

Abstract
BACKGROUND:
Episiotomy is the incision of perineum made to facilitate childbirth. Here are the two types of episiotomy: median and mediolateral. Considering the important role of incision characteristics such as length, angle and distance of initiation point from midperineum line in prevention of perineal rupture and reduction of further complications, this study investigated the comparison episiotomy in midwives and midwifery and medical students in maternity ward of hospitals of Mashhad University of Medical Sciences.
METHODS:
In this descriptive cross-sectional study, 127 midwives and midwifery and medical students completed the novel validated pictorial questionnaire. The length of episiotomy drawn, the distance from the sagittal plane at which the episiotomy was begun, and the angle of the episiotomy from the sagittal plane were evaluated.
RESULTS:
Median length of the episiotomy from the midline was 2.89 ± 0.95 cm. Episiotomies drawn by midwives more angled than those drawn by students (P = 0.04) and median distance of the episiotomy from the midline in episiotomies drawn by students were significantly more than those drawn by midwives (P = 0.0001).
CONCLUSIONS:
This study demonstrated some differences in the episiotomy practice by midwives and midwifery and medical students. The differences demonstrated could predispose mothers to a greater risk of anal sphincter injuries and subsequence complications in child birth.
KEY WORDS: Episiotomy, midwife, medical student, normal vaginal delivery, perineum injury
Episiotomy is incision of the pudenda. Perineotomy is incision of the perineum. In common parlance, however, the term episiotomy often is used synonymously with perineotomy, a practice that we follow here.1–4 Episiotomy is one of the most commonly performed procedures in obstetrics.5 Traditionally, episiotomy was believed to prevent perineal damage, urinary incontinence, anal incontinence, pelvic floor relaxation and protect the newborn from intracranial haemorrhage and intrapartum asphyxia.6
In general, two types of episiotomy have been described: median episiotomy and mediolateral episiotomy. The incision may be made in the midline (vertical incision in the direction of the anal sphincter) creating a median or midline episiotomy or it may begin in the midline but be directed laterally and downward away from the rectum (incision directed towards the ipsilateral ischial tuberosity), termed a mediolateral episiotomy.4–7 The purpose of this procedure was to facilitate completion of the second stage of labor, to prevent perineal trauma and to reduce the risk of anal sphincter injury.5,8 The advantages and disadvantages of the two types of episiotomies are summarized in Table 1.
Table 1.
Comparison of median and mediolateral episiotomies

Many obstetric units in North America favour the midline episiotomy; by contrast, mediolateral episiotomy is most popular in Europe. Midline episiotomy when compared with mediolateral episiotomy is associated with significantly higher rates of third degree perineal tears.4,7,9 The timing of incision, the technique of performing (the type of incision) and the technique of repair have long been the subjects of debate and it is evident that not all episiotomies are the same.4,5 Recently, Tincello et al. have demonstrated differences in the reporting of episiotomy practice by doctors and midwives.8
Andrews et al. have demonstrated that mediolateral episiotomy performed by obstetricians were significantly longer and more angled from the perineal midline than those performed by midwives.7 Eogan et al. have showed that a longer angle of episiotomy was associated with a lower risk of third degree tear.9 Also, a systemic review on Medline and Cochrane Database between 1980 and 2005 performed to describe the different types of episiotomy demonstrated that shorter length and lower angled episiotomies are currently reported for routine practice.10 This difference in technique could predispose women delivered by midwives at greater risk of sustaining anal sphincter injuries. Also, with the restrictive use of episiotomy, midwifery and medical students may be less experienced in the performance of episiotomy, and less convinced of the value of the intervention.8
Furthermore, anecdotal observation in our hospital suggested that midwives and midwifery and medical students were performing episiotomies in a dissimilar fashion. We therefore, designed this study to investigate the episiotomy in midwives and midwifery and medical students in labor and delivery ward of hospitals of Mashhad University of Medical Science.
Methods
This descriptive cross-sectional study was conducted in the labor and delivery unit of Om-ol-Banin, Emam Reza, Ghaem, Hasheminejad hospitals of Mashhad University of Medical Science, Iran in the year 2006. Selected samples were midwives and midwifery and medical students and sample size was determined based on findings from a pilot study.
