

Abstract
This is an article reporting the largest phyllodes tumor and the role of radiotherapy in patients of phyllodes tumor of breast, based on Medline search for articles in English language using keywords “role of radiotherapy in phyllodes tumor of breast”. 32 years female presented with a lump in right breast since last 4 months. This was the second recurrence of similar lump in last 6 years. Biopsy from the lump proved to be cystosarcoma phyllodes. Radical Mastectomy with level I node sampling and reconstruction with Latissimus Dorsi Myocutaneous flap was done as a curative procedure. The tumor measured exactly to be 50 × 25.2 × 16.4 cm in size and 15 kg in weight. Proliferation markers like Ki- 67 and p53 were in the range of 1-2% and 3-4% respectively. Histopathological diagnosis of the tumor was borderline phyllodes tumor. Patient had an uneventful postoperative course and is presently on three monthly follow up since 1 year.
Introduction
The phyllodes tumor, originally described by Johannes Muller in 1838, has presented a diagnostic and treatment dilemma for physicians since its original description. Classically, the name cystosarcoma phyllodes was assigned because of the tumor’s fleshy appearance and tendency to contain macroscopic cysts. The term, however, is a misnomer as these tumors are usually benign. Phyllodes tumor is the currently accepted nomenclature according to the World Health Organization (WHO) [2].
Phyllodes tumors are biphasic fibroepithelial neoplasms of breast [2] which are generally classified as benign, borderline and malignant [3]. Borderline tumors have great potential for local recurrence. They make up 0.3 to 0.5% of female breast tumors [11] and have an incidence of about 2.1 per million.
Phyllodes tumors are sharply demarcated from surrounding tissue which is compressed and distorted. Connective tissue composes of the bulk of these tumors which have mixed gelatinous, solid and cystic areas. Most malignant phyllodes tumors contain liposarcomatous/rhabdomyosarcomatous elements rather than fibrosarcomatous component. Evaluation of number of mitosis may help in diagnosis of malignant tumor [3]. While the surgical management of the phyllodes tumor has been addressed many times in the literature, few reports have specifically commented on the giant phyllodes tumor, an entity that presents the surgeon with several unique management problems. The arbitrary cut off point for designation as a giant phyllodes tumor is 10 cm [1].
Usually wide local excision of the tumor with 1 cm [2] breast margin may suffice as the treatment but larger malignant variety may require tailoring of treatment pertaining to that individual case and number of recurrences. Radiotherapy may have a role in the treatment of phyllodes tumor depending of the number of recurrences, mitotic index, bulky tumor, status of the resection margins p53 and Ki67 expression [10].
Case Report
Thirty-two years female presented with a lump in right breast since last 4 months. This was the second recurrence in last 6 years.
On clinical examination right breast was hugely enlarged to 50 × 20 × 20 cm with altered contour and enlarged nipple areola complex. The breast was large enough to cause scoliotic changes in thoracic spine. Biopsy from the lump proved to be cystosarcoma phyllodes.
As it was the second recurrence and third surgery for the patient simple Mastectomy with level 1 clearance and latissimus dorsi myocutaneous flap reconstruction was planned for the patient as curative procedure.
Intra operatively Pectoralis Major, Pectoralis Minor, Serratus Anterior were infiltrated by the tumor, also the axillary lymphnodes were found to be enlarged. Hence local wide excision (i.e. removal of the three muscles) with level I axillary lymph node sampling and Latissimus Dorsi myocutaneous flap reconstruction was done.
The tumor specimen measured exactly to be 50 × 25.2 × 16.4 in size and weight of 15 kg with closest margin of resection 0.7 cm away from the tumor.
Microscopically the lesion was borderline phyllodes tumor with moderate pleomorphism and 3–4 mitosis per ten high power field with focal areas showing 6–8 mitosis per ten high power field. Areas of myxoid degeneration were present without any lymphovascular invasion. There were three lymphnodes in the specimen which were free from the tumor tissue. Proliferation markers like Ki- 67 and p53 were in the range of 1-2% and 3-4% respectively.
Patient had a uneventful post operative course and is presently on three monthly follow up since 1 year (Figs. 1, 2, 3, 4, 5 and 6).
Fig. 1.

Giant phyllodes tumor- Pre operative photograph
Fig. 2.

