

Abstract
Background & objectives:
With advances in knowledge about health promotion, public health professionals are in search for the determinants of personal health behaviours. This study was carried out to explore the level of engagement of north Indian students in health promoting behaviours; to determine their sense of coherence scores; and to ascertain the determinants of health promoting behaviours of these students.
Methods:
A cross-sectional study was done in four randomly selected colleges of Chandigarh during 2007-2008 in 200 students (100 male, 100 female). Their health promoting lifestyle profile (HPLP) and sense of coherence (SOC) scores were estimated using interviews. The data were analyzed using Pearson's product moment correlation, and also stepwise linear regression analysis.
Results:
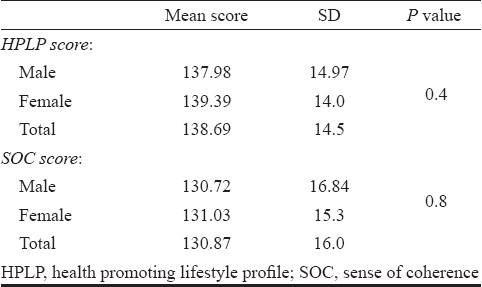
Mean HPLP and SOC scores of the students were 138.69 and 130.87, respectively. Females cared more about their health than males. Male students were more involved in physical activities. There was a linear correlation between the total SOC and HPLP scores (r=0.3). Female students (63%) consulted doctors more than males (50%) and washed their hands more regularly (P<0.05). Only 13 per cent students practiced yoga regularly. Female students had more meaningful relationships with friends and had more faith in God. Regression equation revealed that the two independent variables (SOC and age) accounted for 10.8 per cent of the variance in HPLP.
Interpretation & conclusion:
Students with higher SOC scores had higher HPLP scores. Female students were more health conscious than male students. In general, college students in Chandigarh had a good health promoting lifestyle and good sense of coherence.
Keywords: Health promoting behaviour, health promoting lifestyle profile, lifestyle modifications, salutogenesis, sense of coherence
Health promoting behaviours and psychosocial well being are important determinants of health status and quality of life. Health promoting activities seek to strengthen the host through a variety of approaches in the form of health education, lifestyle modification, ehavior change, environment modification and nutrition intervention. Among these, lifestyle modification was highlighted as a major strategy for prevention of non-communicable diseases during late 20th century.
To a large extent, health is governed by the physical, social, cultural and economic environment in which people live and work. To cajole the individual into taking responsibility for his or her health, while at the same time ignoring the social and environmental circumstances which conspire to make them ill, is a fundamentally defective strategy. In fact, this ‘victim blaming’ orientation of lifestyle approach has been criticized by many experts. Lately, there has been a shift in focus of health care experts toward the role of positive aspects of individual personality in diseases prevention. Individual responsibility is now sought to be differently analyzed as far as determinants of health behaviours or health promotion are concerned. This shift in focus is attributed to introduction of concepts like salutogenesis and people's sense of coherence (SOC). The term Salutogenesis1,2 [Salus (Latin): health, genesis (Greek): origin or giving birth] deals with study of origin or sources of health. This salutogenic concept focuses on elements or factors that help a person to cope with stress, other physical and psychological problems or even exposure to pathogenic factors. It also explores the sources of self-regeneration and self-healing power. This model seeks to explain why some people are able to maintain and even improve their health in stressful life situations.
This approach ignores the search for causation of specific disease or health problem as included in the pathogenic model. From therapeutic point of view, the pathogenic model involves the use of healing devices or interventions from outside to eliminate the pathogenic factors. In salutogenic model, the emphasis is on the internal healing resources of individuals, i.e., their potential for active adaptation to new circumstances. However, the salutogenic model is not the substitute, but a supplement to the pathogenic model. It draws the attention of health care professionals towards the neglected facets of pathogenic model.
Salutogenic theory involves two key concepts, viz., sense of coherence (SOC) and general resistance resources (GRRs)3. Sense of coherence is directly related with one's ability to employ cognitive, affective and instrumental strategies that help to improve the capacity to cope with stress. Across the world various cross-sectional studies on salutogenic theory, have shown that a strong SOC enhances well-being4,5. Persons with a strong SOC are less likely to perceive stressful situations as threatening and anxiety provoking than those with a weak SOC.
