

Abstract
A family of five and pet dog who rented a water-damaged home and developed multiple health problems. The home was analyzed for species of mold and bacteria. The diagnostics included MRI for chronic sinusitis with ENT and sinus surgery, and neurological testing for neurocognitive deficits. Bulk samples from the home, tissue from the sinuses, urine, nasal secretions, placenta, umbilical cord, and breast milk were tested for the presence of trichothecenes, aflatoxins, and Ochratoxin A. The family had the following diagnosed conditions: chronic sinusitis, neurological deficits, coughing with wheeze, nose bleeds, and fatigue among other symptoms. An infant was born with a total body flare, developed multiple Cafe-au-Lait pigmented skin spots and diagnoses with NF1 at age 2. The mycotoxins were detected in bulk samples, urine and nasal secretions, breast milk, placenta, and umbilical cord. Pseudomonas aueroginosa, Acinetobacter, Penicillium, and Aspergillus fumigatus were cultured from nasal secretions (father and daughter). RT-PCR revealed A. fumigatus DNA in sinus tissues of the daughter. The dog had 72 skin lesions (sebaceous glands and lipomas) from which trichothecenes and ochratoxin A. were detected. The health of the family is discussed in relation to the most recent published literature regarding microbial contamination and toxic by-products present in water-damaged buildings.
1. Introduction
Indoor dampness and fungal contamination have been shown in qualitative reviews to be associated with a variety of respiratory health effects, including infections, sinusitis, and otitis media [1–4]. In addition, case studies with and without controls have demonstrated the existence of severe sinusitis as well as neurological deficits in occupants in water-damaged homes and buildings [5–12]. Currently, it is recognized that the indoor water-damaged environment resulting from microbial growth is a complex mixture of mold and bacteria along with their by-products [13–15]. Thus, the illnesses resulting from exposure cannot be defined by any specific component of the affected environment [2, 13–17]. In this paper we present a family of five exposed to fungi and bacteria in a water-damaged home located in Maui, Hawaii. Members of the family developed multiple health problems, including sinusitis and neurological deficits. In addition, the mother was pregnant during occupation of the contaminated home giving birth to a girl who had a total body flare with development of Cafe-au-Lait spots. Her condition has been diagnosed with Neurofibromastosis type (NF1).
2. The Family
The family of five moved from Canada to Maui, Hawaii, in February 2008, where they rented a home. All were healthy prior to the move and began experiencing symptoms shortly after the move in. Chief health complaints were as follows. Father (age 40) had persistent cough with phlegm, throat irritation, headaches, sinusitis, severe fatigue, somnolence, decreased concentration, long-term and recent memory loss, nose bleeds, decreased libido, hair loss, and shortness of breath with wheezing. The mother (age 39) complained of cough with phlegm, throat irritation, headaches, sinusitis, extreme fatigue, somnolence, recent and long-term memory loss, decreased libido, and shortness of breath with wheezing. She became pregnant while living in the home and gave birth to a girl 3 months after moving out of the home. The eldest daughter (age 8) had the same symptoms as the parents, except she had decreased concentration, nausea, and loss of appetite. The son (age 5) had frequent headaches, fatigue and tiredness, nasal congestion, nose bleeds, throat irritation, shortness of breath with mild wheezing, and decreased attention in classroom activities. The newborn had a total body flare (pinkish red) that continued to age 10–12 weeks, after which the flare would appear periodically. She had multiple pigmented skin spots on her back, chest, and abdomen at birth that appeared to be Cafe-au-Lait spots. The pigmented areas are still present at 2 years of that are scheduled for additional diagnostics for neurofibromatosis (Figure 1). Finally, the pet dog developed approximately 72 skin lesions diagnosed as sebaceous and lipoma tumors (Figure 2).
Figure 1.
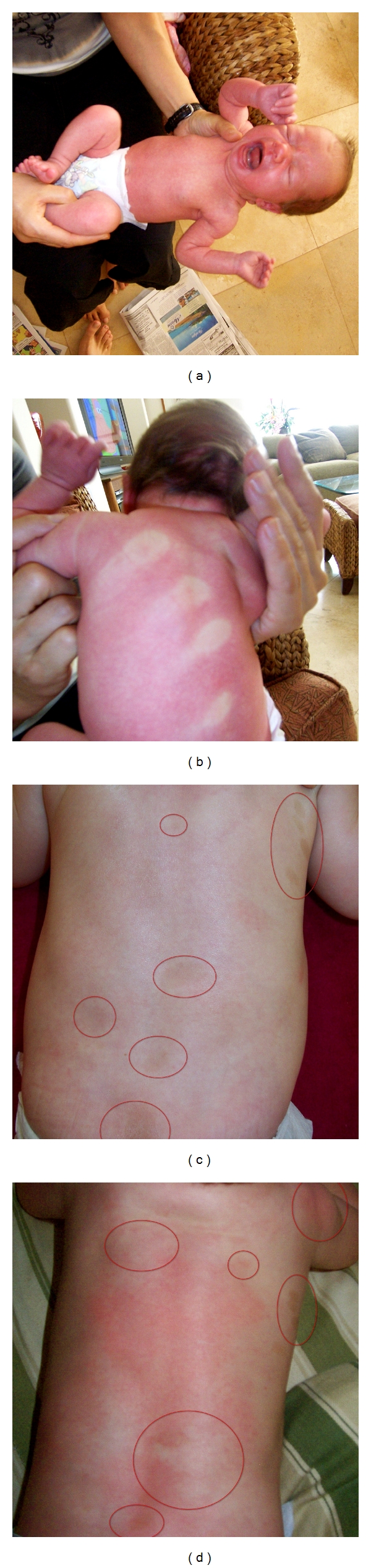
The upper two photos are of the newborn girl demonstrating the total body flare and the impression of the Father's hand on her back. The bottom two photos show the pigmented sports that appear to be Cafe-au-Lait skin pigmentation that were apparent at birth and are still present. The flare reaction was present at birth, began to subside at 10–12 weeks, and occurred periodically through 55 weeks of age. The multiple pigmented spots has been diagnosed as NF1 at U.S. San Francisco, Department of Dermatology.
