate to severe disease that did not respond to treatment with 5-aminosalicylic acid (5-ASA), immunosuppressants or glucocorticoids. In four cases, infliximab was introduced shortly after a diagnosis of extensive small bowel disease. In three patients, the indication for anti-TNF-α agent was fistulating disease, and in all the others, poor response to maintenance medication or steroid dependency. The study group comprised 23 pediatric patients with CD, and 13 with ulcerative colitis (UC). The background data, disease distribution, and medication of the patients are shown in Table 1. Fourteen patients underwent ileocolonoscopy, seven underwent wireless capsule endoscopy, and seven magnetic resonance imaging enterography within 1 m prior to the introduction of infliximab therapy, confirming active disease.
Table 1.
Background data of 36 pediatric patients with inflammatory bowel disease treated with infliximab
| Variable | Result |
| Age median (range) | 14 (5.6-17) yr |
| Sex | 20 boys, 16 girls |
| Diagnosis | |
| CD | 23 |
| Ileitis | 8 |
| Ileocolitis | 8 |
| Colitis | 7 |
| UC | 13 |
| Left-sided colitis | 4 |
| Pancolitis | 9 |
| Maintenance medication at baseline | |
| 5-ASA | 10 |
| 5-ASA + azathioprine/6-MP | 12 |
| Azathioprine/6-MP | 7 |
| None | 7 |
| Prednisolone/budesonide at baseline | 19 |
| Disease duration (median, range) | 2.1 (0.4-7.6) yr |
CD: Crohn’s disease; UC: Ulcerative colitis; 5-ASA: 5-aminosalicylic acid; 6-MP: 6-mercaptopurine.
TNF-α antagonist infliximab (Remicade®) was sche-duled at 5 mg/kg at week 0, 2 and 6. All infusions were administered at the Hospital for Children and Adolescents, Helsinki University, Finland during February 2008 to December 2010. The maintenance medication was unaltered until week 6, but if the patient improved clinically, glucocorticoids were tapered off. At each visit, the patients provided a stool sample for fecal calprotectin measurement and a blood sample for measurement of inflammatory marker erythrocyte sedimentation rate (ESR), and hemoglobin. Fecal calprotectin was measured in the routine clinical laboratory by a quantitative enzyme immunoassay (PhiCal Test, Calpro AS, Oslo, Norway; NovaTec Immunodiagnostica, Dietzenbach, GmBH, Germany) and the values quoted as normal were < 100 μg/g stool[10,19]. The clinical activity of the disease was assessed by physicians global assessment (PGA) score from 1 to 3[20].
Ethical considerations
The ethics committee of Helsinki University Central Hospital approved the study protocol. The families attending the study signed an informed consent form.
Statistical analysis
Spearman non-parametric correlation test, Kruskal-Wallis test, Mann-Whitney U test, and Fisher’s exact test were used. The level of statistical significance was P < 0.05. The values are presented as median and range.
RESULTS
Fecal calprotectin was high at the introduction of infliximab therapy, with a median value of 1150 μg/g (range: 54-6032 μg/g). Two patients had fecal calprotectin < 100 μg/g (reference limit for a raised value), and their indication for treatment was steroid-dependent colitis. By week 2, the median level of fecal calprotectin level had declined to 261 μg/g (Figure 1; P < 0.001, Mann-Whitney U test). In 11 of 30 (37%) patients, fecal calprotectin was below the reference limit (100 μg/g) by week 2. By week 6, there was no additional improvement in the median fecal calprotectin level (345 μg/g, range: 5-5253 μg/g, Figure 1). The individual variation of fecal calprotectin levels is shown in Figure 2.
Figure 1.
