

Abstract
Presented is a patient with papillary tumor of the pineal region (PTPR), an uncommon and recently recognized neoplasm. As its name implies, PTPR does not arise from the pineal gland itself. The cell of origin is thought to be the specialized ependymocytes of the subcommissural organ. Primary tumors of the pineal region include pineal parenchymal neoplasms, germ cell neoplasms, and tumors arising from adjacent structures, including meningiomas, astrocytomas, and ependymomas. Like other masses in this location, PTPR often leads to obstructive hydrocephalus. Due to the relative paucity of reported cases of PTPR, its natural history is unknown.
A 32-year-old man presented with worsening headaches and visual disturbances of several months' duration. Noncontrast computed tomography (CT) revealed a 1-cm mass near the posterior aspect of the third ventricle, which resulted in obstructive hydrocephalus. The third and lateral ventricles were enlarged (Figure 1).
Figure 1.

CT of the brain showing a small mass in the region of the pineal gland (arrow) with enlargement of the third and lateral ventricles (arrowhead).
Brain magnetic resonance imaging (MRI) was subsequently performed before and after intravenous administration of gadolinium contrast material. A precontrast sagittal T1-weighted image showed a mass in the region of the pineal gland, with a thin rim of intrinsic signal hyperintensity and enlargement of the third and lateral ventricles (Figure 2). Postcontrast sagittal and axial T1-weighted images showed avid enhancement of this mass with no additional enhancing lesions (Figure 3). A third ventriculostomy was performed, and the mass was biopsied. Tissue sampling revealed histologic results consistent with PTPR.
Figure 2.
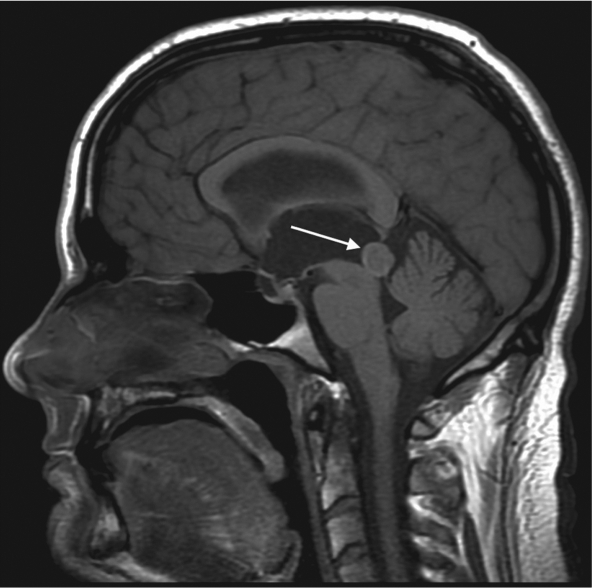
Precontrast sagittal T1-weighted MRI showing a mass in the region of the pineal gland, with a thin rim of intrinsic signal hyperintensity (arrow).
Figure 3.

Postcontrast (a) sagittal and (b) axial T1-weighted images showing an avidly enhancing mass (arrows).
DISCUSSION
The normal pineal gland secretes melatonin and is located in the supratentorial midline, above the superior colliculi and below the vein of Galen. Tumors of the pineal region account for <1% of intracranial neoplasms in adults (1). Primary tumors of the pineal region include pineal parenchymal neoplasms, germ cell neoplasms, and tumors arising from adjacent structures, including meningiomas, astrocytomas, and ependymomas (1). Pineal parenchymal tumors include the relatively indolent pineocytoma and the highly malignant pineoblastoma. Both of these entities appear as lobular, enhancing masses centered in the pineal gland that displace the normal pineal calcifications peripherally (1). Germ cell tumors include germinoma and teratoma. Pineal cysts are considered a normal finding, occurring in up to 40% of patients (1). When they occur in the pineal region, dermoid and epidermoid cysts image similarly to those that occur elsewhere in the central nervous system. Metastases to the pineal gland often result from primary tumors of the lung, breast, colon, and kidney (1).
As its name implies, PTPR does not arise from the pineal gland itself. The cell of origin is thought to be the specialized ependymocytes of the subcommissural organ (2). The subcommissural organ is involved in the secretion of glycopeptides and is located below the posterior commissure at the level of the cerebral aqueduct, just anterior to the pineal gland. It is the glycopeptide content that is thought to be the source of intrinsic T1 hyperintensity commonly reported in PTPR (3).
On imaging, PTPR appears as a heterogeneously enhancing mass arising from the pineal region. Like other masses in this location, obstructive hydrocephalus is a common secondary finding (1). No specific imaging features are pathognomonic for PTPR. However, intrinsic T1 hyperintensity has been reported as a potentially characteristic feature of this neoplasm (3). Hemorrhagic and lipid-containing lesions of the pineal region can also demonstrate T1 shortening and may be excluded from the differential diagnosis by the use of additional sequences such as fat suppression and susceptibility weighted imaging (2). The entire neuraxis should be imaged, as leptomeningeal seeding has been documented (2). Surgical resection followed by radiotherapy is the preferred treatment (4).
Due to the relative paucity of reported cases of PTPR, its natural history is unknown. Histologic grading criteria remain undefined, but will likely correspond to World Health Organization grade II or III (1).
References
- 1.Smith AB, Rushing EJ, Smirniotopoulos JG. From the archives of the AFIP: Lesions of the pineal region: radiologic-pathologic correlation. Radiographics. 2010;30(7):2001–2020. doi: 10.1148/rg.307105131. [DOI] [PubMed] [Google Scholar]
- 2.Chang AH, Fuller GN, Debnam JM, Karis JP, Coons SW, Ross JS, Dean BL. MR imaging of papillary tumor of the pineal region. AJNR Am J Neuroradiol. 2008;29(1):187–189. doi: 10.3174/ajnr.A0784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim YH, Kim JW, Park CK, Kim DG, Sohn CH, Chang KH, Park SH. Papillary tumor of pineal region presenting with leptomeningeal seeding. Neuropathology. 2010;30(6):654–660. doi: 10.1111/j.1440-1789.2010.01108.x. [DOI] [PubMed] [Google Scholar]
- 4.Kaloshi G, Rroji A, Lame A, Leka L, Haxhihyseni E, Vreto G, Petrela M. Natural history of papillary tumor of the pineal region: new insights on biological explanation. J Neurooncol. 2010;100(3):487–488. doi: 10.1007/s11060-010-0198-5. [DOI] [PubMed] [Google Scholar]