Figure 2.

This figure demonstrates the sites of the subcutaneous and lipoma tumors that were removed from the pet dog. The Veterinarian stated that the presence of 72 such lesions on an animal is a very rare observation.
3. Neurological Evaluation
The family sought neurological consultation from one of the authors as previously published [8, 9]. The results of the evaluations are briefly summarized as follows.
The father had 17 neurological deficits as follows: simple and choice reaction time, sway-balance with eyes open and closed, decreased right and left grip strength, abnormal right and left color vision, abnormal visual field performance (right and left), abnormal digit symbol, abnormal perceptual motor speed (dominant pegboard, Trails A and B, right and left finger writing errors), abnormal smell score, abnormal picture completion and elevated Profile of Mood States (POMS), Beck's depression inventory, and Limbic System Check List score. The increased POMS score was consistent with elevated confusion, fatigue, and tension. The mother also had 17 abnormalities, identical to those of the husband (data not repeated). The neurological scores for the daughter were within normal ranges. However, the physical exam revealed abnormal past pointing without dysmetria (finger to nose) and fine resting tremors at 3-4 per second increasing to 10 by intention with amplitude increased. The son (age 5) did not have any detectable neurological deficits. However, the neurological testing is not designed for 5 year olds.
In conclusion, the neurological evaluation revealed multiple deficits in both parents as previously published [8, 9]. The daughter had noticeable tremors which may have resulted from exposure to tremorgenic mycotoxins [18–22] as well as others described here in after (see Section 9 and Tables 4 and 5).
Table 4.
This table summarizes the detection of trichothecenes, aflatoxins and ochratoxin A present in bulk samples taken from the master bath, master bedroom (sandal), and crawl space. The reported data are in ppb per mycotoxin.
| Sample | Trichothecenes | Aflatoxins | Ochratoxin A |
|---|---|---|---|
| Towel—master bath | 11.71 | NP | 4.9 |
| Sandal—master bdrm | 0.47 | NP | 3.4 |
| Wood truss—crawl space | 1.68 | 3.5 | 5.8 |
| Gravel—crawl space | 7.7 | NP | 7.7 |
| Dirt—crawl space | 2.1 | NP | 2.1 |
| Plastic sheet—crawl space | NP | NP | 2.8 |
Reported data are ppb.
NP: Not present.
Limit of Detection: Trichothecenes (0.2 ppb); Aflatoxins (1.0 ppb); Ochratoxin A (2.0 ppb).
Table 5.
Mycotoxins present in body fluid of the five members of the family and the pet dog.
| Patient specimen | Trichothecenes (ppb) | Aflatoxins (ppb) | Ochratoxin (ppb) |
|---|---|---|---|
| Father-Urine | NP | NP | 18.2 |
| Father-Nasal1 Secretion | NP | 0.5 11.2 |
13 7.7 |
| Mother-Urine | NP | NP | 18.2 |
| Mother-Nasal Secretion | 1.02 | 1.2 | 1.6 |
| Daughter-Urine | 0.23 | NP | 28.0 |
| Daughter-Nasal2 Secretion | 4.68 | NP | 3.8 |
| Son-Urine | 0.2 | NP | 18.9 |
| Son-Nasal Secretion | ND | ND | ND |
| Breast Milk | 0.18 | 0.9 | 2.7 |
| Placenta | NP | NP | 4.2 |
| Umbilical Cord | NP | NP | 7 |
| New Born-Urine | NP | NP | NP |
| Dog-Urine | 1.49 | NP | 25.9 |
| Dog-Ear Mass | 23.07 | 0 | 2.2 |
| Dog-Lipoma | 20.9 | 0 | 1.4 |
Limits of Detection: Trichothecenes (0.2 ppb); Aflatoxins (1.0 ppb); Ochratoxin A (2.0 ppb).
ND: Not done.
NP: Not present.
1 Pseudomonas aueroginosa and Penicillium were cultured from the nasal secretions. These data represent two different tests.
2 Acinetobacter sp. was cultured from nasal secretion at too numerous to count. In addition, Aspergillus fumigatus was cultured from left ethmoid and sphenoid mucosal surgical specimen.
4. MRI
MRIs were performed at Oak Tree Medical Imaging, Pasadena, California, for each family member with special reference to the sinuses.
Father —
The father had mild diffuse thickening- bi-ethmoid, bi-maxillary, right sphenoid and frontal sinuses.
Mother —
The cavernous and paranasal sinuses were normal. Prior to the MRI, she had been prescribed corticosteroids, antibiotics, and antifungals.
Daughter —
The daughter had mild fluid within the bilateral mastoid air cells. There is moderate to severe mucosal thickening in the maxillary and ethmoid sinuses without evidence of air fluid level.
Son —
The bifrontal and sphenoid sinuses have not developed. Maxillary sinuses are unremarkable. There is slight mucosal thickening within the bilateral sphenoid sinuses, right greater than left without air fluid level.
In conclusion, the results of the MRI studies demonstrated mucosal thickening of the sinuses of the father and two children. The absence of findings in the mother most likely resulted from the use of corticosteroids and medications to treat her sinusitis.
5. ENT Evaluation
The father and daughter were evaluated at the Atlanta Center for ENT & Facial Plastic surgery according to procedures previously published [5, 6]. The results of the evaluation are briefly summarized as follows.
