

Abstract
Introduction: Encouraged by the change in licensing regulations the practical professional skills in Germany received a higher priority and are taught in medical schools therefore increasingly. This created the need to standardize the process more and more. On the initiative of the German skills labs the German Medical Association Committee for practical skills was established and developed a competency-based catalogue of learning objectives, whose origin and structure is described here.
Goal of the catalogue is to define the practical skills in undergraduate medical education and to give the medical schools a rational planning basis for the necessary resources to teach them.
Methods: Building on already existing German catalogues of learning objectives a multi-iterative process of condensation was performed, which corresponds to the development of S1 guidelines, in order to get a broad professional and political support.
Results: 289 different practical learning goals were identified and assigned to twelve different organ systems with three overlapping areas to other fields of expertise and one area of across organ system skills. They were three depths and three different chronological dimensions assigned and the objectives were matched with the Swiss and the Austrian equivalent.
Discussion: This consensus statement may provide the German faculties with a basis for planning the teaching of practical skills and is an important step towards a national standard of medical learning objectives.
Looking ahead: The consensus statement may have a formative effect on the medical schools to teach practical skills and plan the resources accordingly.
Keywords: Skills, Practical skills, Clinical Skills, medical education, Consensus methods, Delphi Survey, Objectives, Outcomes, Competencies
Abstract
Einleitung: Angestoßen durch die Änderung der Approbationsordnung haben die berufspraktischen Kompetenzen in Deutschland eine höhere Priorität erhalten und werden in den medizinischen Fakultäten deswegen vermehrt vermittelt. Dadurch entstand die Notwendigkeit, den Prozess mehr und mehr zu standardisieren. Auf Initiative der deutschsprachigen Skills Labs wurde der GMA-Ausschuss für praktische Fertigkeiten gegründet, der einen kompetenzbasierten Lernzielkatalog entwickelte, dessen Entstehung und Struktur hier beschrieben wird.
Ziel des Kataloges ist es, die praktischen Fertigkeiten im Medizinstudium zu definieren und damit den Fakultäten eine rationale Planungsgrundlage für die zur Vermittlung praktischer Fertigkeiten notwendigen Ressourcen zu geben.
Methodik: Aufbauend auf schon vorhandenen deutschsprachigen Lernzielkatalogen wurde mittels einem mehrfach iterativem Kondensationsprozesses, der der Erarbeitung von S1-Leitlinien entspricht, vorgegangen, um eine breite fachliche und politische Abstützung zu erhalten.
Ergebnisse: Es wurden 289 verschiedene praktische Lernziele identifiziert, die zwölf verschiedenen Organsystemen, drei Grenzbereichen zu anderen Kompetenzbereichen und einem Bereich mit organsystemübergreifenden Fertigkeiten zugeordnet. Sie wurden drei verschiedenen zeitlichen und drei verschiedenen Tiefendimensionen zugeordnet und mit dem Schweizer und dem Österreichischem Pendant abgeglichen.
Diskussion: Das vorliegende Konsensusstatement kann den deutschen Fakultäten eine Grundlage zur Planung der Vermittlung praktischer Fertigkeiten bieten und bildet einen wichtigen Schritt zu einem nationalen Standard medizinischer Lernziele.
Blick in die Zukunft: Das Konsensusstatement soll einen formativen Effekt auf die medizinischen Fakultäten haben, ihre praktischen Unterrichtsinhalte entsprechend zu vermitteln und die Ressourcen danach zu planen.
Introduction
Due to the developments in medical education in recent years, triggered by the amendment to the Licensing Regulations in Germany [1], the balance of the curriculum has shifted in favour of communicative [http://www.impp.de] and practical vocational skills and thus also in favour of the acquisition of practical skills. As the Licensing Regulations state, “The aim of medical education are scientifically and practically trained doctors who are capable of practising medicine independently, specialisation and CPD.” And a little further on in §1, Section 1 it also states “... the general knowledge, abilities and skills in diagnostics, treatment, health promotion, prevention and rehabilitation needed in medical practice, ...”.
