

Abstract
Background:
Goldenseal (Hydrastis canadensis L.) inhibits various cytochrome P450 (CYP) isoforms such as CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A in vitro. High doses of acetaminophen (APAP) generate the highly reactive intermediate, N-acetyl-p-benzoquinone imine (NAPQI), catalyzed mainly by CYP2E1. The aim of this study was to investigate the hepatoprotective effects of orally administrated goldenseal against APAP-induced acute liver failure (ALF) via inhibition of CYP2E1.
Materials and Methods:
Male Wistar rats were treated orally with goldenseal (300 and 1000 mg/kg) 2, 18, and 26 h before and 6 h after oral APAP (400 mg/kg) administration. Serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) activities as well as serum APAP concentration were evaluated.
Results:
Goldenseal extract inhibited CYP1A2, CYP2D6, CYP2E1, and CYP3A activity, and the inhibitory effect on CYP2E1 was the strongest (IC50 4.32 μg/mL). Treatment with goldenseal (300 mg/kg) significantly attenuated the APAP-induced increase in serum AST and ALT, and the hepatoprotective effect of goldenseal was stronger than that of silymarin (200 mg/kg). Moreover, serum APAP concentration was increased by goldenseal treatment, presumably as a result of the inhibitory effect of goldenseal on the metabolism of APAP to NAPQI.
Conclusion:
These results suggest that goldenseal ameliorates APAP-induced ALF and that this protection can likely be attributed to the inhibition of CYP2E1 activity, which generates the highly reactive intermediate of APAP.
Keywords: Acetaminophen, acute liver failure, CYP2E1, hepatoprotective effect, goldenseal
INTRODUCTION
Acetaminophen (APAP) is one of the most commonly used drugs worldwide to reduce fever in adults and children and is generally considered a safe drug. However, in large single-dose ingestions, it causes acute liver failure (ALF) that may be fatal in both humans and experimental animals.[1–3] Between 400 and 500 deaths occur annually in the United States due to APAP-related liver failure.[4] APAP poisoning currently represents the most common cause of ALF in North America and Europe.[5] Between 1998 and 2007, the adult ALF Study Group enrolled 1147 patients, and the most frequent single cause of ALF, accounting for 46% of cases, was APAP overdose.[4] Availability of APAP as an over-the-counter medication either alone or in combination with other prescription and over-the-counter drugs creates a situation that may lead to exposure to excessive quantities of the drug. Unintentional liver injury from self-medication for pain or fever with daily doses exceeding the recommended 4 g/day is also well recognized. However, unintentional overdosing is usually only recognized after symptoms have developed.[6]
Use of complementary and alternative medicine (CAM) by U.S. adults has increased since 1990, and the most commonly used CAM modality has been herbal therapy, which accounted for about 38 million adults (18.6% of adult population) in 2002.[7] Goldenseal (Hydrastis canadensis L.) is a plant native to North America with a history of use in folk medicine for the treatment of gastrointestinal disturbances, urinary disorders, hemorrhage, inflammation, and various infections. Often combined with echinacea and taken to treat the common cold or upper respiratory tract infections, goldenseal currently ranks among the top-selling botanical supplements in the United States. Recent studies have shown that goldenseal inhibits various cytochrome P450 (CYP) isoforms in vitro, including CYP2C9, CYP2C19, CYP2D6, and CYP3A4.[8–11] Furthermore, it has also been reported that goldenseal inhibits CYP2E1, and this inhibition appeared to be related to the presence in the extract of the alkaloids berberine, hydrastine, and canadine.[12]
With higher dosing, APAP generates the highly reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI) by CYP enzymes. In humans and rodents, CYP2E1 and CYP1A2 are the major enzymes of APAP bioactivation.[13] In particular, CYP2E1 is an important isoform that has been implicated in the generation of reactive oxygen species such as superoxide and hydrogen peroxide and may mediate the toxic effects of a variety of xenobiotic compounds.[14] Furthermore, when CYP2E1-knockout mice were challenged with APAP, they were found to be considerably less sensitive to its hepatotoxic effects than wild-type animals.[15] These results suggest that herbs with the ability to inhibit CYP2E1 may be useful in the prevention of the hepatotoxic effects of APAP overdosing.