Father —
Nasal endoscopy revealed (a) nasal polyps and (b) the ethmoid, sphenoid, and frontal sinuses were edematous with visible thick mucoid material (mucin) bilaterally, confirming the results of earlier MRI and CT scans (data not described). Total IgE was 76.9 IU/mL with a positive IgE score at level IV for Alternaria. He was tested for IgG antibodies for ten fungi and was positive for Epiccocum and Cladosporium at level I, Penicillium, Aspergillus, Alternaria, Fusarium, and Acremonium at level III, and Candida at level III. Recommended treatment was saline nasal wash, intranasal amphotericin B, oral fluconazole, Nystatin, intranasal glutathione, and oxygen via a face mask. Surgery was performed to remove nasal polyps and inflamed sinus tissues. Tissue samples were sent to RealTime Laboratories, Carrollton, Texas, for RT-PCR DNA probes (10 species of fungi), and mycotoxin testing.
The RT-PCR-DNA probes were negative for the following fungi: Aspergillus flavus, fumigatus, niger, and versicolor; Eurotium amstelodami; Fusarium solani; Penicillium chrysogenum and verrucosum; and Stachybotrys chartarum and echinata. Cultures for bacteria (SBA) and fungi (MEA) in nasal secretions were positive for Pseudomonas aeuroginosa and Penicillium spp.
Daughter —
Endoscopic examination revealed that left maxillary, ethmoid, sphenoid, and frontal recesses were edematous. The turbinates were 4+ enlarged. The nasal septum was deviated to the left. On the right side there was some white material on the middle turbinate. The adenoids were hypertrophied. In addition, small white flecks were present in the soft tissue of the left maxillary, ethmoid, and left sphenoid sinuses. Medications include fluconazole, liposomal glutathione, amphotericin B, inhaled corticosteroid, Nystatin, and oxygen via face mask. The patient required left sphenoidotomy. Also, the previous MRI and CT scans showed opacification of the left infundibulum and left maxillary sinus os. Surgical specimens were sent to RealTime Laboratories tor RT-PCR DNA probe (10 species of fungi) and mycotoxin detection.
The RT-PCR tests were negative for the same species as done on the father (see above). However, cultures for bacteria (SBA) and molds (MEA) on nasal secretions revealed Acinetobacter spp. and Aspergillus fumigatus.
In conclusion, the nasal endoscopic examinations of the father and daughter revealed edematous inflammation of the paranasal sinuses that required surgery. The RT-PCR tests were negative for 10 species of fungi, which did not eliminate the presence of fungi other than those tested. Finally, bacterial and fungal cultures of nasal mucous secretions did reveal the presence of bacteria (Pseudomonas and Acinetobacter) as well as fungi (Penicillium and Aspergillus). Thus both patients had severe chronic rhinosinusitis most likely related to microbes (bacteria and fungi) detected in their water-damaged home [1–3, 5, 6, 23–25].
6. The Home
The home was inspected for construction defects and dampness by two independent services: Barkman Inspection Services [26] and Engineering Dynamics Corp [27]. The results of the two inspections are briefly summarized.
6.1. Barkman Report
A serious moisture/mold problem is observed in the crawlspace directly below the bedrooms. Moisture is penetrating the walls of the foundation. The HVAC system is designed to force air into the crawl space, forcing crawl space air into the bedrooms and other areas above. Moisture intrusion also results from the master shower into the crawl space as well as from sprinklers, damp soil against the foundation, lack of roof gutters, and poor grading.
6.2. Engineering Dynamics Report
This is a two-story house with a crawl space. Lower level has a family room, guest bedroom, bathroom, powder room, arts and crafts room, storage closet, garage, and crawl space, which are under upper level bedrooms and bathrooms. Upper level has 3 bedrooms, 3 bathrooms, entertainment room, living room, kitchen, office, and powder room.
The crawl space had water intrusion, musty mold odor, and visible mold on floor joists. The yard sprinklers were directed towards the house and the eaves did not have rain gutters, permitting the pooling of water. Water entered the crawl space through cement walls and followed piping present in the crawl space. Smoke testing revealed communication between the crawl space and upper level bedrooms via electrical outlets and electrical ducts and plumbing. The conduit holes were not sealed, permitting observance of light coming through spaces in the floor joists. A musty odor was present in the master bathroom and noted to get stronger when the fan coil was turned on.
7. Identification of Mold
All air and bulk samples were sent under chain of custody to EMSL Analytical, Inc., Westmont, NJ. The ERMI Q-PCR 36 for mold species was performed on 5 different bulk samples. The data are summarized in Table 1. The identified species of mold varied according to source but included species of Aspergillus, Penicillium, Eurotium amstelodami, A pullulans, C. globosum, and T. viride, among others. The ERMI interpretation level ranged from 2 to 3, indicating moderate contamination.
Table 1.
This table summarizes the results of the E.P.A. ERMI PCR-DNA tests performed on 5 mg dust samples from basement and master bedroom carpeting and master bedroom wall insulation. Only the species detected are listed.
| Sample 36 ERMI Q-PCR test | Carpet basement | Carpet, master Bdrm | Insulation master Bdrm1 | Insulation return air duct | Moist fiberglass |
|---|---|---|---|---|---|
| Group 1 Molds | |||||
| Asp. penicillioides | 77 | 26 | ND | ND | |
| A. restrictus | ND | ND | ND | 40 | 40 |
| A. versicolor | ND | ND | ND | ND | 50 |
| E. amstelodami | ND | ND | ND | 4 | 4 |
| Aur. pullulans | 189 | 20 | ND | ND | ND |
| Ch. globosum | ND | 14 | ND | ND | 2 |
| Cl. Sphaerospermum | 9 | 3 | ND | ND | ND |
| Pae. variotii | ND | 2 | 87 | ND | 734 |
| P. brevicompactum | ND | 19 | ND | ND | ND |
| P. corylophilum | ND | ND | ND | ND | 85 |
| P. crustosum | ND | ND | 3 | ND | ND |
| P. purpurogenum | ND | 2 | ND | ND | ND |
| P. spinulosum | 15 | ND | 3 | ND | ND |
| P. variabile | ND | ND | ND | 136 | 3 |
| T. viride | ND | ND | NS | ND | 15 |
| Sum of the Logs | 6.6 | 6.2 | 2.8 | 2.8 | 10.6 |
|
| |||||
| Group 2 Molds | |||||
| A. ustus | 2 | 4 | 187 | ND | 226 |
| Cl. cladosporioides II | 1 | ND | ND | 65 | 2 |
| Ep. nigrum | 15 | 17 | ND | 65 | 8 |
| Ep. nigrum | 15 | 17 | ND | 14 | 5 |
| Mucor/Rhizopus | 9 | 21 | ND | ND | ND |
| P. chrysogenum | 5 | 4 | 8.738 | ND | 14.013 |
| Sum of the logs | 3.3 | 3.7 | 6.2 | 3.0 | 8.1 |
|
| |||||
| ERMI Value | 3 | 2 | −3 | 0 | 3 |
|
| |||||
| ERMI Interpretation | Level 3 | Level 3 | Level 2 | Level 2 | Level 3 |
ND: Not detected.