The acquisition of practical skills only played a rather minor role in Germany until that point. Although the practical skills and mental skills were already stated in the 7th Amendment of the ÄAppO [2] (§ 1 Para 1, Second Dashed Item), no systematic assessments were carried out.
Therefore virtually only cognitive content were conducive (formative) to the degree course, on which not only students but also the medical faculties placed their emphasis. This occurred frequently, as the results of the Written State Exams are regularly published by the Institute of Medical and Pharmaceutical Examination Questions (IMPP), thus encouraging competitive comparison [http://www.impp.de], in contrast to the acquisition of practical skills. Practical skills were also tested only sporadically in the oral parts of the State Exam. With the introduction of the current 2002 ÄAppO [1], the importance of teaching and examining of practical skills increased. The weighting of the oral practical examination at the end of the degree course increased through the various amendments from 33% (2nd Part of the Medical Examination, 7th Amendment ÄAppO of 1989) to 50% (M2 now). The introduction of graded block placements (bedside teaching (UaK)) also increased the pressure on faculties to address the acquisition of practical teaching content much more comprehensively.
These conditions gave those who considered practical skills important good arguments to support the expansion of the systematic teaching of practical, application-oriented teaching content.
The tuition fees which had been introduced in some states also had a supporting role because they contributed to the construction of training centres for medical skills (skills labs) and thus enabled standardised practical training [3].
The changed framework conditions in the ÄAppO and the general increase in the pressure from health policies toward practice-related skills led to medical schools introducing more OSCEs (Objective Structured Clinical Examinations [4]) as the faculties’ practical examinations, although this would already have been possible under the old Licensing Regulations [5]. According to data collected by Kruppa et al, in the middle of 2008, 78% (28 of 36) of all German medical faculties already had OSCEs and 83% had implemented the use of simulated or standardised patients (30 of 36) [6].
Due to the variety of learned and taught practical skills which appear in the faculty OSCEs, the need arose to better define the skills both for examiners and students and standardise and objectify both the teaching of the curriculum and the examinations.
Relevant literature was published and released as a standard for OSCEs at individual faculties [7], [8].
Through an initiative of the heads of the skills labs in Vienna, Berlin and Cologne in 2007 a series of mini-symposia was launched in the German speaking countries (Germany and Switzerland). The Skills Lab Symposia (Berlin in 2007, Vienna in 2007, Cologne in 2008, Aachen in 2009, Munster in 2010 and Würzburg in 2011) initially took place at half-year intervals and since 2008 on an annual basis as a spring conference. This initiative led to the formation of the GMA Committee on Practical Skills in November 2007 through the decision of the GMA Board and which met for the first time in Cologne in April 2008.
In the course of the Cologne Lab Skills Symposium, the Committee decided to create a competence-based learning target catalogue for practical skills in Germany. Exemplary international models included the Swiss Catalogue of Learning Objcetives (SCLO) [9] [http://www.smifk.ch as well the models this itself was based upon [10], [11], [12].
Similar developments simultaneously took place in Austria. Based on the SCLO, the Austrian Competence Catalogue for Medical Skills (ÖKÄF) was developed, which since May 2011 has been approved by all four Austrian medical universities and is currently being implemented into the curricula as a compulsory basis for degree course design [http://www.meduniwien.ac.at/bemaw/mue/downloads/oekaef.pdf].
In parallel the National Competency-based Learning Objectives Catalogue in Medicine (NKLM) continues to be developed by the GMA and the Medical Faculties’ Conference [13], continuously informed by results of the GMA Committee on Practical Skills. The nature of the NKLM, however, inherently offers a different point of view: peripheral technical skills and the aim of describing a minimum standard (currently 117 skills) largely dissolve the formerly close relationship of this consensus statement and the NKLM, even if overlaps remain. As this catalogue also makes reference to optional areas, this catalogues will more likely serve the faculties as a specific planning aid rather than the future NKLM.
Aims
The statement which hereinafter will be referred to as the Consensus Statement on Practical Skills describes the practical skills which medical students should learn. These serve to fulfill different aims:
It aims to describe the standard of practical skills which will be taught and learned in medical school. Both the depth of the individual learning objectives and the timing within the degree at which they are to be acquired are described.