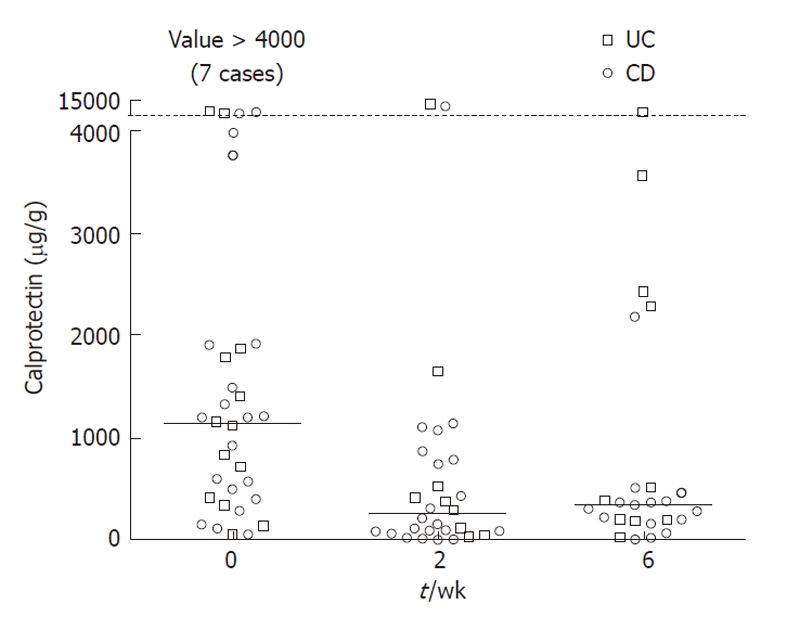
Fecal calprotectin levels at baseline, and 2 and 6 wk after introduction of infliximab therapy in children with Crohn’s disease or ulcerative colitis. The decline in levels between baseline and week 2 was statistically significant (P < 0.001). CD: Crohn’s disease; UC: Ulcerative colitis.
Figure 2.
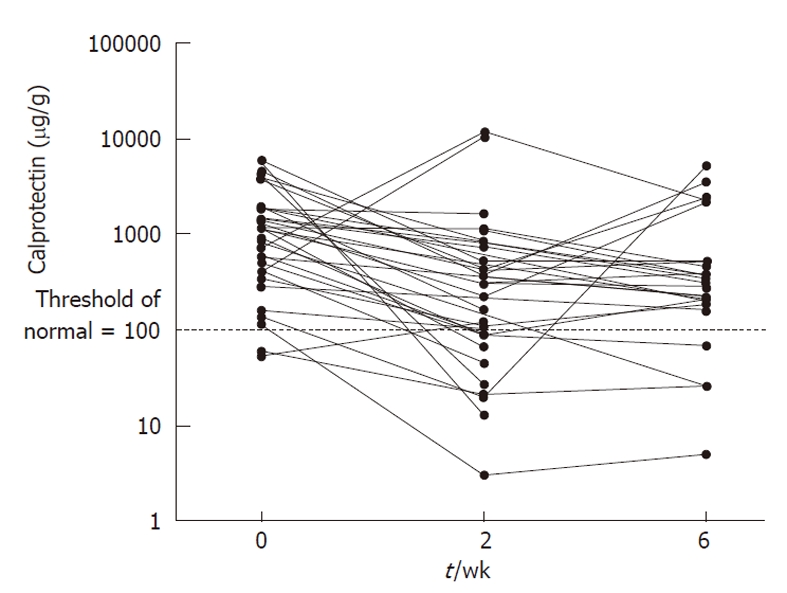
Fecal calprotectin levels at baseline, and 2 and 6 wk after introduction of infliximab therapy showing the individual variation in children with inflammatory bowel disease.
Disease extension or diagnosis did not relate to fecal calprotectin levels or to treatment response (data not shown). Fecal calprotectin decreased in 21 of 22 (95%) of the CD patients, with a raised value during the introduction phase, but in one case, the response was temporary. By week 6, there was no response in two cases when compared to baseline. One patient with CD presented with low fecal calprotectin levels throughout the study period. In this particular case, the indication for treatment was steroid dependency and steroids were tapered off during induction. Thus, the effect of infliximab therapy on fecal calprotectin could not be assessed, and she was not included in the analysis. Of the UC patients with increased fecal calprotectin at baseline, the level decreased in 10 of 12 (83%) patients, but increased to pretreatment levels or above by week 6 in three of 10 (30%) children. Of the two children with no initial decline in fecal calprotectin level, there was no clinical response and the level stayed constantly high (> 1600 μg/g) or increased more than 10-fold within 6 wk. The child with steroid-dependent UC and low fecal calprotectin at the start of this therapy (high disease activity confirmed in colonoscopy 1.5 mo earlier) showed mild elevation in the level (up to 120 μg/g). Thus, by week 6, fecal calprotectin level suggested a response in 20 of 22 (91%) of the CD patients and in seven of 13 (54%) of the UC patients (P < 0.05, Fisher’s exact two-tailed test), corresponding to a figure of 22% of non-responsive patients in total.