1RT-PCR detected Aspergillus fumigatus in a towel taken from the master bathroom.
All values are in Spores E.−/mg dust.
Airborne viable spores were determined by Air-O-Cell cassettes and cultured and identified by EMSL Method M050 and the data are summarized in Table 2. The viable airborne spores (Table 2) showed the presence of toxic fungi inside of the home and none outdoors. The viable spores included species of Aspergillus and Penicillium, which varied according to the sample area, for example, crawl space versus bedroom air and wall space cavity.
Table 2.
This table summarizes the identification and enumeration of culturable air-borne fungi collected by Aerotech cassettes (including speciation of Penicillium, Aspergillus, Cladosporium, and Stachybotrys) by EMSL Method M050.
| Sample location | Media | Temp (°C) | Sensitivity & dilution | Fungal identification | Colon count | CFU per cassette |
|---|---|---|---|---|---|---|
| Swimming pool deck | MEA | 25 | 100 & 100 | None detected | 0 | 0 |
|
| ||||||
| Master bedroom | MEA | 25 | 100 & 100 | Asp. sydowii | 1 | 100 |
| 100 & 100 | Cl. sphaerospermum | 1 | 100 | |||
| P. chrysogenum | 1 | 100 | ||||
| Total | 3 | 300 | ||||
|
| ||||||
| Crawl space | MEA | 25 | 100 & 100 | Asp. ochraceus | 5 | 500 |
| 100 & 100 | Asp. sydowii | 2 | 200 | |||
| 100 & 100 | P. chrysogenum | 1 | 100 | |||
| 1000 & 1000 | P. citreonigrum | 1 | 1000 | |||
| 1000 & 1000 | Phialophora sp. | 1 | 1000 | |||
| 1000 & 1000 | Sterile (dark) sp. | 1 | 1000 | |||
| Total | 11 | 3.800 | ||||
|
| ||||||
| Wall space master bedroom | MEA | 25 | 100 & 100 | Asp. fumigatus | 1 | 100 |
| 100 & 100 | Asp. ustus | 3 | 300 | |||
| 100 & 100 | Paecilomyces sp. | 2 | 200 | |||
| 1000 & 1000 | P. chrysogenum | 1 | 1000 | |||
| Total | 7 | 1.600 | ||||
In conclusion, these data demonstrated that testing for fungal contamination must include several different sample locations involving dust and bulk materials as well as airborne viable spores [28].
8. Identification of Bacteria and Endotoxins
Bulk samples of crawl space dirt, gravel, plastic sheeting, wood, and a sandal from under the master bed were sent to EMSL Analytical, Inc., Westmont, NJ and RealTime Laboratories, Carrolton, TX, to culture and identify bacteria using sheep blood agar (SBA) plates. In addition, two swab samples from the kitchen were analyzed for endotoxins by EMSL. The results are summarized in Table 3.
Table 3.
This table summarizes the bacteria and endotoxins identified in various bulk samples taken from the home (EMSL Method M009) and by RealTime Laboratories (RTL), Dallas, TX.
(a)
| Sample | Sample # | Media | Temp (°C) | Analytical sensitivity CFU/g | Bacteria | Colony count | CFU/g |
|---|---|---|---|---|---|---|---|
| Plastic sheeting, crawl space | #34 | SBA | 35 | 98.000 |
Bacillus sp
Streptomyces sp. Actinomycetes |
25 | 2.450.000 |
|
| |||||||
| Moist gravel, crawl space | #27 | SBA1 | 35 | 885 |
B. megaterium
Bacillus sp. Total |
10 7 17 |
8.850 6.190 15.000 |
|
| |||||||
| Moist dirt, crawl space | #28 | SBA1 | 35 | 8130 |
B. megaterium
Bacillus sp. Total |
4 6 10 |
32.500 48.800 81.300 |
|
| |||||||
| Swab of wood, crawl space | #25 | SBA2 | 35 | 10.000 |
Microbacterium hominis
Staphylococcus sp (not aureus) Total |
972 2 974 |
9.720.000 20.000 9.740.000 |
|
| |||||||
| Dirt crawl space | #28 | Blood Agar | 353 | — |
Bacillus sp.
Proteus sp Pseudomonas sp. |
TNC4 | TNC4 |
|
| |||||||
| Gravel, crawl space | #27 | Blood Agar | 353 | — |
Bacillus sp.
Proteus sp. Pseudomonas sp. |
TNC4 | TNC4 |
|
| |||||||
| Sandal, under master bed | #36 | Blood Agar | 353 | — |
Bacillus sp.
Proteus sp. Pseudomonas sp. |
TNC4 | TNC4 |
(b)
| Endotoxins | Sample # | Sample type | Location | Concentration (EU/Swab)5 |
|---|---|---|---|---|
| #3 | Swab | J-Tube, Under Sink | 4930 | |
| #4 | Swab | Top, Kitchen Cabinet | 24.800 | |
| Blank | Swab | Field Blank | None Detected | |
| Blank | Swab | Lab Blank | None Detected |
1These samples were tested to determine the major species of Bacillus.
2This sample was tested for Actinomycetes because of white mycelia type growth on wood truss.
