

Abstract
Background:
Health care problems faced by migrant construction workers are always neglected. Fifteen patients were admitted with the complaints of loose motion and pain in the abdomen from a labor settlement at a construction site near our city. Three stool samples revealed darting motility.
Objectives:
To find out more number of cases, the source of infection and to recommend necessary actions to control the outbreak.
Study Design:
A cross-sectional epidemiological study.
Materials and Methods:
Pre-tested, pre-designed epidemiological case sheet was used. Sanitary survey and assessment of ecological correlation was also done. Stool samples of all the admitted patients and seven water samples from the site were collected for laboratory analysis.
Results:
Out of 99 inhabitants, 69 were suffering from the same complaints. Male sufferers were more in number. The age groups affected prominently were 1–4 years and 15–44 years. Peculiar epidemic curve with one peak was noted down. There was a history of heavy rains 2 days before the complaints had started. The construction site was situated on the plateau. The source of the water – dug well – was situated on a slope. The water from the site while moving along the slope was getting mixed into the well. Considering the person, time, place distribution and the peculiar symptoms, presumptive diagnosis of outbreak (point source) of acute gastroenteritis was made. The well water was thought to be the source of infection. Three stool samples and three water samples including the sample from drinking well water grew Vibrio cholerae O1. These results support an earlier hypothesis. The timely interventions were done.
Conclusion:
The impending outbreak can be brought under control with the rapid and simple field epidemiological investigation (shoe leather epidemiology).
Keywords: Construction workers, Diarrhea, Disease outbreak, Shoe leather epidemiology, Vibrio cholerae O1
INTRODUCTION
Modernization and industrialization have led to a boom in the construction industry. The construction sector has got a boost in the developing countries like India. There are more than 20 million construction workers in India at present. Delhi alone has around 600,000.
Health care problems faced by migrant construction workers are similar to those of other disadvantaged populations. Poverty, mobility, compromised living and difficult working conditions, and also, cultural isolation put them at a higher risk for illness. In migrant construction workers, it is found that common diseases occur more frequently. Moreover, often these are severe because they are allowed to progress to advanced stages before accessing care. Diarrheal diseases are one of the major illnesses faced by these people. Contaminated drinking water continues to be the source for most diarrheal outbreaks recorded in India.[1,2]
Quick actions taken with simple and rapid field epidemiological (shoe leather epidemiology) and laboratory investigations together can curb such an outbreak before it progresses into an epidemic/larger outbreak leading to higher morbidity/mortality.
MATERIALS AND METHODS
On 16 September 2009, 15 patients (9 adult males and 6 adult females) from a labor settlement located at a construction site, 5 km away from the city, were admitted in the infectious disease ward of our tertiary care hospital with similar complaints of pain in the abdomen and loose motions with dehydration. They were given IV fluids and other supportive treatment. Nature of the stool was watery with mucus flakes. Two stool samples of each admitted patient, one for microscopy (darting motility)[3] and other one in alkaline peptone water for culture, were taken. Hanging drop preparation of three stool samples revealed darting motility. A team of Public Health Specialist and Microbiologist was constituted. On 17 September, the epidemiological investigation team visited the labor settlement at the construction site to find out more number of cases and the cause of this outbreak. We also intended to recommend necessary action to control the outbreak and measures to prevent such outbreaks in future .
The investigation was carried out as a cross-sectional epidemiological study (shoe leather epidemiology).
Study area and population
A settlement of laborers was located at a construction site, 5 km away from the city. It comprised 40 families and had a population of about 200 individuals. We interviewed 25 families, covering a population of 99. Other houses were closed. This was a migratory population.
Data collection
A clinical case definition was used. A case of acute diarrheal disease was defined as patient presenting with acute watery diarrhea during this period . The team members had with them a structured pre-tested epidemiological case sheet. Clinical history of loose motions during the previous week was recorded along with data pertaining to age, sex, occupation, source of water supply, eating places visited, eating habits, and disposal of excreta and solid wastes. Contribution by ecological factors was also assessed.
Sanitary survey was carried out and environmental data were collected. Five water samples – two from bore wells, one from water stream and two from dug wells (A and B) – were collected from the construction site as shown in Figure 1. For each sample, 90 ml of water was taken in a bottle containing 10 ml of 10-fold concentrated alkaline peptone water (pH 9.2).[3] In addition, two more water samples were collected from dug wells (A and B) in sterilized bottles without any media. These samples were sent to Department of Microbiology for further processing within 2 hours of collection.
Figure 1.