Blood inflammatory marker ESR decreased from a median value of 20 mm/h (range: 2-46 mm/h) at baseline to 9 mm/h (range: 2-34 mm/h, P < 0.05, Mann-Whitney U test) at 2 wk. At baseline, 19 of 31 patients (61%) had elevated ESR. By week 2, the respective figure was 28% (9/32). Median PGA score was 2 at baseline (range: 1-3), and by week 2 and 6, the score was 1 (range: 1-3, P < 0.001); by week 6, the majority of patients (33/36) presented with a score of 1. For hemoglobin levels, there was no significant increase in the median values [118 g/L (range: 95-152 g/L) at baseline and 124 g/L at 2 wk (range: 80-147 g/L)]. Glucocorticoids were tapered off in 10/19 patients during the induction phase.
DISCUSSION
Therapy with TNF-α antagonists has emerged in pediatric patients suffering from moderate to severe CD[21,22], but recently, a therapeutic response has also been reported in severe UC[16,23]. These therapies are effective but at present have high costs and carry a risk for the development of severe adverse effects, which possibly hampers their clinical use[24,25]. Thus, it is of key importance to target the therapy on those who show a positive response and to discontinue administration of TNF-α antagonists if the patient is a non-responder[25]. In keeping with this, surrogate markers for the presence of intestinal inflammation such as fecal calprotectin[13,26] are promising and non-invasive means for the assessment of disease activity in IBD. There have only been a few studies on fecal calprotectin related to therapeutic response in IBD. Previously, we have assessed the pattern of fecal calprotectin in acute pediatric IBD from the start of glucocorticoid therapy until their discontinuation[10], and in adults during the first 12 wk of TNF-α antagonist therapy[12]. Here, we showed the pattern of fecal calprotectin in pediatric IBD during the induction phase of TNF-α antagonist therapy, demonstrating a rapid decline in fecal calprotectin levels within the first weeks of induction in the majority of pediatric IBD patients, suggesting an early response.
By week 2 after introduction of infliximab, the median level of fecal calprotectin had declined by 77% from baseline. Expectedly, this rapid decrease in fecal calprotectin in children paralleled the pattern seen in adults after introduction of TNF-α antagonist treatment. In a previous study in adults, endoscopy confirmed remission in 30% of CD patients when assessed at 3 mo[12]. In the present study, in one third of the children, the fecal calprotectin levels had declined to normal - suggesting remission - by week 2 after the start of infliximab therapy. Unexpectedly, there were only a few cases that showed normalization of fecal calprotectin by week 6, thus, the 2-wk result equaled the proportion of children with suggested mucosal healing - the target of IBD therapy[27] - and remission during the induction phase. The finding of an excellent therapeutic response in one third of the patients is comparable to our previous findings in children with acute IBD treated with glucocorticoids (showing a normalization of fecal calprotectin in 27% of patients[10]), and in adults treated with TNF-α antagonist therapy[12] (see above). In two thirds of the patients, fecal calprotectin did not normalize, suggesting incomplete mucosal healing during the induction phase of infliximab therapy. It is important to note that the fecal calprotectin level that is considered as a satisfactory therapeutic response remains undecided. Furthermore, the long-term treatment outcome in pediatric patients related to fecal calprotectin levels warrants further studies. In adult patients, mucosal healing predicts a better long-term outcome[28].
Although primary response to TNF-α antagonist therapy is excellent in children, covering 80%-90% of patients with CD, the therapeutic response according to clinical disease activity may deteriorate during the first year of therapy in a considerable proportion of children. It has been estimated that 34%-49% of initial responders need dose escalation or more intense therapy during the first year of infliximab therapy[15,22]. For infliximab therapy in adults, rates of dose intensification ranging from 31% to 36% at 12 mo are comparable to those in pediatric patients[29,30]. Here, the primary response was possibly lost already during the introduction phase in > 10% of the patients, as reflected in the fecal calprotectin levels. In these particular children, PGA did not decrease either. However, clinical activity indices have less correlation to the presence of mucosal inflammation than fecal neutrophil biomarkers, as shown in adult CD patients[31]. Thus, reliance solely on clinical assessment is insufficient, and constantly high fecal calprotectin concentration during therapy warrants endoscopic evaluation also in children. It should be noted that increased fecal calprotectin level does not discriminate between disease relapse and intestinal infection[32].