3These samples were tested by RealTime Laboratories for the presence of bacteria species on samples tested for mycotoxins.
4CFU was not determined. TNTC: too numerous to count.
5Endotoxins were analyzed by ESML using LAL Kinetic Chromogenic Assay.
Bacteria detected by both laboratories included Gram negative and positive organisms. The primary Gram positive bacteria included Bacillus spp, Actinomycetes (e.g., Streptomyces sp., Mycobacterium hominis), and Staphylococcus (non aureus). The Gram negative bacteria were species of Pseudomonas and Proteus spp. Both groups of bacteria are potential human pathogens. For example, Mycobacterium and Streptomyces spp. are capable of causing lung abscesses and granulomatous mycetomas, while Pseudomonas species can cause respiratory and other infections [29–31].
Endotoxins were tested in only two areas of the home. The J-tube under the kitchen sink, a relatively protected area, had a concentration of 4.930 EU per swab. In contrast, the top of the kitchen cabinet had a concentration of 24.800 EU/swab. The two control swabs were negative. These observations indicate that additional testing was probably warranted, since endotoxins cause respiratory inflammation, sensitizers, and exacerbation of asthma [32–35]. In conclusion, bacterial cultures identified potentially pathogenic Gram negative and positive bacteria. In addition, these bacteria are known to produce toxic secondary metabolites of which Valinomycin is a mitochondrial toxin and is synergistic with macrocyclic trichothecenes [36–39]. Recently, several toxic bacterial metabolites have been demonstrated to cooccur with mycotoxins in moisture-damaged indoor environments [15].
9. Identification of Mycotoxins in Environmental Samples and Body Fluids
Bulk samples were sent to RealTime Laboratories, Carrollton, TX, to test for the presence of mycotoxins. In addition, urine and nasal mucous were collected in sterile cups, sealed and sent to RealTime Laboratories to test for the presence of mycotoxins. The tests for macrocyclic trichothecenes, aflatoxins, and ochratoxin A were performed as previously reported [40].
9.1. Environmental Samples
The data for mycotoxins detected in bulk samples are summarized in Table 4. Trichothecenes and ochratoxin A were detected in the bathroom towel (11.71 and 4.9 ppb), respectively, and the sandal (0.47 and 3.4 ppb), respectively. Mycotoxins were identified in the samples from the crawl space as follows: Wood truss: trichothecenes (1.69 ppb), aflatoxins (3.5 ppb), ochratoxin A (5.8 ppb); Gravel: trichothecenes (7.7 ppb), ochratoxin A (7.7 ppb); Dirt: trichothecenes (2.1 ppb), ochratoxin A (2.1 ppb); and Plastic sheeting: ochratoxin A (2.8 ppb).
9.2. Body Fluids
Mycotoxins detected in body fluids of family members and the pet dog are summarized in Table 5. The father was positive for ochratoxin A in his urine (18.2 ppb), while two separate nasal mucous samples were positive for both aflatoxins (0.5 and 11.2 ppb) and ochratoxin A (18.2 ppb). The mother's urine contained ochratoxin A (18.2 ppb), while nasal mucous contained the three mycotoxins aflatoxin, ochratoxin A, and trichothecenes at 1.02, 1.2, and 1.5 ppb, respectively. The daughter's urine had trichothecenes (0.23 ppb) and ochratoxin (28 ppb), while nasal mucosa had trichothcenes (4.68 ppb) and ochratoxin A (3.8 ppb). The urine sample from the son was positive for ochratoxin A (18.9 ppb), while tests on nasal mucous were not performed. The urine from the pet dog was positive for trichothecenes (1.49 ppb) and ochratoxin A (25.9 ppb).
10. Newborn Baby
The mother gave birth to a girl who was born with a total body flare 3 months after vacating the home (Figure 1). The infant was born with pigmented skin identified as Cafe-au-lait. They are currently distributed as follows: Face (2), neck (6), right axilla (9), left axilla (10), left and right arms (4), abdomen (16), back (28), buttocks (9), right leg (8), and left leg (2) for a total of 84. As a result, breast milk, placenta, umbilical cord, and the baby's urine were tested for the presence of mycotoxins. Ochratoxin A was detected in the breast milk (2.7 ppb), placenta (4.2 ppb), and the umbilical cord (7 ppb). The newborn's urine was negative for mycotoxins. In retrospect, the amniotic fluid (lost during birth) should have been tested.
11. Pet Dog
The pet dog had approximately 72 skin lesions on its legs, trunk, and ears (Figure 2). The lesions were surgically removed. Pathology of the ear mass described it as a sebaceous gland, while the other lesions were lipomas. Tests for mycotoxins in the surgical specimens revealed the following: Ear mass—trichothecenes (23.07 ppb) and ochratoxin A (2.2 ppb); and Lipoma—trichothecenes (20.9 ppb) and ochratoxin A (1.4 ppb). The veterinarian stated that lipomas in dogs are normal; however, the presence of multiple lipomas is a rare occurrence.
12. Discussion
We have presented a family of five who had no history of health problems until they moved into a water-damaged home in Hawaii. Shortly after the move in they began to develop multiple symptoms, sought medical consultation for the health problems involving the upper and lower respiratory tract, headaches, neurocognitive deficits, and severe sinusitis. Neurological evaluation revealed 17 areas of neurological abnormalities in the two adults, consistent with previous reports [8, 9]. The daughter developed tremors that could be related to exposure to tremorgenic and other mycotoxins [18–22]. The son, age 5 at the time of examination, did not have neurological deficits. However, he did have a variety of symptoms (e.g., nose bleeds, cough, wheeze, and headaches) consistent with exposure to water-damaged indoor environments. In addition, when he began school, the teacher reported lack of concentration while in class. Perhaps he was showing signs of autistic spectrum disorder and/or ADD/ADHD as previously reported in children exposed to water-damaged home environments [10].