Goldenseal, as well as APAP, is most popularly used for cold and flu treatment. This makes it easy to co-administer goldenseal with APAP. Therefore, this study was designed to investigate the hepatoprotective effects of orally administrated goldenseal against APAP-induced ALF via inhibition of CYP2E1.
MATERIALS AND METHODS
Materials
Goldenseal root was purchased from Nature's Way Products (Springville, UT). Silymarin, chlorzoxazone, and carboxymethylcellulose (CMC) were obtained from Sigma Chemical (St. Louis, MO), and APAP, o-acetamidophenol (2-AAP), and phenacetin were obtained from Wako Pure Chemical Institute (Osaka, Japan). In the in vitro analysis, goldenseal was extracted by placing in a 5-fold volume of methanol at 40 °C for 2 h. The resulting extract was filtered and evaporated to dryness using a centrifugal concentrator (DNA-mini, Heto, Denmark).
Animals
All experiments and procedures were approved by the Chiba University Institutional Animal Care and Use Committee. Male Wistar rats, 8 weeks of age, were obtained from Japan SLC Inc. (Hamamatsu, Japan) and housed under controlled conditions of light (07:00-19:00) and temperature (24 °C) with food and water available ad libitum.
Drug treatment regimens
Goldenseal (300 or 1,000 mg/kg) and silymarin (200 mg/kg) were suspended in 0.5% CMC and administered in the morning (09:00) and evening (17:00) on days 1 and 2. Rats were fasted for 24 h starting from day 1 (17:00) but given tap water ad libitum. APAP (400 mg/kg) was suspended in 0.5% CMC (w/v) and administered orally once 2 h after the morning administration of goldenseal or silymarin on day 2 (11:00). APAP non-treatment animals (Nil) were treated with vehicle at each treatment point.
Preparation of hepatic microsomes
After perfusion with 50 mM potassium phosphate buffer (containing 250 mM sucrose and 1.15% KCl, pH 7.4), rat livers were excised, pooled, and homogenized. Next, the liver homogenate was centrifuged at 9,500 × g for 30 min. The supernatant was ultracentrifuged at 105,000 × g for 60 min, and the resulting microsomal pellets were suspended in ice-cold potassium phosphate buffer and ultracentrifuged at 105,000 × g for 60 min. The resulting pellets were homogenized with 50 mM potassium phosphate buffer (containing 0.1 mM EDTA, pH 7.4) at a protein concentration of 20 mg/mL and stored at –80 °C until use. The microsomal protein content was determined by the method of Lowry, using the DC protein assay kit (BIO RAD).
Measurement of CYP isozyme activity
Phenacetin, dextromethorphan, chlorzoxazone, and testosterone are specific substrates for CYP1A2, CYP2D6, CYP2E1, and CYP3A, respectively. To ensure the selectivity of these markers and to represent the concentration of the drug in vitro, the substrate concentration near its Km value was utilized in all incubation samples in the assay. The incubation sample (volume 450 μL) contained hepatic microsomes (1 mg protein/mL), 250 mM potassium phosphate buffer (containing 0.25 mM EDTA, pH 7.4), substrate, and goldenseal extract. The samples were preincubated for 5 min before the addition of NADPH-generation system (1.25 mM β-NADP+ , 12.5 mM G-6-P, 5 mM MgCl2, 4 U G6PDH), following a 60-min incubation at 37 °C. The reactions were terminated by the addition of 400 μL ethyl acetate, and then the internal standard was added. Next, the organic phase was vortexed and centrifuged at 9,100 × g for 5 min to separate protein fractions. The supernatant of each sample was transferred to a clean tube and evaporated to dryness using a centrifugal concentrator. The residues were dissolved in a 100-μL aliquot of the mobile phase and analyzed by high-performance liquid chromatography (HPLC).
Chromatographic conditions
The activity of CYP1A2, CYP2D6, CYP2E1, and CYP3A isozymes was analyzed using different probe drugs with the Shiseido Nanospace SI-2 (Tokyo, Japan) HPLC system.
