

Introduction
The University for Applied Health Sciences was founded in Bochum in November 2009. It is the first government-run university which offers occupational therapy, speech therapy, physiotherapy, midwifery and care as bachelor degree programs at undergraduate level. During the initial phase, the intake capacity will be 400 students per year (about 1.300 students in total). The students will receive both a state qualification, which provides the basis for progression towards professional accreditation, and the academic degree Bachelor of Science. The “academisation” of these professions is innovative, albeit not internationally, and may become exemplary for a modern understanding of the health professions in Germany. For this to happen though, the academisation of the health professions in Germany needs to be legitimized and will only be considered useful if it contributes to a better health care for the population. The evaluation guidelines [1] given out by the Federal Ministry of Health mirror this, scrutinizing the impact of the model degree courses on the quality of healthcare. Thus, if the evaluation results of the first five model degree courses explicitly prove the added value of academic training, an essential step has been taken towards the academisation of further health professions.
After a very brief look at the development of academic medicine, we shall examine the academisation process of the health professions so far. This will be followed by an extensive attempt to describe fundamental aspects of the phenomenon “academisation” and to highlight its importance for possible present and future developments in the health professions. It is assumed that although these professions are “sciences in the making” [2] they at the same time have an extensive and invaluable “history of practice”.
On the Academisation of Medicine
It is only since the mid-19th century that the medical profession has been a relatively homogeneous group of academically trained experts. Huerkamp writes that the medical profession was segmented “into various subgroups, differing vastly with respect to their origin, educational background and training, their status and access to various client groups.” [3]. In a paper on the future of medicine [4] the Working Group on Medical Education of the Robert Bosch Foundation states that a relatively small group of academically trained doctors opposed the large group of surgeons, midwives, so-called lay healers and quacks. Similarly, the health professions that are now undergoing academisation may experience the same fate in a few years, opposing the large group of health care professionals who trained outside of academia.
The “Medical Profession Standards for Prussia" were regulated by law [5] in 1852. These formed the base for academic training standards up to this day. The standardization of academic training facilitated a tremendous surge in medical development, dominated by the natural sciences.
Naunyn (1839-1925), a specialist for internal medicine [6] described this historical development (Naunyn 1900): “What has elevated the art of healing is its growth into a self-conscious community of disciplines [such as pathological anatomy, bacteriology, hygiene physiology; author’s note], which are - without exception - natural sciences or at least based on natural science, a process which took place before 1870...” (ibid p. 21). The Prussian State hugely invested in the development of these medical disciplines in this period. However, Naunyn who was also a clinical physician and thinker, concludes “It is not correct to say that the 19th century is the period that fostered medicine to develop into a science... Medicine is also committed to humanity." (ibid p. 1)
Some 30 years after the creation of the standards for the medical profession, the introduction of a statutory health insurance in 1883 under the chancellorship of Bismarck was a further important step in improving the health care for the population. Although initially a statutory health insurance was only compulsory for the population groups with the lowest income [5], it was later extended considerably. Today, according to the Federal Agency for Political Education, 85.4% of the population have a statutory health insurance. These changes to the socio-legal framework have significantly supported the development of standards within the medical profession and have significantly improved the general public’s health, coupled with a steadily rising average life expectancy. The German Medical Journal (Deutsches Ärzteblatt) as an organ of the medical profession is already in its 107th year of publication.
The current trend to academize the health professions is intimately connected with the scientific achievements and the associated large social significance of academic medicine. This is not intended to slight other fields such as psychology, psychotherapy or linguistics. However, the success and the pivotal role of medicine and its physicians in the healthcare system in addition to the demographic development of the population and the conspicuous shift in the age structure are key to the urgently required academisation of the health professions. Medical diagnostics and treatment options have improved dramatically. Boundless innovations and information are available every day. This progress has created many opportunities for new perspectives and the need for necessary interventions. Weiler states [7] that “teaching of analytical, critical and normative skills to evaluate vast amounts of information that are largely disordered and nonvaluated” (p. 48) must be a central aspect of academic education. Examples of such information are the research and the publications on co-morbidity and chronic diseases in a population that is growing older and older. These complex diseases require a regular review of treatment and rehabilitation strategies [8]. The increasing need for the skills of other health professions in addition to medical knowledge and skills is obvious. Independent professional practice should no longer differentiate between medical treatments and so-called supportive medical treatments. In future, the health professions will need to base their complex treatment and therapy practice on strong research, thus generating independent, in-depth knowledge and skills that can be linked with academic medicine and other related disciplines such as linguistics, psychology and sport science.