Sense of coherence may, therefore, provide an important focus for the strategies aiming at lifestyle modification. This relatively new emerging concept can also be considered as a theoretical framework for health promotion6. The salutogenic perspective focuses on three aspects. First, the focus is on problem solving, i.e., finding solutions. Second, it identifies GRRs that help people to move in the direction of positive health. Third, it identifies a global and pervasive sense in individual, groups, population or system that serves as the overall mechanism or capacity for this process, i.e., the development of SOC.
College life is a transitional period, offering opportunities for cementing healthy lifestyle behaviours in students. However, most health professionals do not view this relatively healthy stage of life as a priority for health promotion efforts or for strengthening the positive attitude. Many researchers have tried to ascertain the determinants of health promoting behaviours and of the individual positive health outcomes. Much of the focus has been on locus of control, self-esteem, loneliness, hardiness, resilience and personality type7. SOC has recently emerged as another important concept in this area. However, studies on this aspect are scarce in India.
The present study was therefore, conducted with following objectives: (i) to explore the level of engagement of north Indian students in health promoting behaviours; (ii) to determine their sense of coherence scores; and (iii) to ascertain the determinants of health promoting behaviours of these students.
Material & Methods
This cross-sectional study was carried out during the September 2007 to June 2008 among Indian graduate students (first year BA/BSc) in four randomly selected colleges of Chandigarh, north India. One hundred female students were selected from two randomly selected girls colleges (50 from each college). Likewise, 100 male students were also selected randomly, 50 each from two boys colleges.
Students were asked to gather in a vacant class room on a pre-decided convenient day. Health Promoting Lifestyle Profile (HPLP)8 scale was used to measure health promoting behaviours and Orientation to Life Questionnaire (OLQ-29 version)3 was used to determine the SOC scores. They were asked to encircle one appropriate option for each question. Completed questionnaires were collected on the spot.
HPLP instrument provides a multidimensional assessment of health promoting behaviours and psychosocial well being of individuals8,9. It measures health promoting lifestyles by focusing on self-initiated actions and perceptions that serve to maintain or enhance the level of wellness, self actualization, and fulfillment of individual. It has been used extensively in health promotion research. It was reported to have sufficient validity and reliability for use among various populations including adolescent and young adults9–11.
For the purpose of present study, two items were deleted from the original HPLP, one from ‘physical activities’ subscale, i.e., “Check my pulse rate when exercising” and other one from ‘nutrition habits’ subscale, i.e., “Eat only two to three servings from the meat, poultry, fish, dried beans, eggs each day”. In addition, requisite translation was done which involved changes in some of the terminology/words used in some of the original questions to adapt it locally, e.g., five items from ‘health responsibility’ subscale, four items from ‘physical activities’ subscale, two items from ‘nutrition habits’ subscale, one item from ‘interpersonal relationship’ subscale, three items from ‘stress management’ and one item from ‘spiritual growth’ subscale.
So, a total 50 items were prepared and grouped into six subscales: (i) Health responsibility: This had nine items focused on the individual's general health concerns, e.g., “Consult a doctor whenever have any health problem”. (ii) Physical activities: there were seven items in this subscale about exercise and recreational activities, e.g., “Do exercise such as brisk walking/aerobics”. (iii) Nutrition habits: This subscale contained eight items on nutrition, dealing with choices of a good and balanced diet. e.g. “Make effort to’ choose low fat diet”. (iv) Stress management: This had eight questions on relaxation methods to control stress, e.g., “Practice relaxation or meditation techniques”. (v) Interpersonal relationship: This had nine questions dealing with meaningful relationships with friends and others, e.g.,“Spend time with close friends”. (vi) Spiritual growth: Its items referred to one's attitude towards life, e.g., “Remain hopeful about future”.