For CYP1A2, the mobile phase was 90% 50 mM sodium acetate (pH 4.0)/10% acetonitrile, and phenacetin and APAP were detected at a wavelength of 254 nm. A CAPCELLPAK C18 UG120 column (1.5 × 150 mm, 3 μm, Shiseido) was used at 40 °C with a flow rate of 100 μL/min.
For CYP2D6, the mobile phase was 90% 50 mM potassium phosphate buffer (pH 4.0)/10% acetonitrile, and dextromethorphan and dextrophan were detected at a wavelength of 277 nm. A CAPCELLPAK C18 UG120 column was used at 30 °C with a flow rate of 100 μL/min.
For CYP2E1, the mobile phase was 90% 50 mM potassium phosphate buffer (pH 4.0)/10% acetonitrile, and chlorzoxazone and 6-hydroxychlorzoxazone were detected at a wavelength of 290 nm. A CAPCELLPAK C18 AQ column (1.5 × 250 mm, 3 μm, Shiseido) was used at 35 °C with a flow rate of 100 μL/min.
For CYP3A, the mobile phase was 50% methanol/50% water, and testosterone and 6β-hydroxytestosterone were detected at a wavelength of 240 nm. A CAPCELLPAK C18 UG120 column was used at 30 °C with a flow rate of 100 μL/min.
Measurement of serum aminotransferase activities
Blood was collected from the tail vein 8 and 24 h after the administration of APAP. Serum was then obtained by centrifugation at 1,000 × g for 20 min at 4 °C and stored at –30 °C until use. Serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) activities were determined using Transaminase CII-test Wako (Wako Pure Chemical Institute).
Measurement of serum APAP concentration
Blood was collected from the inferior vena cava 8 h after the administration of APAP. Serum was then obtained by centrifugation at 1,000 × g for 20 min at 4°C and stored at –30°C until use. Serum levels of APAP were determined by HPLC. Briefly, 20-μL aliquots of standards or samples were transferred to 1.5-mL Eppendorf centrifuge tubes. A 10-μL aliquot of internal standard solution (2-AAP, 100 μg/mL final concentration) was added to the serum followed by 100 μL ethyl acetate and briefly mixed on a vortex mixer. The mixture was centrifuged at 5,000 × g for 5 min at 4°C to remove precipitated proteins. The supernatant was then transferred to a 1.5-mL Eppendorf centrifuge tube and evaporated to dryness using a centrifugal concentrator (DNA-mini, Heto, Denmark). Then, a 15-μL aliquot of the HPLC mobile phase (96.5% 50 mM sodium acetate/3.5% acetonitrile) was added and transferred to a 250-μL injection vial. A 5-μL aliquot of the sample or standard solution in the injection vial was subjected to HPLC analysis. A Shiseido Nanospace SI-2 HPLC system was used to analyze APAP. A CAPCELLPAK C18 UG120 column was used at 35°C with a flow rate of 100 μL/min. The mobile phase was 96.5% 50 mM sodium acetate (pH 4.0)/3.5% acetonitrile, and APAP was detected at a wavelength of 254 nm.
Statistical analysis
All data are presented as the mean ± SEM. Statistical significance was analyzed using Fisher's least significant difference test for multiple comparisons. Statistical differences between two groups were analyzed using the Student's t-test or Welch's test following an F-test. Differences at P < 0.05 were considered statistically significant. All statistical analyses were conducted using StatLight software (Yukms Co., Ltd. Tokyo, Japan).
RESULTS
CYP isoform activities
An enzymatic assay of the inhibitory effect of goldenseal extract on CYP isoforms was performed. The ability of goldenseal extract to alter four rat hepatic microsomal CYP-marker enzymatic activities, phenacetine deethylation (CYP1A2), dextromethorphan demethylation (CYP2D6), chlorzoxazone hydrocylation (CYP2E1), and testosterone hydroxylation activities (CYP3A), is shown in Table 1. Goldenseal extract inhibited phenacetin de-ethylation, dextromethorphan demethylation, chlorzoxazone hydroxylation, and testosterone hydroxylation activities with interpolated IC50 values of 15.65, 7.35, 4.32, and 52.07 μg/mL, respectively. Goldenseal showed the strongest inhibitory effect on CYP2E1 among all investigated isoforms.