Blood hemoglobin levels did not significantly alter during the induction phase, but the median ESR decreased during the induction phase by week 2. However, 39% of the patients had normal ESR at baseline, and in these patients, ESR is not applicable for assessment of therapeutic response. In children with IBD, serum C-reactive protein (CRP) is seldom increased, and disappointingly, the measurement of high-sensitivity CRP does not bring additional benefit for the assessment of disease activity[33]. Thus, CRP levels were not measured systematically in the present study. It has also been shown in adult IBD that CRP is a poor marker in mild to moderate disease[34], and performance of fecal calprotectin is significantly better[6].
As in many pediatric studies, one of the major limitations of the present study was the small size of the study group. The majority of the patients had CD but as there were only 13 cases of UC, comparisons related to diagnosis of IBD should be interpreted with caution. Most patients with CD presented with ileocolitis, and the numbers of patients with terminal ileal disease or CD colitis were too small to allow proper comparisons related to therapeutic response to infliximab therapy.
In conclusion, fecal surrogate markers may provide objective and non-invasive means to determine the response to infliximab in individual patients early in treatment. Also, fecal calprotectin is more reliable than clinical activity indices or blood-borne markers of inflammation. It may be possible to identify responding patients by a rapid drop in fecal calprotectin levels, which can be seen already at week 2. By week 6, little improvement is evident and some patients even appear to lose their therapeutic response. Based on our results, fecal calprotectin is a promising marker for evaluating patient response to TNF-α antagonist therapy and may offer a tool for identifying responding patients at an early stage, for more efficient targeting of treatment.
ACKNOWLEDGMENTS
We thank Ms Anne Nikkonen, RN and Sari Honkanen, RN for excellent assistance in gathering the patient data.
COMMENTS
Background
In pediatric patients, tumor necrosis factor (TNF)-α antagonists have emerged for therapy of severe inflammatory bowel disease (IBD), in patients who do not respond to conventional treatment. In children, endoscopy is an invasive procedure, which limits its use in follow-up. Fecal calprotectin is a surrogate marker for the presence of intestinal inflammation and thus provides a non-invasive means to assess disease activity in children.
Research frontiers
The recent development of easily applicable fecal surrogate markers for intestinal inflammation has provided new means for objective assessment of disease activity and treatment response in chronic IBD, a disease becoming more prevalent among children. When compared to clinical scores and serum inflammatory markers, fecal calprotectin is the most accurate tool to detect the presence of active mucosal inflammation in the intestine, and it is easily applicable to pediatric clinical practice.
Innovations and breakthroughs
This is believed to be the first pediatric study to follow fecal calprotectin levels during the induction phase of therapy with TNF-α antagonist agent infliximab. The study showed that, in one third of pediatric patients, fecal calprotectin level normalized by week 2. However, in two thirds of the patients, fecal calprotectin levels stayed elevated by week 6, suggesting incomplete mucosal healing.
Applications
Based on the results, fecal calprotectin is a promising marker for objective evaluation of patient response to TNF-α antagonist therapy and may offer a tool for identifying responding patients at an early stage, for more efficient targeting of treatment. The long-term treatment outcome in pediatric patients related to fecal calprotectin levels after induction therapy warrants further study.
Terminology
IBD consists of Crohn’s disease, ulcerative colitis and indeterminate colitis, and is a chronic illness that affects the intestines, with a partly TNF-α-driven inflammation that is effectively abated by TNF-α antagonists such as infliximab. Fecal calprotectin is a neutrophil-derived marker of inflammation that is present in the stools, and is a reliable surrogate for endoscopic evaluation of disease activity.
Peer review
The authors prospectively evaluated the therapeutic response in pediatric IBD patients during introduction to infliximab reflected in fecal calprotectin levels. It is a relevant study and the paper is well presented.