Each item was scored through a fixed 4-point Likert-type format, where “never” was coded as 1, “sometimes” as 2, “often” as 3, and “routinely” as 4. The term “routinely” was chosen to represent the most frequent response category because it suggested a regular pattern of behaviours or characteristic of lifestyle. Six items were negatively stated. Before computing the total score, necessary reversion was done. To calculate a mean score, the scores for all items were summed and then divided by the numbers of items. Higher mean scores denoted positive health promoting lifestyle or behaviours. The internal consistency, reliability coefficients for total scale, and subscales ranged from 0.7-0.85. The original HPLP had reliability with internal consistency for the total score and subscale ranging from 0.7-0.928.
The OLQ-29 version was used to estimate SOC scores of individuals. It consisted of eight items for manageability, 11 items for comprehensibility and 10 for meaningfulness3. The OLQ has shown to have good stability, reliability and validity4. The necessary language modification in OLQ was done in order to adapt it locally. All the OLQ Items were fitted to a seven-point Likert scale. Each option was explained to the students to make the OLQ understandable. Seventeen items were negatively stated. These were reversed before the total score was computed. Total possible score ranged from 29 to 203. A higher score reflected a strong SOC. Cronbach alpha was 0.85, indicating adequate internal consistency.
For item analysis of HPLP, only those who reported “often” or ‘routinely” or similar option or those who got 3 or 4 score in each items were considered as practicing health promoting ehavior. Those who reported “never” or “sometimes” and got a score of 1 or 2 were considered as not practicing the particular health promoting ehavior. For SOC, the first three responses were considered as a low score and last three as a higher score. The 4th response was considered as equivocal.
Ethical consideration: Ethical clearance was obtained from Institute Ethics Committee of PGIMER. Permission to carry out the study was obtained from vice chancellor of the university and from the concerned principals of the various colleges. The cover pages of the questionnaires briefly explained about the study and provided instructions to the respondents on how to fill it up. It also provided information about the researcher. It also mentioned that anonymity and confidentiality would be maintained and that the participation of students was voluntary. It specified that data would be used only for research purposes.
Statistical analysis: The data were analyzed using SPSS for Windows, version 16 (Chicago, Illinois, USA). Descriptive statistics was used to calculate frequency of health promoting ehavior of study population. In order to compare mean score, t-test for independent samples was used. For item-wise difference of HPLP in male and female students χ2 test was used. The SOC and HPLP scores were correlated by using Pearson's product moment correlation. Stepwise linear regression analysis was also performed with HPLP as a dependent variable. SOC and other socio-demographic characteristics were taken as independent variables. P<0.05 was considered significant.
Results
HPLP questionnaires were completely filled up by both the groups of students without missing any item. In OLQ, 6 items were missed by 5 students. The missing values were replaced by the mean value of the remaining SOC items of the individual5. Table I shows gender wise difference in health promoting behaviour subscales. Table II shows HPLP and SOC scores of the students. The mean age of students was 18.67 ± SD yr (range 17-25 yr).
Table I.
Gender difference in health promoting behaviour of the study population (N=200; M=100, F=100)
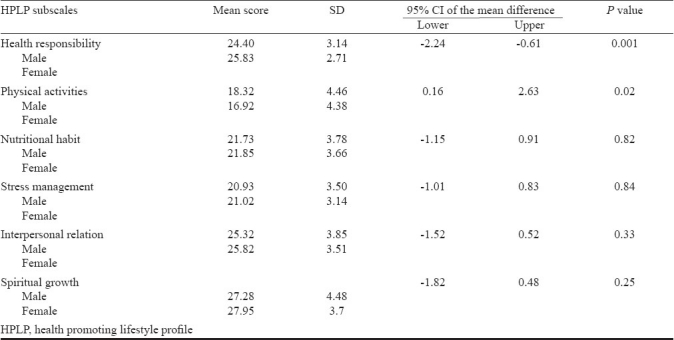
Table II.