Table 1.
Inhibition of rat cytochrome P450 isoforms by goldenseal and positive controls

Effects on serum AST and ALT activities
Serum AST and ALT activities were assessed 8 and 24 h after a single administration of APAP. Serum AST and ALT activities significantly increased 8 and 24 h after APAP administration. The increase in serum AST and ALT levels 24 h following APAP administration was decreased by both goldenseal (300 and 1000 mg/kg) and silymarin (200 mg/kg), but only goldenseal at 300 mg/kg caused a significant reduction [Figure 1b]. Goldenseal, at a dose of 300 mg/kg, only moderately (30–35%) decreased the levels of AST and ALT in serum 8 h after APAP administration [Figure 1a].
Figure 1.
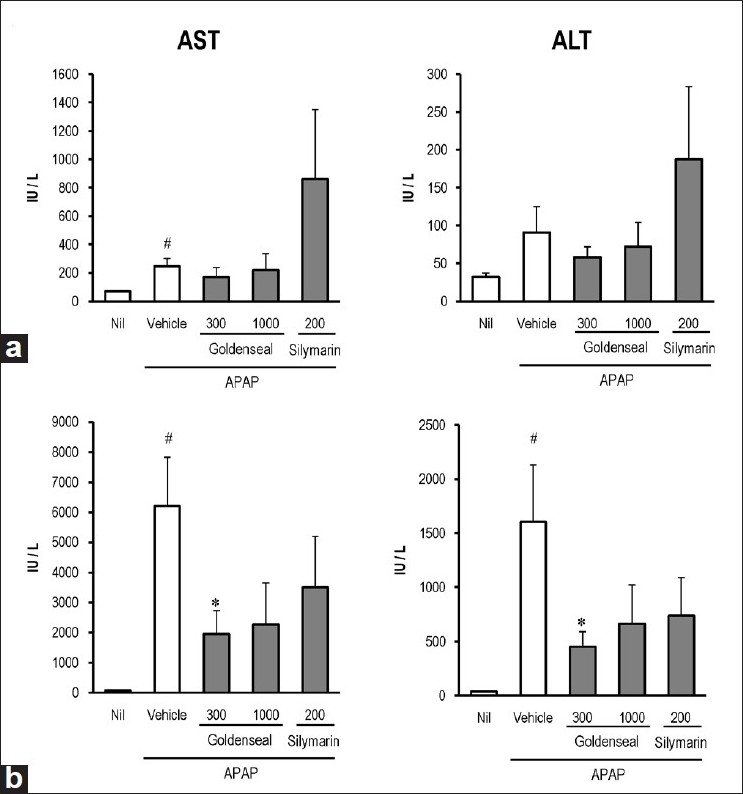
Effects of goldenseal and silymarin on serum AST and ALT activities in APAP-induced liver failure. Rats were administered goldenseal or silymarin 2, 18, and 26 h before and 6 h after oral APAP (400 mg/kg) administration. Blood was collected 8 h (a) or 24 h (b) after APAP administration, and serum AST and ALT activities were determined. Values represent the mean ± SEM of five rats. #P < 0.05 vs. Nil; * < 0.05 vs. vehicle
Effects on serum APAP concentration
In the vehicle group, serum APAP concentration 8 h after the APAP administration was 56.8 ± 7.0 μg/mL. Administration of 300 and 1,000 mg/kg goldenseal enhanced the APAP concentration by 38.2% and 19.5%, respectively, compared with the vehicle group [Figure 2]. Silymarin treatment, as a positive control, also increased the APAP concentration by 30.6% compared with vehicle control.
Figure 2.