Footnotes
Supported by The Finnish Pediatric Research Foundation; the Päivikki and Sakari Sohlberg Foundation; the Mary and Georg C Ehrnrooth Foundation; and the Helsinki University Central Hospital Research Fund
Peer reviewers: Won Ho Kim, MD, Professor, Department of Internal Medicine, Yonsei Uiversity College of Medicine, 134 Shinchon-dong Seodaemun-ku, Seoul 120-752, South Korea; Dr. Charles B Ferguson, MRCP, Department of Gastroenterology, Belfast City Hospital, 51 Lisburn Road, Belfast BT9 7AB, United Kingdom
S- Editor Tian L L- Editor Kerr C E- Editor Li JY
References
- 1.Røseth AG, Aadland E, Jahnsen J, Raknerud N. Assessment of disease activity in ulcerative colitis by faecal calprotectin, a novel granulocyte marker protein. Digestion. 1997;58:176–180. doi: 10.1159/000201441. [DOI] [PubMed] [Google Scholar]
- 2.Bunn SK, Bisset WM, Main MJ, Gray ES, Olson S, Golden BE. Fecal calprotectin: validation as a noninvasive measure of bowel inflammation in childhood inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2001;33:14–22. doi: 10.1097/00005176-200107000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Fagerberg UL, Lööf L, Lindholm J, Hansson LO, Finkel Y. Fecal calprotectin: a quantitative marker of colonic inflammation in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2007;45:414–420. doi: 10.1097/MPG.0b013e31810e75a9. [DOI] [PubMed] [Google Scholar]
- 4.Canani RB, Terrin G, Rapacciuolo L, Miele E, Siani MC, Puzone C, Cosenza L, Staiano A, Troncone R. Faecal calprotectin as reliable non-invasive marker to assess the severity of mucosal inflammation in children with inflammatory bowel disease. Dig Liver Dis. 2008;40:547–553. doi: 10.1016/j.dld.2008.01.017. [DOI] [PubMed] [Google Scholar]
- 5.Quail MA, Russell RK, Van Limbergen JE, Rogers P, Drummond HE, Wilson DC, Gillett PM. Fecal calprotectin complements routine laboratory investigations in diagnosing childhood inflammatory bowel disease. Inflamm Bowel Dis. 2009;15:756–759. doi: 10.1002/ibd.20820. [DOI] [PubMed] [Google Scholar]
- 6.Langhorst J, Elsenbruch S, Koelzer J, Rueffer A, Michalsen A, Dobos GJ. Noninvasive markers in the assessment of intestinal inflammation in inflammatory bowel diseases: performance of fecal lactoferrin, calprotectin, and PMN-elastase, CRP, and clinical indices. Am J Gastroenterol. 2008;103:162–169. doi: 10.1111/j.1572-0241.2007.01556.x. [DOI] [PubMed] [Google Scholar]
- 7.Bunn SK, Bisset WM, Main MJ, Golden BE. Fecal calprotectin as a measure of disease activity in childhood inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2001;32:171–177. doi: 10.1097/00005176-200102000-00015. [DOI] [PubMed] [Google Scholar]
- 8.Gisbert JP, McNicholl AG. Questions and answers on the role of faecal calprotectin as a biological marker in inflammatory bowel disease. Dig Liver Dis. 2009;41:56–66. doi: 10.1016/j.dld.2008.05.008. [DOI] [PubMed] [Google Scholar]
- 9.Walker TR, Land ML, Kartashov A, Saslowsky TM, Lyerly DM, Boone JH, Rufo PA. Fecal lactoferrin is a sensitive and specific marker of disease activity in children and young adults with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2007;44:414–422. doi: 10.1097/MPG.0b013e3180308d8e. [DOI] [PubMed] [Google Scholar]
- 10.Kolho KL, Raivio T, Lindahl H, Savilahti E. Fecal calprotectin remains high during glucocorticoid therapy in children with inflammatory bowel disease. Scand J Gastroenterol. 2006;41:720–725. doi: 10.1080/00365520500419623. [DOI] [PubMed] [Google Scholar]