The parents and the two children have chronic sinusitis and nasal inflammation. The isolation of bacteria (Pseudomonas and Acinetobacter) and molds (Penicillium and Aspergillus) from nasal secretions from the father and daughter is consistent with the literature. Bacterial and fungal sinusitis has been reported [1, 5, 6, 23–25]. In addition, the detection of mycotoxins in the nasal secretions from the family points towards fungal rhinosinusitis. Finally, the culture of surgical specimens taken from the daughter's sphenoid/ethmoid mucosa identified Aspergillus fumigatus.
Macrocyclic trichothecenes and tremorgens have been detected in airborne fungal fragments less than the size of conidia [22, 41–43]. Furthermore, trichothecenes, aflatoxins, sterigmatocystin, ochratoxin A, and other mycotoxins are present in the dust of water-damaged buildings [13, 16]. In addition, indoor microbial growth fragments, releasing particulates less than one micron that penetrate deep into the alveolar spaces [44–46]. Thus, the presence of trichothecenes, ochratoxin A, and aflatoxins in bulk samples (Table 4) and body fluids of the family (Table 5) is interpreted as an inhalation exposure resulting in uptake of mycotoxins attached to dust and fine microbial particulates. Moreover, it is reported in this issue and elsewhere that these mycotoxins are present in the urine and tissue biopsy/necropsy materials taken from individuals residing in water-damaged homes and buildings [42, 47–50].
The newborn girl had a total body flare at birth that began to clear at 10–12weeks after birth, which may have been associated with mast cell/eosinophil activity. However, medical workup was not done in this area. The body flaring periodically appeared until approximately 55 months of age. The majority of the Cafe-au-Lait spots were apparent soon after delivery and continued to develop after birth and continue to be present (Figure 1). She was diagnosed with NF1 by Dr. Frieden at U.C.S.F. at age 2, and additional diagnostics are anticipated. The placenta, umbilical, breast milk, urine, and nasal secretion of the mother were positive for Ochratoxin A (Table 5), while a urine sample from the infant was negative. It is reasoned that amniotic fluid (lost at birth) would have been a better choice for mycotoxin testing. However, the presence of ochratoxin A in the placenta and umbilical cord suggests that the infant most likely was exposed in utero. There is no family history of NF1 leading Dr. Frieden with conclusion that the mutation to NF1 gene most likely occurred sometime during in utero development. It is possible that her condition could be related to ochratoxin A or other toxins known to be present in water-damaged buildings.
A few comments are in order regarding the pet dog. The dog developed 72 cutaneous lesions that were distributed over its body, including the ears (Figure 2). The dog's urine was positive for ochratoxin A and trichothecenes. In addition, surgical specimens of the ear (sebaceous gland) and body tumors (lipomas) were also positive for trichothecenes and ochratoxin A. The question that arises is were the growths caused by the mycotoxins or were they storage sites for the toxins.
In conclusion, a family of five (one in utero) was exposed to several species of mold and bacteria while occupying a water-damaged home. They presented with multiple symptoms, including chronic sinusitis, fatigue, and neurological complaints. Testing of the home revealed the presence of both mold and bacteria. Differential diagnostic procedures demonstrated in up to seventeen areas of central nervous system deficits as well as chronic fungal/bacterial sinusitis.
Mycotoxins testing demonstrated that ochratoxin A was the predominant mycotoxin in samples of urine, nasal secretions, breast milk, placenta, and umbilical cord. Lesser concentrations of macrocyclic trichothecenes were also detected. A newborn girl had a total body flare and had Cafe-au-Lait pigmentation spots. The infant is scheduled for further evaluation for her NF1 condition. This case study indicates that mold and bacteria and by-products in water-damaged homes are most likely the cause of the adverse health conditions of these occupants.
Disclosure
Jack Dwayne Thrasher, Ph.D, is semiretired. He has consulted to the practice of Dr. Gray. He has been an expert witness in both defense and plaintiff cases regarding toxic exposures. Michael A. Gray, M.D, is in private practice in Benson, Arizona. He has been an expert witness in both defense and plaintiff cases involving toxic exposures. Kaye H. Kilburn, M.D, is a Professor Emeritus, USC Keck School of Medicine. He has been an expert witness in plaintiff cases. Donald P. Dennis, M.D, is in private practice specializing in ENT. He has no other conflict of interest. Archie Yu MS, CIH, is the owner and operator of Compliance Solution. He performs industrial hygiene evaluations for both industry and private citizens.