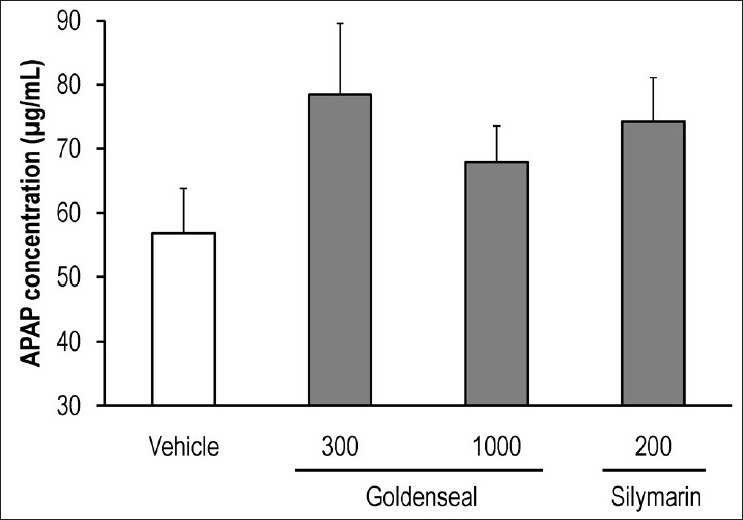
Effects of goldenseal and silymarin on serum APAP concentration in APAP-induced liver failure. Rats were administered goldenseal or silymarin 2, 18, and 26 h before and 6 h after oral APAP (400 mg/kg) administration. Blood was collected 8 h after APAP administration and serum APAP concentrations were determined. Values represent the mean ± SEM of five rats
DISCUSSION
To our knowledge, this is the first study to show the hepatoprotective effects of goldenseal on APAP-induced ALF in rats.
It has been reported that the formation of the highly reactive intermediate, NAPQI, from APAP is mediated by CYP2E1, CYP1A2,[16] CYP3A4,[17] and CYP2D6.[18] In this study, we investigated the inhibitory effect of goldenseal on all cited isoforms and found that goldenseal inhibited CYP1A2 activity in addition to that of the previously reported isoforms, CYP2E1,[12] CYP2D6, and CYP3A4.[9] Furthermore, the inhibitory effect of goldenseal on CYP2E1 was the strongest among the four isoforms we investigated. CYP2E1 has been considered to be a major isoform responsible for the bioactivation of APAP in humans.[19] Recent studies demonstrated that transgenic CYP2E1-knockout mice were considerably less sensitive to APAP hepatotoxicity.[15] In this study, we focused initially on the strong inhibitory effect of goldenseal on CYP2E1 and then investigated its hepatoprotective potential on APAP-induced ALF by concomitant administration of goldenseal plus APAP. As expected, administration of goldenseal, started 1 day before APAP treatment, markedly ameliorated the APAP-induced ALF.
In the clinical setting, serum APAP levels can be useful for determining the severity of injury if the time of ingestion is known.[20] In this study, we measured serum APAP levels to estimate the inhibitory effect of goldenseal on the metabolism of APAP to NAPQI. Oral administration of goldenseal increased the serum concentration of unchanged APAP. We found a strong correlation between the increasing levels of unchanged APAP concentration and the suppressive effect of goldenseal on serum AST and ALT levels. Taken together, these observations suggest that the hepatoprotective effect of goldenseal is due to a decrease in the formation of NAPQI via inhibition of CYP2E1 and other isoforms that metabolize APAP to NAPQI.
Silymarin is hepatoprotective via its antioxidant and cell-regenerating functions[21] and is often used as a positive control for investigating hepatic injury. We found that silymarin increased serum APAP concentration while reducing the elevation of serum aminotransferases. It was reported that silymarin extract showed moderate inhibition of CYP2E1, CYP2D6, and CYP3A4 activities.[22] Therefore, it is likely that the elevation of serum APAP concentration is mediated, at least in part, by the inhibitory effect of silymarin on CYP isoforms.
In this study, the hepatoprotective effects of goldenseal were not dose dependent. It has been reported that APAP-induced ALF is associated with the immune response.[23] Furthermore, goldenseal may enhance immune function.[24] Therefore, it is likely that the immunostimulatory action of a high dose of goldenseal may, at least in part, play a role in reducing the hepatoprotective effect. In addition, it was reported that oral administration of high dose of goldenseal resulted in increased incidences of hepatocyte hypertrophy in the liver of rats.[25] We hypothesized that high dose of goldenseal might induce liver injury. Therefore, the hepatoprotective effect might have been weakened in a high dose of goldenseal. However, further studies are required to confirm these.