Mean HPLP and SOC score of the students (N=200; M=100, F=100)
Female students consulted doctors more frequently for their health problems as compared to male students (P<0.05). Very few students searched health related articles (18.5%) from internet; one fourth went for health check-up (26%) in the last year. Overall, female students showed more sense of health responsibility than male students. More than one third of students indulged in bicycling or morning walk. Gender-wise, significantly more male students did muscle stretching exercise (55 vs 34%; P<0.05) and played outdoors game than female students (59 vs 21%; P<0.05). Female students practiced yoga more frequently than their male counterpart (18 vs 9%; P<0.05). Males were significantly more involved in physical activities than female students. One fourth students made effort to choose a diet low in fat or sugars. More of female students reported that they read labels to identify the foods contents more than males (68 vs 55%; P<0.05). Female students consumed processed/fast food more regularly than males (31 vs 20%; P<0.05).
In stress management subscale, no statistically significant difference was found between the responses of male and female students. Half of the students used various stress control methods such as watching TV, movies and going for shopping, etc. More than half of the students got enough time to sleep regularly (65%) and shared their feeling with friends (59%). Relaxation/meditation was practiced by 21 per cent students.
Three items of interpersonal relation subscale, i.e., “Maintain and meaningful relationships with friends” (88 vs 77%; P<0.05), “Do find way to meet your friends” (75 vs 61%; P<0.05), “Listen to your friends’ problems” (91 vs 78%; P<0.05) were reported more by female students as compared to male students. More female students had faith in God than male students (92 vs 77%; P<0.5). More female students reported that they knew what was important in life (89 vs 79%; P<0.05). There was no significant gender-wise difference in the overall HPLP and SOC scores (Table II).
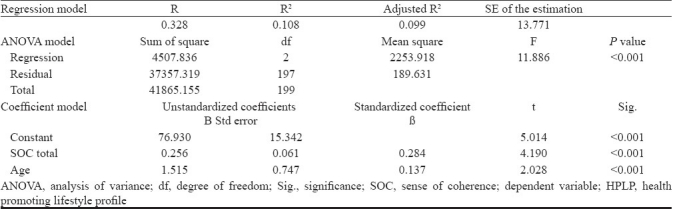
The univariate analysis showed no significant association between gender, religion, father's education and type of accommodation with HPLP. But it showed significant association between SOC scores and age of students. There was a significant correlation between SOC scores and age with HPLP scores of male and female students (r=0.328, P<0.001, Table III). The regression model showed that two independent variables (SOC and age) accounted for 10.8% (R2: 0.108) of the variation in HPLP. The linear regression of SOC and age with HPLP was also significant (F=11.886, P<0.001, Table III). The regression coefficients of SOC and age were 0.256 and 1.515, respectively.
Table III.
Independent variables of HPLP according to stepwise linear regression analysis
Discussion
Sense of coherence is a theoretical construct defined to represent the belief that what happens in life is comprehensible, manageable, and meaningful. Salutogenesis is hypothesized as a flexible and adaptive dispositional orientation of life that enables our successful coping with adverse experiences. SOC score reflects the inclination and capacity of a person to cope with stressors and his or her predisposition to maintenance of good health. Actual engagement in health maintaining action is reflected by HPLP score. So, it can be anticipated that if the SOC score is high, one is more likely to have better HPLP score. Our study also demonstrated a positive correlation between HPLP and SOC scores of students. Similar results have been reported elsewhere. For instance, in a recent pilot study of Finnish polytechnic students, extent of involvement in physical activity was positively correlated with the SOC score12. In other studies it was found that strong SOC was also associated with lower rates of cigarette smoking13 and drinking behaviours14. Norfolk population based cohort study reported a strong correlation of SOC with healthier behaviours choices, independently of social class and education15. In a study from Sweden, SOC was shown to correlate significantly with healthier dietary habits among adults16. Another study revealed that SOC was strongly related with self-rated health score and possession of health promoting resources that support the development of a positive subjective state of health17. A recent prospective study (19 years follow up) in Finland showed that a strong SOC was associated with reduced risk of psychiatric disorders18.
It has also been suggested that in non-smokers, an improvement in exercise enhances natural killer cell activity through an increased SOC19. In a study among homeless or drug-abusing minority women, it was revealed that subjects with higher SOC scores reported significantly fewer high risk behaviours, such as use of intravenous drugs, frequent unprotected sex, or a history of a sexually transmitted disease20.