- 11.Sipponen T, Kolho KL. Faecal calprotectin in children with clinically quiescent inflammatory bowel disease. Scand J Gastroenterol. 2010;45:872–877. doi: 10.3109/00365521003782389. [DOI] [PubMed] [Google Scholar]
- 12.Sipponen T, Savilahti E, Kärkkäinen P, Kolho KL, Nuutinen H, Turunen U, Färkkilä M. Fecal calprotectin, lactoferrin, and endoscopic disease activity in monitoring anti-TNF-alpha therapy for Crohn’s disease. Inflamm Bowel Dis. 2008;14:1392–1398. doi: 10.1002/ibd.20490. [DOI] [PubMed] [Google Scholar]
- 13.Sipponen T, Björkesten CG, Färkkilä M, Nuutinen H, Savilahti E, Kolho KL. Faecal calprotectin and lactoferrin are reliable surrogate markers of endoscopic response during Crohn’s disease treatment. Scand J Gastroenterol. 2010;45:325–331. doi: 10.3109/00365520903483650. [DOI] [PubMed] [Google Scholar]
- 14.Buderus S, Boone J, Lyerly D, Lentze MJ. Fecal lactoferrin: a new parameter to monitor infliximab therapy. Dig Dis Sci. 2004;49:1036–1039. doi: 10.1023/b:ddas.0000034568.69407.47. [DOI] [PubMed] [Google Scholar]
- 15.Hyams J, Crandall W, Kugathasan S, Griffiths A, Olson A, Johanns J, Liu G, Travers S, Heuschkel R, Markowitz J, et al. Induction and maintenance infliximab therapy for the treatment of moderate-to-severe Crohn’s disease in children. Gastroenterology. 2007;132:863–873; quiz 1165-1166. doi: 10.1053/j.gastro.2006.12.003. [DOI] [PubMed] [Google Scholar]
- 16.Turner D, Mack D, Leleiko N, Walter TD, Uusoue K, Lech ST, Day AS, Crandall W, Silverberg MS, Markowitz J, et al. Severe pediatric ulcerative colitis: a prospective multicenter study of outcome and predictors of response. Gastroenterology. 2010;138:2282–2291. doi: 10.1053/j.gastro.2010.02.047. [DOI] [PubMed] [Google Scholar]
- 17.Hyams JS, Lerer T, Griffiths A, Pfefferkorn M, Stephens M, Evans J, Otley A, Carvalho R, Mack D, Bousvaros A, Rosh J, Grossman A, Tomer G, Kay M, Crandall W, Oliva-Hemker M, Keljo D, LeLeiko N, Markowitz J; Pediatric Inflammatory Bowel Disease Collaborative Research Group. Outcome following infliximab therapy in children with ulcerative colitis. Am J Gastroenterol. 2010;105:1430–1436. doi: 10.1038/ajg.2009.759. [DOI] [PubMed] [Google Scholar]
- 18.Lennard-Jones JE. Classification of inflammatory bowel disease. Scand J Gastroenterol Suppl. 1989;170:2–6; discussion 16-19. doi: 10.3109/00365528909091339. [DOI] [PubMed] [Google Scholar]
- 19.Berni Canani R, Rapacciuolo L, Romano MT, Tanturri de Horatio L, Terrin G, Manguso F, Cirillo P, Paparo F, Troncone R. Diagnostic value of faecal calprotectin in paediatric gastroenterology clinical practice. Dig Liver Dis. 2004;36:467–470. doi: 10.1016/j.dld.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 20.Haapamaki J, Roine RP, Sintonen H, Kolho K-L. Health-related quality of life in paediatric patients with inflammatory bowel disease. J Paediatr Child Health. 2011;47:832–837. doi: 10.1111/j.1440-1754.2011.02034.x. [DOI] [PubMed] [Google Scholar]
- 21.Ruemmele FM, Lachaux A, Cézard JP, Morali A, Maurage C, Giniès JL, Viola S, Goulet O, Lamireau T, Scaillon M, et al. Efficacy of infliximab in pediatric Crohn’s disease: a randomized multicenter open-label trial comparing scheduled to on demand maintenance therapy. Inflamm Bowel Dis. 2009;15:388–394. doi: 10.1002/ibd.20788. [DOI] [PubMed] [Google Scholar]
- 22.Hyams JS, Lerer T, Griffiths A, Pfefferkorn M, Kugathasan S, Evans J, Otley A, Carvalho R, Mack D, Bousvaros A, et al. Long-term outcome of maintenance infliximab therapy in children with Crohn’s disease. Inflamm Bowel Dis. 2009;15:816–822. doi: 10.1002/ibd.20845. [DOI] [PubMed] [Google Scholar]