Academisation of the Health Professions to Date
Since 1973 when the Science Council called for three-year diploma courses for physicians (technical, laboratory, care), there have been efforts to advance the academisationof the health professions in Germany. In a paper by the Robert Bosch Foundation, the need to further the academisation of care is described more extensively and in greater detail [9]. The paper argues for academic training in general care and a need to evolve the professional concept of a “supportive health profession to a health care profession” (p. 19-21). Already then detailed concepts for academic graduate courses (p. 129-146) were presented, albeit with an emphasis on management and pedagogy in care. Over the past few years, the initially reluctant then fast-paced development has seen more than 50 graduate courses grow in the care sciences with core areas in nursing science, nursing education and management. A closer look at the academisation of care shows how difficult this process is. Each health profession has its own vocational laws and provisions that determine the structure and curriculum of its relevant academic training program. Regarding “care”, the student training contract reveals the two strands of the undergraduate course: it is both a traditional vocational training and a graduate course which needs to adapt to the job training. The fundamental paradigm shift from vocational training to undergraduate studies is yet to come.
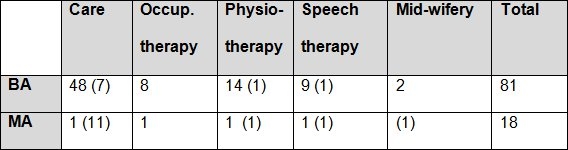
For occupational therapy, physiotherapy and speech therapy, the picture changes. It was only towards the end of 1990s that the first graduate courses for these professions were founded. Today, there are approximately 30 BA programs for therapists that already have a vocational training qualification. In Germany, these programs are usually taught at Universities of Applied Sciences in cooperation with vocational colleges and are mainly add-on or integrated training concepts. For midwives, there are two bachelor programs and a master’s degree program so far (see Table 1 (Tab. 1)).
Table 1. Number of graduate courses at universities and universities of applied sciences. The numbers in parentheses indicate university courses [1].
In 2003, a model clause was introduced into the vocational licensing regulations for nursing/care. The primary task of this early model clause was to obtain insights for new training models in the nursing profession. The clause also opened up the possibility for implementing model projects at universities. In September 2009, the new model clauses were brought into the vocational licensing regulations of occupational therapy, midwifery, physiotherapy and speech therapy. Similar to the former model clause, these new regulations allow for certain changes to the existing training and examination regulations. These minor changes only refer to the teaching part of the training, not to the practical part. Linking the vocational licensing regulations which in part are 20-30 years old to the academic curriculum of the graduate program will inevitably lead to mismatches as the goals and methods of a vocational training will, for very good reasons, not be the same as for those of an academic program. The vocational concepts for example assume that the teaching of theory and practice is almost entirely face to face. An academic program, however, requires that two-thirds of the course structure allow the student to learn autonomously, thus promoting the intellectual independence of aspiring academics. In addition, in contrast to claims of the Bologna process, it is difficult or impossible for students to spend parts of their studies abroad as the vocational licensing regulations demand that the German state authorities closely monitor training locations. This by itself is very difficult to implement in practice. In order to evaluate model projects the state of North Rhine-Westphalia founded the University for Applied Health Sciences in November 2009 as a university of applied sciences under the auspices of the Government of North Rhine-Westphalia in Bochum. It has been offering such model graduate courses since the winter semester 2010/2011.
Academisation - Attempting a Description
The academisation of health professions has been safeguarded with the adoption of the model clauses (for the time being). In 2015, there will be a first evaluation of the success of these courses following the guidelines of the Federal Ministry of Health [1]. At this point in time it cannot be said whether the academisation will succeed or not. This makes it all the more important to reflect upon the desired standard.
Academisation is a complex process. Its current state and development can only be described in small portions. One aspect concerns the scientific shift of the professions undergoing academisation and their need to legitimise this development in view of conventional vocational training. This process also addresses the question about the added value of higher education, i.e. training at a university.
The central goal of the academisation of health professions is to improve the quality of professional practice and thus to improve the provision of healthcare to the public. Equally important is the promotion of young scientists. The classic, more formal elements of an academic education also apply to the new model programs in health professions, such as ties to a university, special admission requirements, qualified teaching staff, research-based teaching, independent learning phases and academic degrees.