Giant phyllodes tumor- Pre operative photograph
Fig. 3.
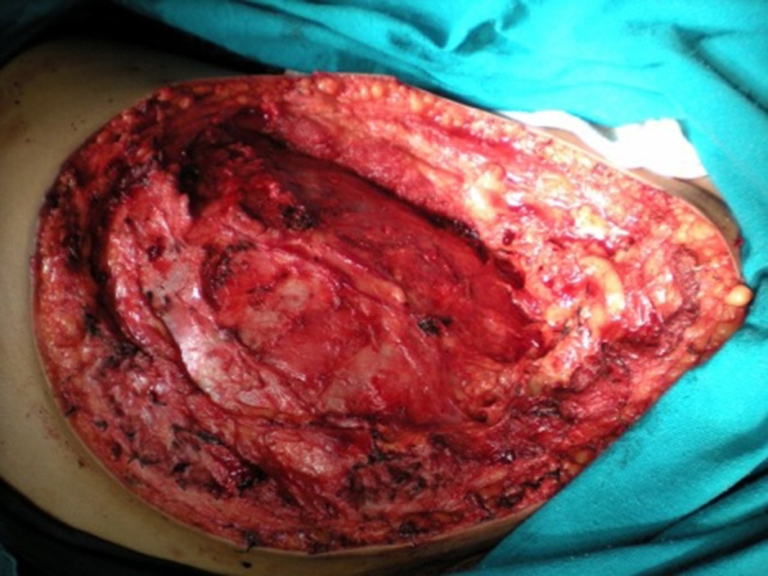
Intra operative photograph after resection of tumor with pectoralis major, minor and serratus anterior
Fig. 4.

Post Operative outcome
Fig. 5.
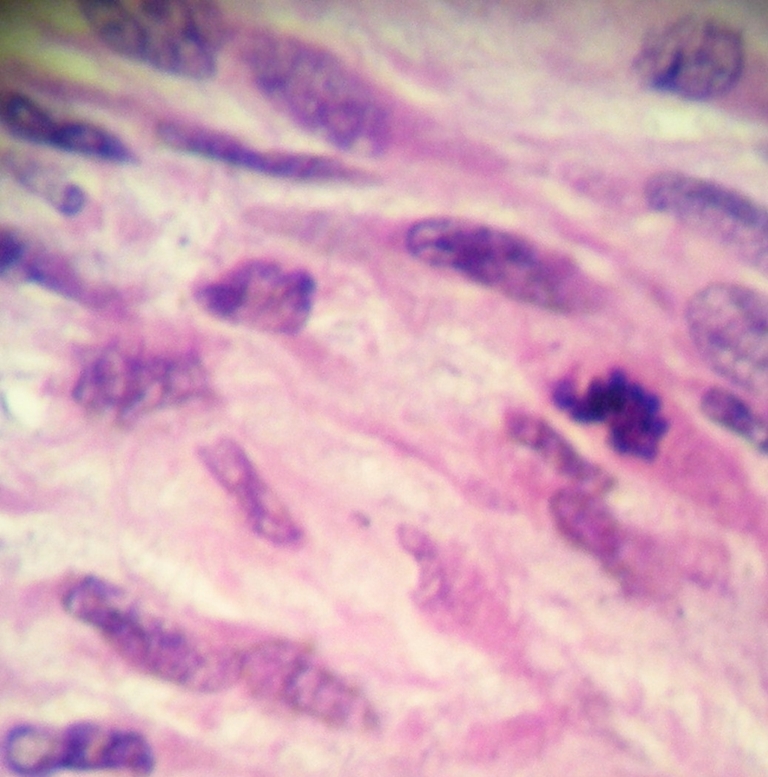
Microsopic view
Fig. 6.