In this study, 300 mg/kg of goldenseal was the most effective on hepatoprotective effect in rats. If we convert this animal dose to human equivalent dose based on body surface area, it will be 50 mg/kg (300/6.2). This dosage of goldenseal is within the usual recommended range of supplement doses in human.
Our results suggest that goldenseal might have hepatoprotective effects that ameliorate APAP-induced ALF and that this protection is due to inhibition of CYP2E1 activity, which generates the highly reactive intermediate NAPQI. When APAP is taken to reduce fever caused by, for example, a cold or flu, concomitant use of goldenseal may be useful for preventing APAP-induced ALF as a result of unintentional overdosing.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Black M. Acetaminophen hepatotoxicity. Annu Rev Med. 1984;35:577–93. doi: 10.1146/annurev.me.35.020184.003045. [DOI] [PubMed] [Google Scholar]
- 2.Hinson JA. Reactive metabolites of phenacetin and acetaminophen: A review. Environ Health Perspect. 1983;49:71–9. doi: 10.1289/ehp.834971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Prescott LF, Roscoe P, Wright N, Brown SS. Plasmaparacetamol halflife and hepatic necrosis in patients with paracetamol overdosage. Lancet. 1971;1:519–22. doi: 10.1016/s0140-6736(71)91125-1. [DOI] [PubMed] [Google Scholar]
- 4.Lee WM, Squires RH, Jr, Nyberg SL, Doo E, Hoofnagle JH. Acute liver failure: Summary of a workshop. Hepatology. 2008;47:1401–15. doi: 10.1002/hep.22177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Larsen FS, Kirkegaard P, Rasmussen A, Hansen BA. The Danish liver transplantation program and patients with serious acetaminophen intoxication. Transplant Proc. 1995;27:3519–20. [PubMed] [Google Scholar]
- 6.Larson AM, Polson J, Fontana RJ, Davern TJ, Lalani E, Hynan LS, et al. Acetaminophen-induced acute liver failure: Results of a United States multicenter, prospective study. Hepatology. 2005;42:1364–72. doi: 10.1002/hep.20948. [DOI] [PubMed] [Google Scholar]
- 7.Tindle HA, Davis RB, Phillips RS, Eisenberg DM. Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med. 2005;11:42–9. [PubMed] [Google Scholar]
- 8.Budzinski JW, Foster BC, Vandenhoek S, Arnason JT. An in vitro evaluation of human cytochrome P450 3A4 inhibition by selected commercial herbal extracts and tinctures. Phytomedicine. 2000;7:273–82. doi: 10.1016/S0944-7113(00)80044-6. [DOI] [PubMed] [Google Scholar]
- 9.Foster BC, Vandenhoek S, Hana J, Krantis A, Akhtar MH, Bryan M, et al. In vitro inhibition of human cytochrome P450-mediated metabolism of marker substrates by natural products. Phytomedicine. 2003;10:334–42. doi: 10.1078/094471103322004839. [DOI] [PubMed] [Google Scholar]
- 10.Chatterjee P, Franklin MR. Human cytochrome p450 inhibition and metabolic-intermediate complex formation by goldenseal extract and its methylenedioxyphenyl components. Drug Metab Dispos. 2003;31:1391–7. doi: 10.1124/dmd.31.11.1391. [DOI] [PubMed] [Google Scholar]