The University of Applied Health Sciences aims to train its graduates for direct patient contact and not primarily for tasks in health management or as tutors in vocational colleges. They will therefore be faced with tasks, just as their non-academically trained colleagues, connected to direct contact with the patient in their professional practice. This may require both general and specialist skills. However, it can be expected that the skills acquired in an academic education and the resulting stronger reflexive attitude will enable the graduates to work with a higher degree of professionalism compared to professionals with a purely vocational training background. The aim of a university degree is to enable the graduate to independently apply and produce scientific insights and to have the ability to critically reflect their work methods [10]. This constitutes a substantial part of the added value which distinguishes a university graduate from a graduate in classical vocational training. University teaches students to better cope with the imponderable, the uncertainty and competing interpretations of complex issues. Scientific discrimination is a prerequisite for the ability to analyse and evaluate complex issues and to question professional thinking and practice in professional life marked by routine. These are skills which the future professional will need to deal with complex situations in practice.
Generally, academic disciplines achieve these tasks by relying on years of academic and professional experience. The health professions lack this type of long experience. In Germany, they stand at the beginning of the process of academisation, although aspects of this process are at very different stages of development. The academisation of care, for example, due to its temporal advantage, is at a very different stage than the academisation of midwifery which has only been represented at German universities since 2008. These new disciplines can indeed look back on decades of practice but in terms of their academisation, they have to rely on other established sciences. Not one of the health professions has yet completely achieved their own scientific identity as an academic discipline. The “new” health disciplines are “sciences in the making” [2]. Their key reference sciences, the medical sciences aside, include psychology, linguistics, sociology and pedagogy. The process of developing an identity which is associated with academisation is complex and difficult and appears contradictory. This may lead to considerable confusion and controversy amongst its key stakeholders, as is well known from other academic disciplines. There is no silver bullet in the academisation process. Differences and diversity can enrich disputes in academic encounters. An academic “culture” that allows these differences and diversity will appear lively and exemplary. This culture can certainly be found between the academized health professionals and the medical profession. Furthermore, this culture fosters an academic stance at university that is characterised by critical, interdisciplinary and innovative thinking and work, professional curiosity and respect.
The members of the teaching staff should be experts in their own disciplines. For that reason legal topics, for example, are taught by lawyers, psychological topics by psychologists and medical topics by physicians. Research-based teaching requires extensive knowledge of the relevant disciplines (reference sciences). At the same time, the reference scientists (such as physicians, psychologists) need to have sufficient knowledge of the working and thinking processes that are specific to the disciplines undergoing academisation. This can be achieved if the academic staff of all these disciplines engage in an intensive exchange of ideas. This cooperation will also fertilize the process of academisation with theoretical and methodological impulses. The practice-oriented clinical focus of the undergraduate studies requires the integration of references sciences, thus providing excellent opportunities for shaping and promoting the academisation process. Particularly during the practice-oriented phases, it is vital to open the space to diverse theoretical and didactical influences as these will foster a variety of experiences and strengthen the academic identity.
Due to the practice-oriented clinical focus during the studies, a special emphasis is placed on case-oriented learning. By reflecting their practical experiences, students contribute to the scientific development of their disciplines. It is desirable that practice-oriented seminars and exercises are taught with an interdisciplinary approach. This allows students (and tutors) of different disciplines to learn together and practice how they collaborate as professionals in the future. Furthermore, case-oriented learning enables students to develop a reflected understanding of professional practice and a growing awareness of their specific professional identity. Students thus experience that ‘their’ discipline is closely connected with others: Inspite of their own specialist knowledge and skills, they all depend on reference sciences.
The academisation process is made up of training and broad-based research activities. With the exception of care, the health disciplines are still at the very beginning of a research base. Adler & von dem Knesebeck [8] stress that generating evidence-based research is essential if academisation is to succeed. Pure research can help to develop theoretical models and concepts that can be transferred to the vocational fields. These could then be tested empirically, thus forming the transition to patient-oriented research, which in turn verifies the effectiveness of policies.
At the same time is also conceivable that clinical research will generate new theoretical models, which in turn will serve to improve clinical practice [11]. The Epistemology of Practice as developed by Schön [12] counters a practice which is characterised by “complexity, uncertainty, instability, uniqueness and value-conflict" (p. 39) and which cannot be captured or represented by technical rationality. At the heart of Schön’s epistemology lies the practice concept of ‘reflection-in-action’ (p. 49) where practitioners are viewed as reflective practitioners. By reflecting their own practice they become researchers and generate theories of practice which are constantly evolving, without turning into static theoretical knowledge which is meaningless for practice. Reflection-in-action as a research concept is suited for ensuring practice-oriented degree courses and constitutes the attempt to deal (in innovative ways) with the major uncertainties and inconsistencies of practice, with its unusual and unexpected scenarios, to explore ways which may lead to (innovative) possibilities for practice. In essence, this research concept is a progressive spiral of different levels of perceptions: Actions and reviews of these actions are continuously processed, analyzed and evaluated, as for example in Schaub’s evaluation of a practical research project on the treatment of chronically ill patients in primary care [11].