Among pregnant women, a significant difference in SOC scores was shown between smoking and non-smoking women . Women who relapsed to smoking had a weaker level of SOC, particularly in the manageability component21. In a study among sexually abused women22, it was shown that chronic cannabis users generally had weak SOC scores. But after six weeks of treatment, the scores increased to same range as observed in the normal control group23. SOC has also been found to be associated with more general indices of lifestyle24. A recently published longitudinal study supports the notion that a weakened SOC accompanying smoking and alcohol consumption may partially cause a pathogenic process following a negative life event in initially healthy participants25. Prospective study on the participants Helsinki Heart Clinical Trial also found that SOC was inversely associated with risk of injuries26.
It has been proposed that strong SOC is associated with higher level of education and income. It also has been found to correlate significantly and positively with a wide variety of other psycho-social characteristics, such as self-esteem, locus of control, self motivation inventory and inversely with negative affectivity, depression, psychological distress and anxiety.
In the present study, the mean HPLP and SOC scores indicated that north Indian students had reasonably good health promoting profile as well as salutogenic orientation. Overall, mean HPLP score (139) among our respondents was higher than that of reported in other studies, i.e., 119.78 among Hong Kong university students27, 131.45 among adult women Tuscalosa USA28 and 132.03 in Taiwan women29. This indicates that the lifestyle of educated youth in north India has reasonably good orientation towards health promotion.
In our study, female students had a higher sense of health responsibility than their male counterparts. This was mainly due to a higher rate of consultation with doctors as reported by female students. They also indulged more regularly in the practice of washing their hands before meals. This reflects that female students were more conscious about their health and hygiene than male students. The overall low medical consultation rate (26%) may be due to the younger age of the students who are usually more active physically. College life, in general, represents a relatively healthy part of our life span. Male students were more likely to engage in physical activities than female students. This may be due to the stereotype of more physical active role of males in our society. This reflects that, by nature, male students are more involved in outdoor activities, games and exercise, etc. Yoga was not much popular among students, as only 13.5 per cent of students practiced it. But, female students practiced yoga more than males. This finding is consistent with that of a study in Western society (France, Denmark, Finland, etc.) including USA, where also, yoga was more reported to be popular among women30. According to the most recent worldwide survey, the vast majority of participants in yoga classes were women (77%)31.
One fourth of students reported regular consumption of processed or fast food. However, the frequency of fast food consumption was higher among female students as compared to male students. Another related issue that required attention was that 15 per cent of students smoked and 21 per cent of them took alcohol regularly. Gender-wise, significantly more of male students smoked (24 vs 9%; P<0.05) and consumed alcohol (33 vs 9%; P<0.05) as compared to female students.
Female students reported more meaningful relationship with friends than male students. Since college students spend most of their time with their friends in the class room or on campus, having a meaningful relationship with friends is important for them. More faith in God reported by female students than males may again be due to their nature and the cultural ethos of Indian people where females are more involved in prayers, etc. Similar results were also reported from a survey by the Pew Forum on Religion & Public life, USA and American Religious Identification Survey, 200832,33.
The fact that not many students (18%) used internet regularly for searching health related articles implied that health was not the major agenda for the students as far as use of internet or media is concerned. Similarly, participation in or initiation of health related programmes or activities was also not a routine part of their life. It was not their major concern.
Stepwise linear regression analysis revealed that age and SOC scores were positively related to health promoting behaviours. Another study also reported that SOC is positively correlated with age, i.e., higher the age, stronger the SOC34. Possibly, maturity acquired with age enhances individual SOC. Thus, a good salutogenic orientation as reflected by a higher SOC score as seen in our study, is likely to be a strong determinant of engagement of students in health promoting behaviours.
However, it was a cross-sectional study and the temporal or antecedent consequent relationships between HPLP and SOC scores cannot be established in such studies. Further prospective studies are warranted to understand whether better salutogenic orientation leads to better health promoting behaviours or vice versa.