It provides a guideline for planning local curricula regarding practical skills and help planners the skills implement them at appropriate places in the curriculum and examinations.
It should offer a rational basis for planning, accommodation, human and material resources at various stages of study.
In the following we will describe the process and the results and offer an outlook for the future.
Methods
The learning objectives catalogue was condensed based on the already available learning objectives catalogue of the medical faculties (Berlin (Reformed and Traditional Degree Course), Düsseldorf, Erlangen, Frankfurt, Freiburg, Göttingen, Kiel and Cologne) through several iterative reviews (see Table 1 (Tab. 1)). The chosen approach corresponds to a focus group approach for the development of S1-AWMF guidelines [14], [15].
Table 1. Chronology of the consultations for the competence-based learning targets catalogue of the GMA-Committee on Practical Skills.
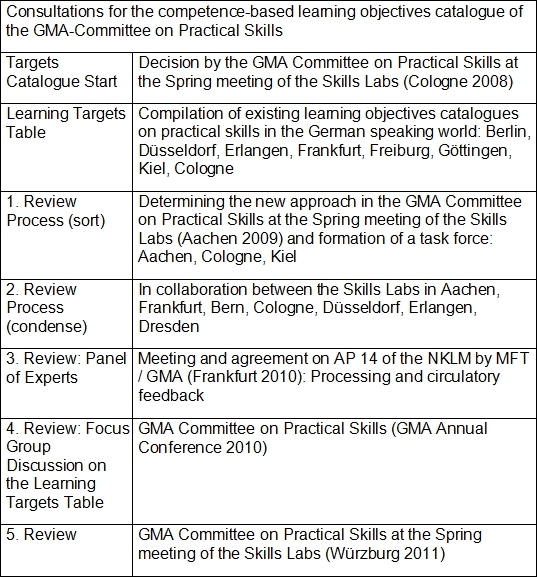
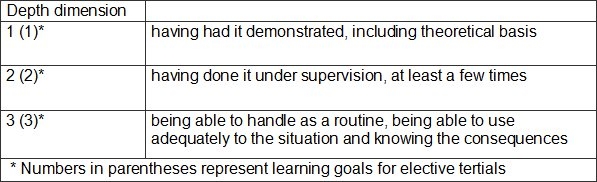
During the Spring Conference 2009 in Aachen, the GMA Committee on Practical Skills formed a task force which coordinated the compilation of existing learning objectives catalogues on practical skills in German speaking countries. Duplications were removed and uniform nomenclature agreed in the first review process. This also set the deep dimensions which define to which depth the individual learning objectives will apply (see Table 2 (Tab. 2)). The committee has agreed on three depth dimensions, thereby also implying how teaching should be conducted to achieve these goals.
Table 2. Depth dimensions of the learning targets.
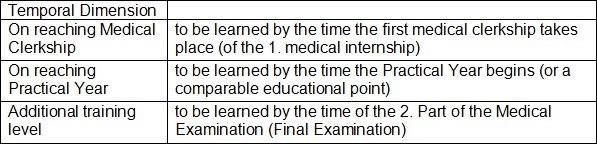
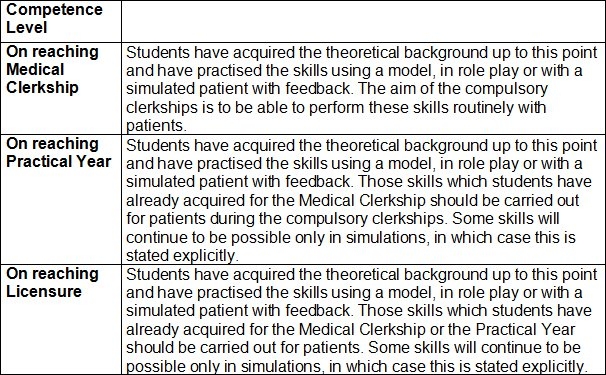
In parallel, based on the training steps from the skills training in Cologne, the points in time of a degree course at which these skills are to be acquired were fixed (see Table 3 (Tab. 3)).