References
- 1.Fisk WJ, Eliseeva EA, Mendel MJ. Association of residential dampness and mold with respiratory tract infections and bronchitis: a meta-analysis. Environmental Health. 2010;9(72) doi: 10.1186/1476-069X-9-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mendell MJ, Mirer AG, Cheung K, Tong M, Douwes J. Respiratory and allergic health effects of dampness, mold, and dampness-related agents: a review of the epidemiologic evidence. Environmental Health Perspectives. 2011;119(6):748–756. doi: 10.1289/ehp.1002410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mudarri D, Fisk WJ. Public health and economic impact of dampness and mold. Indoor Air. 2007;17(3):226–235. doi: 10.1111/j.1600-0668.2007.00474.x. [DOI] [PubMed] [Google Scholar]
- 4.Park JH, Cox-Ganser JM. Mold exposure and respiratory health in damp indoor environments. Frontiers in Bioscience E. 2011;3:575–571. doi: 10.2741/e284. [DOI] [PubMed] [Google Scholar]
- 5.Dennis DP. Chronic sinusitis: defective T-cells responding to superantigen treated by reduction of fungi in the nose and air. Archives of Environmental Health. 2004;58(7):433–441. doi: 10.1080/00039896.2003.11879144. [DOI] [PubMed] [Google Scholar]
- 6.Dennis D, Robertson D, Curtis L, Black J. Fungal exposure endocrinopathy in sinusitis with growth hormone deficiency: Dennis-Robertson syndrome. Toxicology and Industrial Health. 2009;25(9-10):669–680. doi: 10.1177/0748233709348266. [DOI] [PubMed] [Google Scholar]
- 7.Empting L. Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure. Toxicology and Industrial Health. 2009;25(9-10):577–582. doi: 10.1177/0748233709348393. [DOI] [PubMed] [Google Scholar]
- 8.Kilburn KH. Role of molds and mycotoxins in being sick in buildings: neurobehavioral and pulmonary impairment. Advances in Applied Microbiology. 2004;55:339–359. doi: 10.1016/S0065-2164(04)55013-X. [DOI] [PubMed] [Google Scholar]
- 9.Kilburn KH. Neurobehavioral and pulmonary impairment in 105 adults with indoor exposure to molds compared to 100 exposed to chemicals. Toxicology and Industrial Health. 2009;25(9-10):681–692. doi: 10.1177/0748233709348390. [DOI] [PubMed] [Google Scholar]
- 10.Kilburn KH, Thrasher JD, Immers NB. Do terbutaline- and mold-associated impairments of the brain and lung relate to autism? Toxicology and Industrial Health. 2009;25(9-10):703–710. doi: 10.1177/0748233709348391. [DOI] [PubMed] [Google Scholar]
- 11.Rea WJ, Didriksen N, Simon TR, Pan Y, Fenyves EJ, Griffiths B. Effects of toxic exposure to molds and mycotoxins in building-related illnesses. Archives of Environmental Health. 2004;58(7):399–405. doi: 10.1080/00039896.2003.11879140. [DOI] [PubMed] [Google Scholar]
- 12.Rea WJ, Pan Y, Griffiths B. The treatment of patients with mycotoxin-induced disease. Toxicology and Industrial Health. 2009;25(9-10):711–714. doi: 10.1177/0748233709348281. [DOI] [PubMed] [Google Scholar]
- 13.Bloom E, Nyman E, Must A, Pehrson C, Larsson L. Molds and mycotoxins in indoor environments–a survey in water-damaged buildings. Journal of Occupational and Environmental Hygiene. 2009;6(11):671–678. doi: 10.1080/15459620903252053. [DOI] [PubMed] [Google Scholar]
- 14.Thrasher JD, Crawley S. The biocontaminants and complexity of damp indoor spaces: more than what meets the eyes. Toxicology and Industrial Health. 2009;25(9-10):583–615. doi: 10.1177/0748233709348386. [DOI] [PubMed] [Google Scholar]
- 15.Täubel M, Sulyok M, Vishwanath V, et al. Co-occurrence of toxic bacterial and fungal secondary metabolites in moisture-damaged indoor environments. Indoor Air. 2011;21(5):368–375. doi: 10.1111/j.1600-0668.2011.00721.x. [DOI] [PubMed] [Google Scholar]
- 16.Polizzi V, Delmulle B, Adams A, et al. JEM spotlight: fungi, mycotoxins and microbial volatile organic compounds in mouldy interiors from water-damaged buildings. Journal of Environmental Monitoring. 2009;11(10):1849–1858. doi: 10.1039/b906856b. [DOI] [PubMed] [Google Scholar]
- 17.WHO. Dampness and Mould: WHO Guidelines for Indoor Air Quality. Euro Non Serial Publications; 2009. [PubMed] [Google Scholar]
- 18.Ciegler A, Vesonder RF, Cole RJ. Tremorgenic mycotoxins. In: Rodricks JV, editor. Mycotoxins and Other Fungal Related Food Problems. American Chemical Society; 1976. pp. 163–177. (Advances in Chemistry Series no. 149). [Google Scholar]
- 19.Kyriakidis N, Waight ES, Day JB, Mantle PG. Novel metabolites from Penicillium crustosum, including penitrem E, a tremorgenic mycotoxin. Applied and Environmental Microbiology. 1981;42(1):61–62. doi: 10.1128/aem.42.1.61-62.1981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Braselton WE, Rumler PC. MS/MS screen for the tremorgenic mycotoxins roquefortine and penitrem a. Journal of Veterinary Diagnostic Investigation. 1996;85(4):515–518. doi: 10.1177/104063879600800427. [DOI] [PubMed] [Google Scholar]
- 21.Khoufache K, Puel O, Loiseau N, et al. Verruculogen associated with Aspergillus fumigatus hyphae and conidia modifies the electrophysiological properties of human nasal epithelial cells. BMC Microbiology. 2007;7, article 11 doi: 10.1186/1471-2180-7-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kosalec I, Klarić MŠ, Pepeljnjak S. Verruculogen production in airborne and clinical isolates of Aspergillus fumigatus Fres. Acta Pharmaceutica. 2005;55(4):357–364. [PubMed] [Google Scholar]
- 23.Coffey CS, Sonnenburg RE, Melroy CT, Dubin MG, Senior BA. Endoscopically guided aerobic cultures in postsurgical patients with chronic rhinosinusitis. American Journal of Rhinology. 2006;20(1):72–76. [PubMed] [Google Scholar]
- 24.Chakrabarti A, Denning DW, Ferguson BJ, et al. Fungal rhinosinusitis: a categorization and definitional schema addressing current controversies. Laryngoscope. 2009;119(9):1809–1818. doi: 10.1002/lary.20520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mantovani K, Bisanha AA, Demarco RC, Tamashiro E, Martinez R, Anselmo-Lima WT. Maxillary sinuses microbiology from patients with chronic rhinosinusitis. Brazilian Journal of Otorhinolaryngology. 2010;76(5):548–551. doi: 10.1590/S1808-86942010000500002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Barkman J. Home Inspection Report. Kihei, Hawaii, USA: 2009. [Google Scholar]