Microsopic view
Discussion
Though surgery has been an inseparable part in the management of the phyllodes tumors ever since they were first described, due to rarity of the condition there has been no fixed protocol in the optimal management of the disease.
Here is the review of some studies highlighting the role of radiotherapy in phyllodes tumor of breast (Table 1).
Table 1.
Overview of various studies highlighting the role of radiotherapy in phyllodes tumor
| Study | Number of patients | Criteria for giving radiotherapy | Inference (for using radiotherapy: yes/no/equivocal) |
|---|---|---|---|
| Chaney AW et al. [4] | 08 | bulky tumor volume, positive margins, recurrence, and/or malignant histology. | YES |
| Belkac’emi etal [5] | 39 | Malignant and borderline histology | YES |
| Macdonald OK et al. [6] | 821 | Malignant and borderline histology | EQUIVOCAL |
| Saumarova’R et al. [8] | 25 | Malignant histology | YES |
| Stranzl H et al. [9] | 06 | Malignant histology | YES |
| Erhan Y et al. [10] | 21 | high mitotic rate, p53 and Ki-67 fraction | YES |
| Chen WH et al. [7] | 172 | Malingnant and borderline histology | EQUIVOCAL |
Conclusion
Radiotherapy is useful in a subset of patients described. Though the review of various studies indicate towards the importance of radiotherapy in the management of the phyllodes tumor of breast, but still a randomized controlled trial with adequate sample size would be required to derive a fixed treatment protocol and dosage of radiotherapy for the management of the same. Rarity of the condition is the major obstacle.
In author’s opinion based on the review of these studies, radiotherapy is a viable option and should be utilized in patients with adverse histology and recurrent tumors.
References
- 1.Tan P-H, Jayabaskar T, Chuah K-L, Lee H-Y, Tan Y, Hilmy M, et al. Phyllodes tumors of the breast the role of pathologic parameters. Am J Clin Pathol. 2005;123:529–540. doi: 10.1309/U6DVBFM81MLJC1FN. [DOI] [PubMed] [Google Scholar]
- 2.Liang MI, Ramaswamy B, Patterson CC, McKelvey MT, Cordillo G, Nuovo GJ, Carson WE., III Giant breast tumors: surgical management of phyllodes tumors, potential for reconstructive surgery and review of literature. World Jr of Surgical Oncology. 2008;6:117. doi: 10.1186/1477-7819-6-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khan SA, Badve S. Phyllodes tumors of breast. Curr Treat options Oncol. 2001;2:139–147. doi: 10.1007/s11864-001-0056-y. [DOI] [PubMed] [Google Scholar]
- 4.Chaney AW, Pollack A, McNeese MD, Zagars GK. Adjuvant radiotherapy for phyllodes tumor of breast. Radiat Oncol Investig. 1998;6(6):264–7. doi: 10.1002/(SICI)1520-6823(1998)6:6<264::AID-ROI3>3.0.CO;2-J. [DOI] [PubMed] [Google Scholar]
- 5.Belkacémi Y, Bousquet G, et al. Phyllodes tumor of the breast. Int J Radiat Oncol Biol Phys. 2008;70(2):492–500. doi: 10.1016/j.ijrobp.2007.06.059. [DOI] [PubMed] [Google Scholar]
- 6.Macdonald OK, Lee CM, Tward JD, Chappel CD, Gaffney DK. Malignant phyllodes tumor of the female breast: association of primary therapy with cause-specific survival from the Surveillance, Epidemiology, and End Results (SEER) program. Cancer. 2006;107(9):2127–33. doi: 10.1002/cncr.22228. [DOI] [PubMed] [Google Scholar]
- 7.Chen WH, Cheng SP, Tzen CY, Yang TL, Jeng KS, Liu CL, Liu TP. Surgical treatment of phyllodes tumors of the breast: retrospective review of 172 cases. J Surg Oncol. 2005;91(3):185–94. doi: 10.1002/jso.20334. [DOI] [PubMed] [Google Scholar]
- 8.Soumarová R, Seneklová Z, Horová H, Vojkovská H, Horová I, Budíková M, Růzicková J, Jezková B. Retrospective analysis of 25 women with malignant cystosarcoma phyllodes—treatment results. Arch Gynecol Obstet. 2004;269(4):278–81. doi: 10.1007/s00404-003-0593-7. [DOI] [PubMed] [Google Scholar]
- 9.Stranzl H, Peintinger F, Hackl A. Phyllodes tumor: an unexpected tumor of the breast. A report on six patients. Strahlenther Onkol. 2004;180(3):148–51. doi: 10.1007/s00066-004-1182-9. [DOI] [PubMed] [Google Scholar]
- 10.Erhan Y, Zekioglu O, Ersoy O, Tugan D, Aydede H, Sakarya A, Kapkaç M, Ozdemir N, Ozbal O, Erhan Y. p53 and Ki-67 expression as prognostic factors in cystosarcoma phyllodes. Breast J. 2002;8(1):38–44. doi: 10.1046/j.1524-4741.2002.08008.x. [DOI] [PubMed] [Google Scholar]
- 11.Rowell MD, Perry RR, Jeng-Gwang H, Barranco SC. Phyllodes tumors. Am J Surg. 1993;165:376–79. doi: 10.1016/S0002-9610(05)80849-9. [DOI] [PubMed] [Google Scholar]