Table 3. Temporal dimension: Point in time during degree course at which a learning target should have been reached.
The nomenclature of the learning objectives thus forms the framework of which learning objectives should be studied when and to what depth.
In co-operation between the skills labs in Aachen, Frankfurt, Bern, Cologne, Düsseldorf, Erlangen and Dresden the learning objectives were condensed and tidied up in terms of language and content in a second review process in smaller groups, which corresponded to the subject areas.
This was followed by a two-stage Delphi survey [16] by the working group of the NKLM of the MFT. The learning objectives of the Committee on Practical Skills were commented upon in terms of their dimensions and transferred into core and elective learning objectives by the working group of what is now known as Work Package 14 (Practical Skills) following the first working group meeting on 01.07.2010 in Frankfurt am Main (feedback from 8 of 10 participating university sites of the AP 14).
The differences arising from this survey where then revised and re-condensed at the meeting of the Committee on Practical Skills at the Bochum Annual Meeting of the GMA in September 2010 in focus group discussions.
Results
The four-stage process described here identified 289 different practical skills in medical studies which were divided into 12 organ systems (respiratory, musculoskeletal, blood/immune system, endocrine system, gastrointestinal tract, urinary/genital organs, skin, cardiovascular system, nervous system, mental health, sense organs, growth/aging), 3 contact areas with other areas of expertise (communications contact area, emergency medicine contact area, soft skills contact area) and an area of cross-organ system skills.
The learning objectives in the contact area of emergency medicine was extracted in a separate process from the consensus process AP 17 of the NKLM and the National Learning Objectives Catalogue of the German Society for Anaesthesiology and Intensive Care Medicine (DGAI) and adjusted to the guidelines of the Committee on Practical Skills.
Due to the complexity of the content, it was not possible to prevent overlaps totally in all areas. There were content-related reasons for the few remaining overlaps and they were thus considered to be tolerable.
The complete Table 6 can be viewed as a digital attachment .
For external validation, the table was compared with the Swiss and Austrian learning objectives catalogues and highlighted in the table with the appropriate level depth.
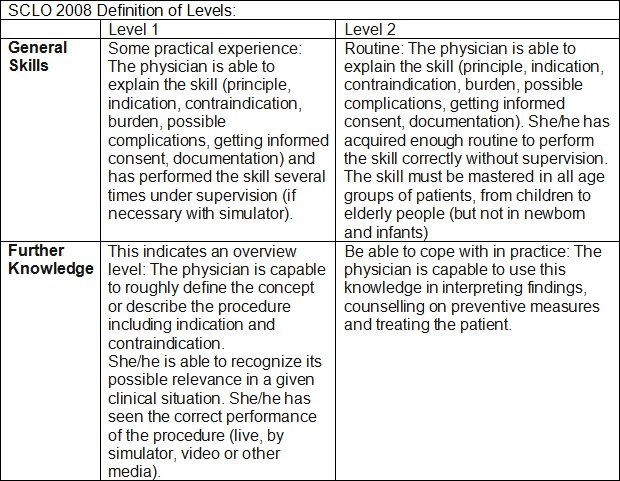
In the comparison with the Swiss learning objectives catalogue a slightly different definition of the depth dimensions (definition of levels) had to be observed as the Swiss system generally works with only two levels (see Table 4 (Tab. 4)). These were marked as GS1 and GS2 in the table. Under Further Knowledge those learning objectives of the previous Level 1+2 (2002 version [9] “only theory” and “seen or have had demonstrated”) were sorted which implied no practical student experience. These two levels correspond most closely to Level 1 of this learning target catalogue. The table lists the learning objectives as FK1 and FK2.
Table 4. Extract of the definitions of learning objectives levels for practical skills in the Swiss learning targets catalogue.
Also missing from the SCLO is the temporal dimension, since it only describes the outcomes after graduation. Thus the faculties decide independently when certain skills should be taught.
The Austrian Competence Level Catalogue for medical skills groups the learning objectives along a temporal dimension too, similar to the German catalogue (see Table 5 (Tab. 5)). In terms of depth dimensions, all learning objectives require personal practical experience at the lowest level, followed by the requirement of routine at the next higher level. The catalogue is limited to the mandatory minimum standards and in contrast to the catalogue presented here does not list elective areas.