- 27.Engineering Dynamics Corp. Maui, Hawaii, USA: Dizy Residence Report. [Google Scholar]
- 28.Pugliese. Multiple testing parameters of water damaged buildings. The Canadian Journal of Environmental Education. In press. [Google Scholar]
- 29.Feltman H, Schubert G, Khan S, Jain M, et al. Prevalence of type III secretion genes in clinical and environmental isolates of Pseudomonas aeruginosa . Journal of Microbiology. 2001;147:2659–2669. doi: 10.1099/00221287-147-10-2659. [DOI] [PubMed] [Google Scholar]
- 30.Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. American Journal of Respiratory and Critical Care Medicine. 2007;175(4):367–416. doi: 10.1164/rccm.200604-571ST. [DOI] [PubMed] [Google Scholar]
- 31.Kapadia M, Rolston KVI, Han XY. Invasive Streptomyces infections: six cases and literature review. American Journal of Clinical Pathology. 2007;127(4):619–624. doi: 10.1309/QJEBXP0BCGR54L15. [DOI] [PubMed] [Google Scholar]
- 32.Copeland S, Warren HS, Lowery SF, et al. Acute respiratory response to endotoxin in mice and humans. Clinical and Diagnostic Laboratory Immunology. 2005;12:60–57. doi: 10.1128/CDLI.12.1.60-67.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Martinez FD. CD14, endotoxin, and asthma risk: actions and interactions. Proceedings of the American Thoracic Society. 2007;4(3):221–225. doi: 10.1513/pats.200702-035AW. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rylander R. Endotoxin and occupational airway disease. Current Opinion in Allergy and Clinical Immunology. 2006;6(1):62–68. doi: 10.1097/01.all.0000202356.83509.f7. [DOI] [PubMed] [Google Scholar]
- 35.Thorn J, Rylander R. Inflammatory response after inhalation of bacterial endotoxin assessed by the induced sputum technique. Thorax. 1998;53(12):1047–1052. doi: 10.1136/thx.53.12.1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Andersson MA, Mikkola R, Kroppenstedt RM, et al. The mitochondrial toxin produced by Streptomyces griseus strains isolated from an indoor environment is valinomycin. Applied and Environmental Microbiology. 1998;64(12):46–67. doi: 10.1128/aem.64.12.4767-4773.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Islam Z, Amuzie CJ, Harkema JR, Pestka JJ. Neurotoxicity and inflammation in the nasal airways of mice exposed to the macrocyclic trichothecene mycotoxin roridin A: kinetics and potentiation by bacterial lipopolysaccharide coexposure. Toxicological Sciences. 2007;98(2):526–541. doi: 10.1093/toxsci/kfm102. [DOI] [PubMed] [Google Scholar]
- 38.Roy-Burman A, Savel RH, Racine S, et al. Type III protein secretion is associated with death in lower respiratory and systemic Pseudomonas aeruginosa infections. Journal of Infectious Diseases. 2001;183(12):1767–1774. doi: 10.1086/320737. [DOI] [PubMed] [Google Scholar]
- 39.Huttunen K, Pelkonen J, Nielsen KF, Nuutinen U, Jussila J, Hirvonen MR. Synergistic interaction in simultaneous exposure to Streptomyces californicus and Stachybotrys chartarum . Environmental Health Perspectives. 2004;112(6):659–665. doi: 10.1289/ehp.6701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hooper DG, Bolton VE, Guilford FT, Straus DC. Mycotoxin detection in human samples from patients exposed to environmental molds. International Journal of Molecular Sciences. 2009;10(4):1465–1475. doi: 10.3390/ijms10041465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Brasel TL, Douglas DR, Wilson SC, Straus DC. Detection of airborne Stachybotrys chartarum macrocyclic trichothecene mycotoxins on particulates smaller than conidia. Applied and Environmental Microbiology. 2005;71(1):114–122. doi: 10.1128/AEM.71.1.114-122.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Brasel TL, Campbell AW, Demers RE, et al. Detection of trichothecene mycotoxins in sera from individuals exposed to Stachybotrys chartarum in indoor environments. Archives of Environmental Health. 2004;59(6):317–323. doi: 10.3200/aeoh.58.6.317-323. [DOI] [PubMed] [Google Scholar]
- 43.Straus DC. The possible role of fungal contamination in sick building syndrome. Frontiers in Bioscience E. 2011;3:562–580. doi: 10.2741/e270. [DOI] [PubMed] [Google Scholar]
- 44.Reponen T, Seo SC, Grimsley F, Lee T, Crawford C, Grinshpun SA. Fungal fragments in moldy houses: a field study in homes in New Orleans and Southern Ohio. Atmospheric Environment. 2007;41(37):8140–8149. doi: 10.1016/j.atmosenv.2007.06.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cho SH, Seo SC, Schmechel D, Grinshpun SA, Reponen T. Aerodynamic characteristics and respiratory deposition of fungal fragments. Atmospheric Environment. 2005;39(30):5454–5465. [Google Scholar]
- 46.Górny RL. Filamentous microorganisms and their fragments in indoor air—a review. Annals of Agricultural and Environmental Medicine. 2004;11(2):185–197. [PubMed] [Google Scholar]
- 47.Hope JH, Hope BE. Ochratoxin-A from inhalation exposure associated with focal segmental glomerulosclerosis: two human cases. The Canadian Journal of Environmental Education. In Press. [Google Scholar]
- 48.Hibi D, Susuki Y, Ishi Y, et al. Site-specific in vivo mutagenicity in the kidney of bpt deta rats given a carcinogenic dose of Ochratoxin A. Toxicological Sciences. 2011;122:406–414. doi: 10.1093/toxsci/kfr139. [DOI] [PubMed] [Google Scholar]
- 49.Palma N, Cinelli S, Sapora O, Wilson SH, Dogliotti E. Ochratoxin A-induced mutagenesis in mamalian cells is consistent with the production of oxidative stress. Chemical Research in Toxicology. 2007;20:1031–1037. doi: 10.1021/tx700027j. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Karmus W, Dimitrov P, Simeonov V, Tsolova S, Batuman V. Offspring of parents with Balkan Endemic Nephropathy have igher C-reactive protein levels suggestive of inflammatory processes: a longitudinal study. BMC Nephrology. 2009;10, article 10 doi: 10.1186/1471-2369-10-10. [DOI] [PMC free article] [PubMed] [Google Scholar]