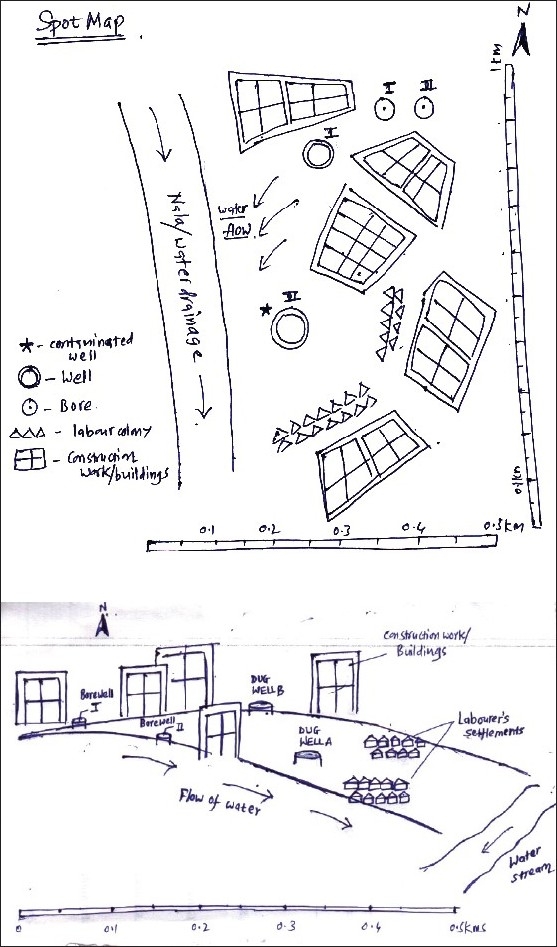
Spot map of the construction site
Statistical analysis
Data were entered and analyzed in Microsoft Excel.
RESULTS
Sanitary survey
The construction was spread over 1 km2 area. The surrounding area was barren except scanty bushy vegetation. There were no farms and any industry in the vicinity. All the houses were kuccha houses (shacks). Shades were provided as bathrooms. Sullage was disposed in an open space around the houses. Open air defecation was the only practice.
On inspection, the construction site had two bore wells and two dug wells. Dug wells were labeled as A and B. Out of these two dug wells, well A was the only source of drinking water and was near the settlement. It was not a sanitary well. The diameter of the well was 25 ft. It was filled up to the brim with water. The depth of the well was 15 ft. Water was turbid with lots of suspended particulate matter. The dimensions of the dug well B were similar to those of dug well A and it was also full of water. These wells were never chlorinated. Construction site was situated on the plateau. Well supplying the drinking water was on the slope, and at the lowermost part of the slope was a flowing water stream which fed on water coming from the construction site, slope and surrounding area. The water from the construction site, while draining into the water stream, was contaminating the drinking water well. Water of both the bore wells and the dug well B was used solely for construction work.
Findings of epidemiological case sheet
All of the males and majority of females except minors were working as laborers. Their earning was meager daily wages.
Clinical history
Of the total 99, 69 were having similar complaints of loose motions and pain in abdomen. 10% of them had complaints of nausea and vomiting also. Every family had at least one member suffering from similar complaints.
Person distribution
This is discussed in Table 1.
Table 1.
Age and sex distribution of the population in the settlement and of cases with diarrheal disease, with age-specific attack rates
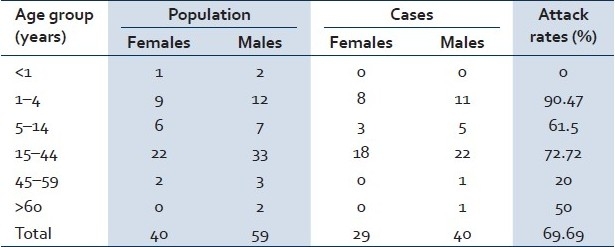
Out of total 69 cases, 40 (57.9%) were males. Overall age-specific rate was 69.69%. Age-specific attack rate was 72.72% in the age group of 15–44 years. It was the highest, i.e. 90.47%, in the age group of 1–4 years. No one in the age group less than 1 year was having any complaint.
Ecological correlation: There was a history of heavy rains 6 days back, i.e. on 9th and 10th of September. Two days after these heavy rains, the complaints started.
There was no history suggestive of food poisoning, e.g. large gathering or any other recent function. No history of recent travel and consumption of food outside was given by any of the patients.
Considering the following, we arrived at a probable diagnosis of an outbreak of acute gastrointestinal infection, eliminating the other possible causes like food poisoning for such an outbreak.
-
a)
Presentation of patients with particular signs and symptoms, darting motility in stool samples on investigations, prominently affected age groups and sex.
-
b)
History of heavy rains leading to contamination of drinking water source in large dose because of its peculiar location on the slope.
-
c)
Start of the complaints after 2 days of the rain with the peculiar epidemic curve with one peak.
We thought of the well water (dug well A) as the possible source of infection.
Laboratory analysis
Out of the 15 stool samples, stool samples of three patients had presence of darting motility. All three grew Vibrio cholerae O1 biotype El Tor, serotype Ogawa. The strains were sensitive to Tetracycline (30 μg), Erythromycin (15 μg), Polymyxin B (50 units), and Norfloxacin (10 μg) and resistant to Cotrimaxazole (25 μg). Out of five water samples (taken in alkaline peptone water), two from the dug wells A and B and one from the water stream showed similar results on the next day. Other two water samples without any media from the dug wells revealed that presumptive coliform counts of both the dug wells were more than the acceptable level.