Table 5. Temporal and depth dimensions of the learning objectives of the Austrian Competence Level Catalogue for medical skills.
Discussion
With this statement and the underlying competency-based learning objectives for practical skills for the first time German-speaking countries have a position paper which in a broad consultation process with the medical faculties describes the necessary practical skills at various stages of medical undergraduate studies. This statement can form the basis for the planning of practical skills in the curricula of German medical faculties, as well as providing an incentive for a revision of the Swiss and Austrian learning objectives catalogues.
It can suggest both to the learner and the tutor, as well as to planners on the meta-level, which skills should be taught and learned at which point and to what depth. The resulting German learning objectives catalogue for practical skills describes the core learning objectives which are based on the minimum requirements agreed in a German interdepartmental and interdisciplinary consensus regarding the practical skills of licensed doctors. This enables healthcare providers define a graduate standard, measured objectively at the end of a student’s degree course by the faculties and, for example, checked through OSCEs. The necessary personnel, accommodation and material (models, dummies, simulators) resources arising indirectly from the learning objectives and their depth level can thus give planners rational justifications for planning human and other resources locally in their own faculties.
The differences between the Swiss and the Austrians learning objectives should give cause for considering common long-term learning objectives and for minimising national differences or for deliberately maintaining national profiles.
This consensus statement in its present form is valid for two years and will be revised at that point.
Outlook
The procedure for the preparation of this catalogue for a German learning objectives catalogue for practical skills is equivalent to a focus group approach for the development of the AWMF S1 guidelines. In coordination with the GMA there are plans to publish the present consensus statement as a guideline for the acquisition of practical skills by the professional society. This can and should have a formative effect on faculties in aligning their practical teaching content with the guidelines and making the necessary personnel, accommodation and material resources available. It appears feasible to develop a German-language learning objectives catalogue with mandatory content together with Switzerland, Austria and Germany in the not too distant future in terms of all remaining substantive and structural differences.
Acknowledgement
We would like to thank to all those who have helped initiate, create, model, revise and finalise this learning objectives catalogue. Out special thanks to the GMA Committees on Practical Skills, for emergency medicine and for communication and social skills as well as the members of Work Package 14 of the National Competence-based Learning Objectives Catalogue (NKLM)*
Note
* The National Competence-based Learning Objectives Catalogue in Medicine (NKLM) is a cooperative project by the Medical Faculties’ Conference BRD (MFT) and the Society for Medical Education (GMA) (see http://www.nklm.org).
Competing interests
The authors declare that they have no competing interests.
Supplementary Material
References
- 1.Bundesministerium für Gesundheit. Approbationsordnung für Ärzte. BGBL. 2002;I(44.) [Google Scholar]
- 2.Bundesministerium für Gesundheit. 7. Verordnung zur Änderung der Approbationsordnung für Ärzte. BGBL. 1989;I:2549. [Google Scholar]