- 11.Gurley BJ, Swain A, Hubbard MA, Williams DK, Barone G, Hartsfield F, et al. Clinical assessment of CYP2D6-mediated herb-drug interactions in humans: Effects of milk thistle, black cohosh, goldenseal, kava kava, St.John's wort, and Echinacea. Mol Nutr Food Res. 2008;52:755–63. doi: 10.1002/mnfr.200600300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Raner GM, Cornelious S, Moulick K, Wang Y, Mortenson A, Cech NB. Effects of herbal products and their constituents on human cytochrome P450(2E1) activity. Food Chem Toxicol. 2007;45:2359–65. doi: 10.1016/j.fct.2007.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Shayiq RM, Roberts DW, Rothstein K, Snawder JE, Benson W, Ma X, et al. Repeat exposure to incremental doses of acetaminophen provides protection against acetaminophen-induced lethality in mice: An explanation for high acetaminophen dosage in humans without hepatic injury. Hepatology. 1999;29:451–63. doi: 10.1002/hep.510290241. [DOI] [PubMed] [Google Scholar]
- 14.Castillo T, Koop DR, Kamimura S, Triadafilopoulos G, Tsukamoto H. Role of cytochrome P-450 2E1 in ethanol-, carbon tetrachloride- and iron-dependent microsomal lipid peroxidation. Hepatology. 1992;16:992–6. doi: 10.1002/hep.1840160423. [DOI] [PubMed] [Google Scholar]
- 15.Lee SS, Buters JT, Pineau T, Fernandez-Salguero P, Gonzalez FJ. Role of CYP2E1 in the hepatotoxicity of acetaminophen. J Biol Chem. 1996;271:12063–7. doi: 10.1074/jbc.271.20.12063. [DOI] [PubMed] [Google Scholar]
- 16.Raucy JL, Lasker JM, Lieber CS, Black M. Acetaminophen activation by human liver cytochromes P450IIE1 and P450IA2. Arch Biochem Biophys. 1989;271:270–83. doi: 10.1016/0003-9861(89)90278-6. [DOI] [PubMed] [Google Scholar]
- 17.Thummel KE, Lee CA, Kunze KL, Nelson SD, Slattery JT. Oxidation of acetaminophen to N-acetyl-p-aminobenzoquinone imine by human CYP3A4. Biochem Pharmacol. 1993;45:1563–9. doi: 10.1016/0006-2952(93)90295-8. [DOI] [PubMed] [Google Scholar]
- 18.Dong H, Haining RL, Thummel KE, Rettie AE, Nelson SD. Involvement of human cytochrome P450 2D6 in the bioactivation of acetaminophen. Drug Metab Dispos. 2000;28:1397–400. [PubMed] [Google Scholar]
- 19.Patten CJ, Thomas PE, Guy RL, Lee M, Gonzalez FJ, Guengerich FP, et al. Cytochrome P450 enzymes involved in acetaminophen activation by rat and human liver microsomes and their kinetics. Chem Res Toxicol. 1993;6:511–8. doi: 10.1021/tx00034a019. [DOI] [PubMed] [Google Scholar]
- 20.Smilkstein MJ, Bronstein AC, Linden C, Augenstein WL, Kulig KW, Rumack BH. Acetaminophen overdose: A 48-hour intravenous N-acetylcysteine treatment protocol. Ann Emerg Med. 1991;20:1058–63. doi: 10.1016/s0196-0644(05)81352-6. [DOI] [PubMed] [Google Scholar]
- 21.Pradhan SC, Girish C. Hepatoprotective herbal drug, silymarin from experimental pharmacology to clinical medicine. Indian J Med Res. 2006;124:491–504. [PubMed] [Google Scholar]
- 22.Zuber R, Modrianský M, Dvorák Z, Rohovský P, Ulrichová J, Simánek V, et al. Effect of silybin and its congeners on human liver microsomal cytochrome P450 activities. Phytother Res. 2002;16:632–8. doi: 10.1002/ptr.1000. [DOI] [PubMed] [Google Scholar]
- 23.Masubuchi Y, Sugiyama S, Horie T. Th1/Th2 cytokine balance as a determinant of acetaminophen-induced liver injury. Chem Biol Interact. 2009;179:273–9. doi: 10.1016/j.cbi.2008.10.028. [DOI] [PubMed] [Google Scholar]
- 24.Rehman J, Dillow JM, Carter SM, Chou J, Le B, Maisel AS. Increased production of antigen-specific immunoglobulins G and M following in vivo treatment with the medicinal plants Echinacea angustifolia and Hydrastis canadensis. Immunol Lett. 1999;68:391–5. doi: 10.1016/s0165-2478(99)00085-1. [DOI] [PubMed] [Google Scholar]
- 25.National Toxicology Program. Toxicology and carcinogenesis studies of goldenseal root powder (Hydrastis Canadensis) in F344/N rats and B6C3F1 mice (feed studies) Natl Toxicol Program Tech Rep Ser. 2010;562:1–188. [PubMed] [Google Scholar]