The limitation of the study is that all the information collected in the study was based on self reporting. Verification of the reported behaviours was not attempted. So, it is likely that some of the students might not have had the opportunity to discuss any difficulty faced by them in understanding the questions.
Acknowledgments
Authors thank Shri Sharad for statistical help in multiple regression analysis.
References
- 1.Antonovsky A. Unraveling the mystery of health - How people manage stress and stay well. 1st ed. San Francisco, CA: Jossey-Bass Publishers; 1987. [Google Scholar]
- 2.Lindstrom B, Eriksson M. Salutogenesis. J Epidemiol Community Health. 2005;59:440–2. doi: 10.1136/jech.2005.034777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36:725–33. doi: 10.1016/0277-9536(93)90033-z. [DOI] [PubMed] [Google Scholar]
- 4.Eriksson M, Lindstrom B. Validity of Antonovsky's sense of coherence scale: a systematic review. J Epidemiol Community Health. 2005;59:460–6. doi: 10.1136/jech.2003.018085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Suominen S, Helenius H, Blomberg H, Uutela A, Koskenvuo M. Sense of coherence as a predictor of subjective state of health: results of 4 years of follow-up of adults. J Psychosom Res. 2001;50:77–86. doi: 10.1016/s0022-3999(00)00216-6. [DOI] [PubMed] [Google Scholar]
- 6.Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. 1996;11:11–8. [Google Scholar]
- 7.Booth-Kewley S, Vickers RR., Jr Associations between major domains of personality and health behavior. J Personal. 1994;62:281–98. doi: 10.1111/j.1467-6494.1994.tb00298.x. [DOI] [PubMed] [Google Scholar]
- 8.Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile: development and psychometric characteristics. Nurs Res. 1987;36:76–81. [PubMed] [Google Scholar]
- 9.Walker S, Sechrist K, Pender N. The health-promoting lifestyle profile II. Omaha: University of Nebraska Medical Center, College of Nursing; 1995. [Google Scholar]
- 10.Acton GJ, Malathum P. Basic need status and health promoting self-care behavior in adults. West J Nurs Res. 2000;22:796–811. doi: 10.1177/01939450022044764. [DOI] [PubMed] [Google Scholar]
- 11.Clement M, Bouchard L, Jankowski LW, Perreault M. Adoption of health promotion behaviors in first-year baccalaureate nursing students: pilot study. Can J Nurs Res. 1995;27:111–31. [PubMed] [Google Scholar]
- 12.Hassmen P, Koivula N, Uutela A. Physical exercise and psychological well-being: a population study in Finland. Prev Med. 2000;30:17–25. doi: 10.1006/pmed.1999.0597. [DOI] [PubMed] [Google Scholar]
- 13.Glanz K, Maskarinec G, Carlin L. Ethnicity, sense of coherence, and tobacco use among adolescents. Ann Behav Med. 2005;29:192–9. doi: 10.1207/s15324796abm2903_5. [DOI] [PubMed] [Google Scholar]
- 14.Midanik LT, Soghikian K, Ransom LT, Polen MR. Alcohol problems and sense of coherence among older adults. Soc Sci Med. 1992;34:43–8. doi: 10.1016/0277-9536(92)90065-x. [DOI] [PubMed] [Google Scholar]
- 15.Wainwright NW, Surtees PG, Welch AA, Luben RN, Khawk, Bingham SA. Healthy lifestyle choices: could sense of coherence aid health promotion? J Epidemiol Community Health. 2007;61:871–6. doi: 10.1136/jech.2006.056275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lindmark U, Stegmay B, Nilsson B, Lindahl B, Johansson I. Food selection associated with sense of coherence in adults. Nutr J. 2005;4:9. doi: 10.1186/1475-2891-4-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eriksson M, Lindstrom B, Lilja J. A sense of coherence and health.Salutogeneis in a societal context: Aland, a special case? J Epidemiol Community Health. 2007;61:684–8. doi: 10.1136/jech.2006.047498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kouvonen AM, Vaananen A, Vahtera J, Heponiemi T, Koskinen A, Cox SJ, et al. Sense of coherence and psychiatric morbidity: a 19-year register-based prospective study. J Epidemiol Community Health. 2010;64:255–61. doi: 10.1136/jech.2008.083352. [DOI] [PubMed] [Google Scholar]