- 3.Segarra LM, Schwedler A, Weih M, Hahn EG, Schmidt A. Der Einsatz von medizinischen Trainingszentren für die Ausbildung zum Arzt in Deutschland, Österreich und der deutschsprachigen Schweiz. GMS Z Med Ausbild. 2008;25(2):Doc80. Available from: http://www.egms.de/de/journals/zma/2008-25/zma000564.shtml. [Google Scholar]
- 4.Harden RM, Gleeson FA. Assessment of clinical competence using an objective structured clinical examinaton (OSCE) Med Educ. 1979:41–54. doi: 10.1111/j.1365-2923.1979.tb00918.x. Available from: http://dx.doi.org/10.1111/j.1365-2923.1979.tb00918.x. [DOI] [PubMed] [Google Scholar]
- 5.Schnabel K, Scheffner D. Innovationsspielräume der Approbationsordnung für Ärzte. Med Ausbild. 2001;18:12–15. [Google Scholar]
- 6.Kruppa E, Jünger J, Nikendei Ch. Einsatz innovativer Lern- und Prüfungsmethoden an den medizinischen Fakultäten der Bundesrepublik Deutschland Eine aktuelle Bestandsaufnahme. Dtsch Med Wochenschr. 2009;134:371–372. doi: 10.1055/s-0028-1124008. [DOI] [PubMed] [Google Scholar]
- 7.Schnabel KP, Ahlers O, Dashti H, Georg W, Schwantes U. Ärztliche Fertigkeiten. Anamnese, Untersuchung, ausgewählte Anwendungsgebiete. 1. Aufl. Stuttgart: Wissenschaftliche Verlagsgesellschaft; 2009. [Google Scholar]
- 8.Schnabel K, Müller S. Vermittlung praktischer Fertigkeiten in der Pädiatrie. Am Beispiel der Curricula der Charité – Universitätsmedizin Berlin. Monatsschr Kinderheilkd. 2008;156:446–451. Available from: http://dx.doi.org/10.1007/s00112-008-1725-8. [Google Scholar]
- 9.Bloch R, Bürgi H. The Swiss Catalogue of Learning Objectives. Med Teach. 2002;24(2):144–150. doi: 10.1080/01421590220120759. Available from: http://dx.doi.org/10.1080/01421590220120759. [DOI] [PubMed] [Google Scholar]
- 10.Frank JR. The CanMEDS 2005 Physician Competency Framwork. Ottawa: The Royal College; 2005. Professional; pp. 23–24. Available from: http://meds.queensu.ca/medicine/obgyn/pdf/CanMEDS2005.booklet.pdf. [Google Scholar]
- 11.Metz JC, Verbeek-Weel AM, Huisjes HJ. Blueprint 2001: training of doctors in The Netherlands. Utrecht: NFU; 2001. Available from: http://www.nfu.nl/fileadmin/documents/BLUEPRINT-Training-of-doctors.pdf. [Google Scholar]
- 12.The Scottish Deans' Medical Curriculum Group. Learning Outcomes for the Medical Undergraduate in Scotland: A foundation for competent and reflective practitioners. Edinburgh: University of Edinburgh; 2000. Available from: http://www.scottishdoctor.org/resources/scotdoc1.pdf. [DOI] [PubMed] [Google Scholar]
- 13.Hahn EG, Fischer MR. Nationaler Kompetenzbasierter Lernzielkatalog Medizin (NKLM) für Deutschland: Zusammenarbeit der Gesellschaft für Medizinische Ausbildung (GMA) und des Medizinischen Fakultätentages (MFT) GMS Z Med Ausbild. 2009;26(3):Doc35. doi: 10.3205/zma000627. Available from: http://dx.doi.org/10.3205/zma000627. [DOI] [Google Scholar]
- 14.AWMF. Erarbeitung von Leitlinien für Diagnostik und Therapie. Methodische Empfehlungen ("Leitlinie für Leitlinien", Stand Dez. 2004) Düsseldorf: AWMF; 2004. Available from: http://leitlinien.net/ [Google Scholar]
- 15.Kopp IB. Projektskizze Leitlinien (Muster) Düsseldorf: AWMF; 2007. Available from: http://www.awmf.org/leitlinien/awmf-regelwerk/hilfen-werkzeuge/publikationen/leitlinien-manual.html. [Google Scholar]
- 16.Clayton, M Delphi: A technique to harness expert opinion for critical decision-making tasks in education. Educ Psychol. 1997;17(4):373–386. doi: 10.1080/0144341970170401. Available from: http://dx.doi.org/10.1080/0144341970170401. [DOI] [Google Scholar]
- 17.Kiessling C, Dieterich A, Fabry G, Hölzer H, Langewitz W, Mühlinghaus I, Pruskil S, Scheffer S, Schubert S. Basler Consensus Statement "Kommunikative und soziale Kompetenzen im Medizinstudium": Ein Positionspapier des GMA-Ausschusses Kommunikative und soziale Kompetenzen. GMS Z Med Ausbild. 2008;25(2):Doc83. Available from: http://www.egms.de/de/journals/zma/2008-25/zma000567.shtml. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.