- 23.McGinnis JK, Murray KF. Infliximab for ulcerative colitis in children and adolescents. J Clin Gastroenterol. 2008;42:875–879. doi: 10.1097/MCG.0b013e3181354417. [DOI] [PubMed] [Google Scholar]
- 24.Kolho KL, Ruuska T, Savilahti E. Severe adverse reactions to Infliximab therapy are common in young children with inflammatory bowel disease. Acta Paediatr. 2007;96:128–130. doi: 10.1111/j.1651-2227.2007.00042.x. [DOI] [PubMed] [Google Scholar]
- 25.Stephens MC, Shepanski MA, Mamula P, Markowitz JE, Brown KA, Baldassano RN. Safety and steroid-sparing experience using infliximab for Crohn’s disease at a pediatric inflammatory bowel disease center. Am J Gastroenterol. 2003;98:104–111. doi: 10.1111/j.1572-0241.2003.07161.x. [DOI] [PubMed] [Google Scholar]
- 26.Røseth AG, Aadland E, Grzyb K. Normalization of faecal calprotectin: a predictor of mucosal healing in patients with inflammatory bowel disease. Scand J Gastroenterol. 2004;39:1017–1020. doi: 10.1080/00365520410007971. [DOI] [PubMed] [Google Scholar]
- 27.Baert F, Moortgat L, Van Assche G, Caenepeel P, Vergauwe P, De Vos M, Stokkers P, Hommes D, Rutgeerts P, Vermeire S, et al. Mucosal healing predicts sustained clinical remission in patients with early-stage Crohn’s disease. Gastroenterology. 2010;138:463–468; quiz 463-468. doi: 10.1053/j.gastro.2009.09.056. [DOI] [PubMed] [Google Scholar]
- 28.Ardizzone S, Cassinotti A, Duca P, Mazzali C, Penati C, Manes G, Marmo R, Massari A, Molteni P, Maconi G, et al. Mucosal healing predicts late outcomes after the first course of corticosteroids for newly diagnosed ulcerative colitis. Clin Gastroenterol Hepatol. 2011;9:483–489.e3. doi: 10.1016/j.cgh.2010.12.028. [DOI] [PubMed] [Google Scholar]
- 29.Regueiro M, Siemanowski B, Kip KE, Plevy S. Infliximab dose intensification in Crohn’s disease. Inflamm Bowel Dis. 2007;13:1093–1099. doi: 10.1002/ibd.20177. [DOI] [PubMed] [Google Scholar]
- 30.Wu EQ, Mulani PM, Yu AP, Tang J, Pollack PF. Loss of treatment response to infliximab maintenance therapy in Crohn’s disease: a payor perspective. Value Health. 2008;11:820–829. doi: 10.1111/j.1524-4733.2008.00335.x. [DOI] [PubMed] [Google Scholar]
- 31.Sipponen T, Savilahti E, Kolho KL, Nuutinen H, Turunen U, Färkkilä M. Crohn’s disease activity assessed by fecal calprotectin and lactoferrin: correlation with Crohn’s disease activity index and endoscopic findings. Inflamm Bowel Dis. 2008;14:40–46. doi: 10.1002/ibd.20312. [DOI] [PubMed] [Google Scholar]
- 32.Kaiser T, Langhorst J, Wittkowski H, Becker K, Friedrich AW, Rueffer A, Dobos GJ, Roth J, Foell D. Faecal S100A12 as a non-invasive marker distinguishing inflammatory bowel disease from irritable bowel syndrome. Gut. 2007;56:1706–1713. doi: 10.1136/gut.2006.113431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sidoroff M, Karikoski R, Raivio T, Savilahti E, Kolho KL. High-sensitivity C-reactive protein in paediatric inflammatory bowel disease. World J Gastroenterol. 2010;16:2901–2906. doi: 10.3748/wjg.v16.i23.2901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Solem CA, Loftus EV, Tremaine WJ, Harmsen WS, Zinsmeister AR, Sandborn WJ. Correlation of C-reactive protein with clinical, endoscopic, histologic, and radiographic activity in inflammatory bowel disease. Inflamm Bowel Dis. 2005;11:707–712. doi: 10.1097/01.mib.0000173271.18319.53. [DOI] [PubMed] [Google Scholar]