127 midwives and midwifery and medical students completed the novel validated pictorial questionnaire. Recently, Tincello et al. devised a validated and simple pictorial questionnaire in order to explore possible differences in clinical practice between doctors and midwives in respect to the size and site of episiotomy. A diagram of a crowning head was taken from a midwifery text. This pictorial questionnaire is a reliable tool for assessing episiotomy technique.8
In this study, midwives and midwifery and medical students were asked to mark the size and the site of an episiotomy on the diagram, assuming that an episiotomy was clinically indicated, also asked for details of profession, training and length of time in practice. Measurements taken from the questionnaire included the length of episiotomy drawn, the distance from the sagittal plane at which the episiotomy was begun, and the angle of the episiotomy from the sagittal plane, the perpendicular distance from the sagittal plane to the origin of the episiotomy mark upon the introitus, the length of the mark, and the angle subtended by the mark to the sagittal plane. Distances were measured in millimeters. The questionnaire was piloted on a sample of 25 midwives and midwifery and medical students who completed the two samples of questionnaire approximately 14 days apart. Test-retest reliability of each measurement was measured using a combination of Spearman's correlation for categories and percentage agreement. Test–retest analysis demonstrated the following Kapa coefficients: 0.9 for the start of episiotomy line (distance from the midline), 0.94 for the length of line (size of episiotomy), and 0.8 for the angle from the sagittal plane (laterality). In data analysis, independent t-test and one-way analyses were used to compare the quantitative data with normal distribution between the two groups. Nonparametric Mann-Whitney U test and Kruskal Wallis test were used in analyzing the data with abnormal distribution using SPSS version 14.0.
Results
One hundred and twenty-seven questionnaires were completed, 40 from midwives and 80 from midwifery and medical students. Median length of the episiotomy from the midline was 2.89 (mean) ± 0.95 (SD) cm with no difference between midwives and midwifery and medical students. Median angle of episiotomies from the sagittal plane drawn by for midwives (47.78 ± 9.06°) were more angled than those drawn by midwifery and medical students (43.77 ± 9.9°) (P = 0. 04, Mann-Whitney U test) (Table 2 and Figure 1). Median distance of the episiotomy from the midline for midwives was 0.5 ± 0.89 cm and for midwifery and medical students was 1.42 ± 1.18 cm and the difference was significant (P = 0.0001, t-test, Figure 2).
Table 2.
Differences in angle of episiotomy drawn by midwives and midwifery and medical students

Figure 1.
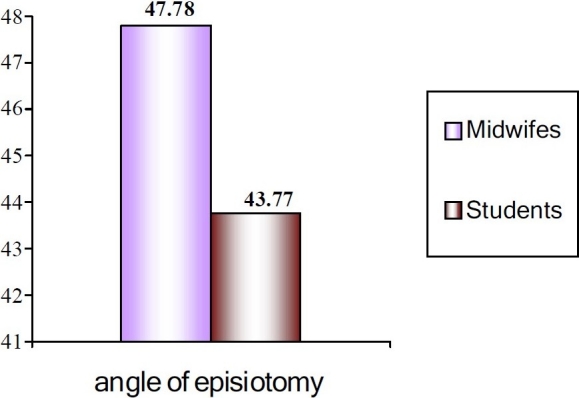
Differences in angle of episiotomy drawn by midwives and students
Figure 2.
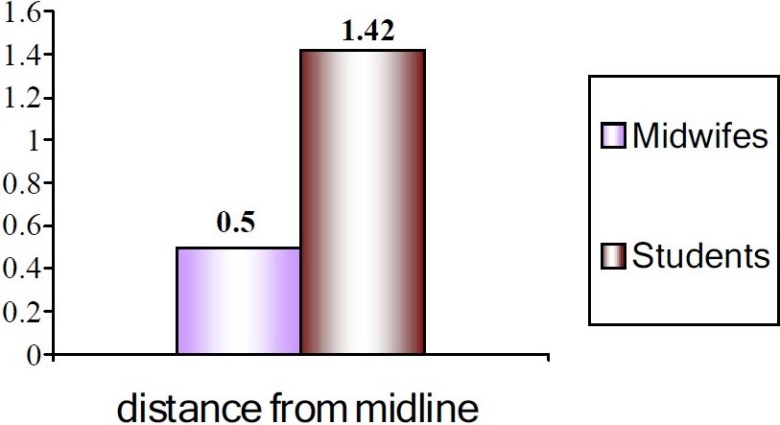
Differences in distance of episiotomy from midline by midwives and students
Discussion
This study demonstrated differences in the episiotomy practice by midwives and midwifery and medical students. Episiotomies drawn by midwives were more angled than those drawn by students. Median distance of the episiotomy from the midline in episiotomies drawn by students was significantly more than those drawn by midwives. Our data demonstrated that the assumption that all professionals perform episiotomy in the same way is not valid, and may reflect a difference in attitude of midwives and midwifery and medical students to perineal damage during normal delivery. Examination of standard texts suggested that episiotomies should begin in the midline with an angle of 45-60°.11–14 In this study, 22 midwives and 17 midwifery and medical students drew an episiotomy with a midline start and angled 40-60°.