- 19.Nakamura H, Matsuzaki I, Sasahara S, Hatta K, Nagase H, Oshita Y, et al. Enhancement of a sense of coherence and natural killer cell activity which occurred in subjects who improved their exercise habits through health education in the workplace. J Occup Health. 2003;45:278–85. doi: 10.1539/joh.45.278. [DOI] [PubMed] [Google Scholar]
- 20.Nyamathi AM. Relationship of resources to emotional distress, somatic complaints, and high-risk behaviors in drug recovery and homeless minority women. Res Nurs Health. 1991;14:269–77. doi: 10.1002/nur.4770140405. [DOI] [PubMed] [Google Scholar]
- 21.Abrahamsson A, Ejlertsson G. A salutogenic perspective could be of practical relevance for the prevention of smoking amongst pregnant women. Midwifery. 2002;18:323–31. doi: 10.1054/midw.2002.0325. [DOI] [PubMed] [Google Scholar]
- 22.Luszczynska A. Sense of coherence and smoking in a sample of abused women. Psychol Rep. 2002;90:1123–8. doi: 10.2466/pr0.2002.90.3c.1123. [DOI] [PubMed] [Google Scholar]
- 23.Lundqvist T. Chronic cannabis use and the sense of coherence. Life Sci. 1995;56:2145–50. doi: 10.1016/0024-3205(95)00201-g. [DOI] [PubMed] [Google Scholar]
- 24.Ogawa Y, Nakamura H, Nagase H, Ogino K, Ooshita Y, Tsukahara S. Structural analysis for psychosocial factors including health locus of control (HLC) and sense of coherence (SOC) associated with lifestyle-related diseases. Nihon Eiseigaku Zasshi. 2001;55:597–606. doi: 10.1265/jjh.55.597. [DOI] [PubMed] [Google Scholar]
- 25.Kivimäki M, Vahtera J, Elovainio M, Lillrank B, Kevin MV. Death or illness of a family member, violence, interpersonal conflict, and financial difficulties as predictors of sickness absence: longitudinal cohort study on psychological and behavioral links. Psychosom Med. 2002;64:817–25. [PubMed] [Google Scholar]
- 26.Poppius E, Virkkunen H, Hakama M, Tenkanen L. The sense of coherence and risk of injuries: role of alcohol consumption and occupation. J Epidemiol Community Health. 2008;62:35–41. doi: 10.1136/jech.2006.057232. [DOI] [PubMed] [Google Scholar]
- 27.Lee RL, Loke AJ. Health-promoting behaviors and psychosocial well-being of University students in Hong Kong. Public Health Nurs. 2005;22:209–20. doi: 10.1111/j.0737-1209.2005.220304.x. [DOI] [PubMed] [Google Scholar]
- 28.Adams MH, Bowdenia G, Humphrey DS, McAdam LB. Social support and health promotion lifestyles of rural women. Online J Rural Nurs Health Care. 2000;1:28–40. [Google Scholar]
- 29.Wang HH. A comparison of two models of health-promoting lifestyle in rural elderly Taiwanese women. Public Health Nurs. 2001;18:204–11. doi: 10.1046/j.1525-1446.2001.00204.x. [DOI] [PubMed] [Google Scholar]
- 30. [accessed on October 6, 2010]. www.helium.com .
- 31. [accessed on October 6, 2010]. http://yogaforsoul.wordpress.com .
- 32. [accessed on October 6, 2010]. http://religions.pewforum.org/reports .
- 33. [accessed on October 6, 2010]. Available from: www.americanreligionsurvey-aris.org .
- 34.Nilsson KW, Leppert H, Simonsson B, Starrin B. Sense of coherence and psychological well-being: improvement with age. J Epidemiol Community Health. 2010;64:347–52. doi: 10.1136/jech.2008.081174. [DOI] [PubMed] [Google Scholar]