The academisation of graduates leads to numerous job opportunities which also contribute to changes in the labour market. These changes follow from the fact that professional groups will be made up of various job qualifications and career paths in need of coordination, as the Council of Experts [13] stated in 2007 (p. 26). This causes anxiety amongst various professional associations, trade unions and groups within the medical profession. Only gradually a discussion has begun on which labour market graduates will be competing in, and what tariff structures in which practice fields will be open to them. The issue of the academisation of health professions is closely associated with this discussion but it is not strictly speaking an issue of the academisation of health professions but rather an issue of their professionalisation. The aspect of academisation cannot be equated with the overall phenomenon of professionalisation. In an overview, Kurtz [6] describes how characteristics of professionalisation have affected many areas of society. Moreover, the sociology of professionalisation stresses that professionalisation is to be understood as an ongoing change process amongst vocational groups on the basis of changing societal conditions [14].
Academisation of the Health Professions – Outlook
It is too early to give a first critical review of the possible impacts of the effects of academisation. Nevertheless, chances and development opportunities which result from this process can be identified. With the current wave of academisation, Germany is trying to catch up with standards long achieved in Europe and the US. The introduction of model clauses can only be seen as a first step on this journey [15]. Particularly in the UK, some Scandinavian countries, the Netherlands and the USA academisation is already well advanced, including the creation of appropriate positions in the labour market. It is therefore understandable that many enthusiastic and highly qualified graduates from vocational colleges and high schools in Germany leave to study abroad and eventually work in appropriate posts. It is necessary to offer attractive degree models in Germany in cooperation with universities so that not only German students remain in the country but foreign students are attracted to coming to Germany, too.
In future, the working relationship between academic medicine, other disciplines such as psychology, sociology, linguistics or rehabilitation sciences and the health professions undergoing academisation will play a central role. This new form of cooperation will most likely succeed if attempts are made to identify common interests. Two fields shall serve as examples and will be described in more detail. They constitute part-joint degree courses and clinical research projects.
Under the heading “Interprofessional Education (IPE)”, the World Health Organization (WHO) states [16]: “Interprofessional education occurs, when students from two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes” (p.7). The WHO goes on to state that IPE is a necessary prerequisite for identifying local needs as students learn to think inter-professionally and become competent in working in interdisciplinary teams. This can be practiced in joint case-oriented learning phases. By doing this, the various professional roles can practice working collaboratively with patients [17]. It can be assumed that the quality of diagnosing and treating patients will be significantly improved if the involved professional groups are able to communicate openly and freely on the basis of mutual respect. For this reason, the joint learning and practice of professional interactions adds a quality to degree courses that cannot be valued too highly and is therefore essential for future programs. Recently Hahn [18] proposed to create a Society for Education in Health Professions which can become a partner of the existing Society for Medical Education. In the long term, both societies could merge. This would promote inter-professionalism but also elevate educational research for a future healthcare system to an internationally competitive level.
The second field concerns clinical research. Countless research topics lend themselves to be researched upon, especially if the interfaces between the various disciplines are considered. For example, research could be done on medical obstetrics and midwifery or on the treatment and rehabilitation of stroke patients as carried out by medicine, nursing, occupational therapy, physiotherapy and speech therapy. An overview of worldwide research in the area of interdisciplinary research is offered by the Human Resources for Health Framework for Action on Interprofessional Education & Collaborative Practice [16]. It can be very helpful for all involved parties to draw on decades of research and practice experience within medicine and other related disciplines as well as on the various research experiences and the seemingly endless amount of practical experience of the health professions.
It is not yet possible to determine in detail what the consequences of cooperation will have on tomorrow’s healthcare. But experience has already shown that, in particular in the field of co-and multi-morbidity and chronic diseases, successful cooperation can reduce suffering because professionals that coordinate different perspectives at high quality level increase the chances of healing processes. The academisation of health professions represents a useful building block in this framework and is not an end in itself. It solely serves to improve healthcare and to use knowledge and responsibility for the support of people.
Competing interests
The authors declare that they have no competing interests.