These findings objectively confirmed the hypothesis of Tincello et al. and Andrews et al.7,8 who showed similar differences using a pictorial questionnaire. The findings of our study may offer a possible explanation for this finding that most mediolateral episiotomies are not truly mediolateral. However, in order to determine the advantages and disadvantages of episiotomy, the timing, the size and the angle of episiotomy must be standardized. The actual mechanics of the pressure of the fetal head on perineum and the relief of this pressure by an episiotomy are unknown. It is well recognized that midline episiotomy increases the risk of anal sphincter damage, but it is not clear at what angle from the midline, an episiotomy ceases to function as a midline incision and functions as a medio-lateral incision. A subjective consideration of the anatomy of the external anal sphincter would suggest that an angle of about 40° or less is likely to function like a midline incision, however, the differences demonstrated could predispose to a greater risk of anal sphincter injuries and subsequence complications in child birth.
Therefore, when episiotomy is indicated, every effort should be made to ensure that it is truly mediolateral. More intensive training of midwifery and medical students and midwives is clearly required to improve knowledge of anatomy, episiotomy technique and repair. Hands-on perineal workshops appear to be an ideal teaching forum and further studies, comparing reported practice with observation of actual episiotomies, are the obvious and necessary next steps.
The authors declare no conflict of interest in this study.
References
- 1.Sciarra JJ. Philadelphia: Lippincott; 1995. Gynecology and Obstetrics: Obstetrics. [Google Scholar]
- 2.Danforth DN, Scott JR. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2003. Danforth's obstetrics and gynecology. [Google Scholar]
- 3.Enkin MW, Neilson JP. 2nd ed. New York: Oxford University Press; 1999. A guide to effective care in pregnancy and childbirth. [Google Scholar]
- 4.Cunningham FG, Williams W. New York: McGraw-Hill Professional; 2005. Williams obstetrics. [Google Scholar]
- 5.ACOG Practice Bulletin. Episiotomy. Clinical Management Guidelines for Obstetrician-Gynecologists. Number 71, April 2006. Obstet Gynecol. 2006;107(4):957–62. [PubMed] [Google Scholar]
- 6.Sartore A, De Seta F, Maso G, Pregazzi R, Grimaldi E, Guaschino S. The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstet Gynecol. 2004;103(4):669–73. doi: 10.1097/01.AOG.0000119223.04441.c9. [DOI] [PubMed] [Google Scholar]
- 7.Andrews V, Thakar R, Sultan AH, Jones PW. Are mediolateral episiotomies actually mediolateral? BJOG. 2005;112(8):1156–8. doi: 10.1111/j.1471-0528.2005.00645.x. [DOI] [PubMed] [Google Scholar]
- 8.Tincello DG, Williams A, Fowler GE, Adams EJ, Richmond DH, Alfirevic Z. Differences in episiotomy technique between midwives and doctors. BJOG. 2003;110(12):1041–4. [PubMed] [Google Scholar]
- 9.Eogan M, Daly L, O’Connell PR, O’Herlihy C. Does the angle of episiotomy affect the incidence of anal sphincter injury? BJOG. 2006;113(2):190–4. doi: 10.1111/j.1471-0528.2005.00835.x. [DOI] [PubMed] [Google Scholar]
- 10.Verspyck E, Sentilhes L, Roman H, Sergent F, Marpeau L. [Episiotomy techniques] J Gynecol Obstet Biol Reprod (Paris) 2006;35(1 Suppl):1S40–1S51. [PubMed] [Google Scholar]
- 11.Fraser DM, Cooper MA. London: Churchill Livingstone; 2003. Myles textbook for midwives. [Google Scholar]
- 12.Beischer NA, MacKay EV. Episiotomy. In: Beischer NA, MacKay EV, editors. Obstetrics and the newborn: an illustrated textbook. Philadelphia: Saunders; 1986. [Google Scholar]
- 13.Chamberlain G. Obstetric procedures. In: Chamberlain G, editor. Obstetrics by Ten Teachers. London: Arnold; 1995. [Google Scholar]
- 14.Gabbe SG, Niebyl JR, Simpson JL. London: Churchill Livingstone; 2003. Obstetrics: Normal and Problem Pregnancies. [Google Scholar]