References
- 1.Bundesministerium für Gesundheit. Bekanntmachung von Richtlinien über die wissenschaftliche Begleitung und Auswertung von Modellvorhaben nach § 4 Absatz 6 Satz 3 des Ergotherapeutengesetzes, § 6 Absatz 4 Satz 3 des Hebammengesetzes, § 4 Absatz 6 Satz 3 des Logopädengesetzes und § 9 Absatz 3 Satz 3 des Masseur- und Physiotherapeutengesetzes vom 16. November. Bundesanzeiger. 2009;180:4052. [Google Scholar]
- 2.Friedrichs A, Schaub HA. Interprofessionalität – aktuelle Rahmenbedingungen und Anforderungen an das Studium. Ausbildung für die Gesundheitsversorgung von morgen. Stuttgart: Schattauer Verlag; 2011. pp. 98–101. [Google Scholar]
- 3.Heilmeyer L. Lehrbuch der Inneren Medizin. 2. Auflage. Göttingen, Heidelberg: Springer; 1961. p. 3. [Google Scholar]
- 4.Robert Bosch Stiftung. Arztbild der Zukunft: Analysen künftiger Anforderungen an den Arzt; Konsequenzen für die Ausbildung und Wegweisung zu ihrer Reform. Gerlingen: Arbeitskreis Medizinerausbildung d. Robert Bosch Stiftung; 1989. p. 22. [Google Scholar]
- 5.Deutsches Reichstag und Bundesrath. Reichsgesetz. Reichsgesetz-Blatt. 1883;9:15. [Google Scholar]
- 6.Kurtz T. Berufssoziologie. Bielefeld: Transcript; 2002. [Google Scholar]
- 7.Weiler H. Bildung zwischen Ökonomie und Technologie – Homo Sapiens im Wettbewerb. Die berufsbildende Schule. 2010;62:45–50. [Google Scholar]
- 8.Adler G, von dem Knesebeck JH. Auf akademischen Wegen. Dtsch Arztebl. 2010;107(9):A386–A390. [Google Scholar]
- 9.Robert Bosch Stiftung. Pflege braucht Eliten. Gerlingen: Bleicher Verlag; 1992. [Google Scholar]
- 10.Bollinger H, Gerlach A, Pfadenhauer M. Gesundheitsberufe im Wandel – Soziologische Beobachtungen und Interpretationen. Frankfurt a.M.: Mabuse; 2005. [Google Scholar]
- 11.Schaub HA. Klinische Sozialarbeit. Göttingen: Vandenhoeck & Ruprecht unipress; 2008. [Google Scholar]
- 12.Schön DA. The Reflective Practitioner. How Professionals think in Action. New York: Basic Books; 1983. [Google Scholar]
- 13.Sachverständigenrat zur Begutachtung der Entwicklung im Gesundheitswesen. Kooperation und Verantwortung. Bonn: Nomos-Verlag; 2007. [Google Scholar]
- 14.Walkenhorst U. Potenziale der Ergotherapie in der Gesundheits- und Krankenversorgung – Eine handlungsorientierte professionssoziologische Analyse. Idstein: Verlag Schulz-Kirchner; 2008. [Google Scholar]
- 15.Wasner M. Qualitätsmanagement in der Ausbildung Physiotherapie in den EU-Ländern. Heidelberg: Fak. f Verhaltens- und empirische Kulturwissenschaften der Ruprecht-Karls-Universität; 2007. [Google Scholar]
- 16.World Health Organization. Health Professions Networks Nursing & Midwifery. London: CAIPE; 2010. Available from: http://www.caipe.org.uk. [Google Scholar]
- 17.Dahlgaard K. Verbesserung der teamorientierten Zusammenarbeit zwischen Ärzten und Pflegenden – Neue Chancen durch Prozessorientierung und erweiterte Aufgaben für Pflegende. Z Evid Fortbild Qual Gesundhwesen (ZEFQ) 2010;104:32–38. doi: 10.1016/j.zefq.2009.12.004. Available from: http://dx.doi.org/10.1016/j.zefq.2009.12.004. [DOI] [PubMed] [Google Scholar]
- 18.Hahn EG. Anmerkungen aus der Medizin. Dokumentation der 3. Werkstatt-Tagung „Zukunft der Hochschulbildung für Gesundheitsberufe im europäischen Kontext“ vom 24. und 25.06.2010 in Bochum. Magdeburg: Hochschulen für Gesundheit e. V.; 2010. pp. 31–32. [Google Scholar]
- 19.Billig M. Gesundheitsfachberufe. Drang zu akademischer Ausbildung. Dtsch Arztebl. 2011;108(1-2):A–30. [Google Scholar]
- 20.Huerkamp C. Aufstieg der Ärzte im 19. Jahrhundert. Vom Gelehrtenstand zum professionellen Experten: Das Beispiel Preußens. Kritische Studien zur Geschichtswissenschaft. Göttingen: Vandenhoeck & Ruprecht; 1985. pp. 68–122. [Google Scholar]