Isolates were sent to the National Institute of Cholera and Enteric Diseases (NICED), Kolkata. Findings were confirmed.
The laboratory findings later supported our earlier epidemiological hypothesis of an acute outbreak (point source) of gastroenteritis and source of the infection being well water.
Containment measures
Rapid survey of the site was done immediately.
Those who were suffering were treated at the site.
The findings of the survey were immediately conveyed to the local health department.
Drinking of the water from the suspected well was stopped immediately.
Alternate source of potable safe water was made available by local authority after our survey report.
Laborers were asked to drink the water after proper boiling.
Laborers were educated regarding the personal hygiene, sanitary habits.
Deep trench latrines were built for the laborers.
DISCUSSION
The construction work is growing at a rapid pace in the urban parts of developing countries like India. It has come up with its own problems including health problems of the construction workers. More than 150 years after John Snow removed the pump handle in London and used the term “shoe leather epidemiology” for the investigation of Cholera outbreak, outbreaks of cholera continue to be reported worldwide. According to National Health Profile 2008, 11,231,039 cases of acute diarrhea were recorded that year in India, with only 2680 cases of cholera and only one death due to cholera.[4]
In the present outbreak, bacteriological examination of stool and water sample revealed V. cholerae O1, biotype El Tor, serotype Ogawa as the causative organism. Other studies in India[5–8] also revealed the same strain as the causative organism of gastroenteritis outbreaks in the recent past in India.
In the present study, male sufferers were more in number, i.e. 57.9%, because more males compared to females were working at the site. Drinking of water by males was more frequent during work. Age-specific attack rate was 72.72% in the most active age group, i.e. 15–44 years. It was the highest in the age group of 1–4 years which is always the vulnerable group. Similar observations were made by Singh et al. in their study.[9]
In the present study, no one in the age group less than 1 year was having any complaint. The reason for their healthy status could be the fact that infants were mainly fed on breast milk and were drinking less water.
Availability of safe and potable drinking water at the construction site has always been a major problem because of the temporary settlements. Open air defecation and disposal of sullage in an open space, though hazardous, are commonly practiced at such temporary settlements. As these laborers are illiterates/less educated and from lower socioeconomic strata, they also have poor awareness regarding personal hygiene. So, agent, host and environmental factors already coexist. Thus, platform for an outbreak is always set at such sites. This particular balance can get easily disturbed by the natural events like heavy rainfall which may lead to the contamination of drinking water in high dose.[10] Similar scenario was present at the construction site in our study. There was a history of heavy rains 6 days back. Two days after these heavy rains, the complaints started. The epidemic curve of an outbreak showed peak on the 4th day [Figure 2]. Different distributions of incubation periods in differently susceptible individuals and the bacterial dose can be the reason for this kind of an epidemic curve.
Figure 2.
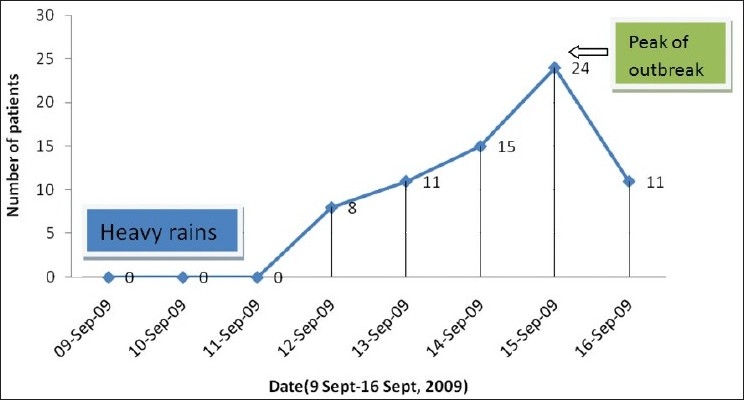
Epidemic curve of an outbreak of acute diarrheal disease
Results of water sampling depicted that the cases had contracted the disease from the contaminated water of a dug well. Further spread of the disease was controlled by active detection of diarrhea cases by house to house survey, prompt treatment of the cases, providing them with ORS packets, health education of people, water sampling of the other water sources, building deep trench latrines and recommending to local health authorities for chlorination of water and closing the contaminated well.
In a developing country like India, with limited resources, a technique/method called as shoe leather epidemiology (field epidemiology), though unfortunately not being implemented nowadays, would definitely help us in controlling an impending epidemic even today. A proper surveillance system for early identification of cases along with continuing health education will help in initiating and implementing prompt control measures. Greater political and financial commitment is needed to look into the health of these migrant workers.
CONCLUSIONS
An investigation was carried out at a labor settlement situated at a construction site, 5 km away from the city, in September 2009 following admission of 15 patients with the complaints suggestive of gastrointestinal infection. A simple and rapid epidemiological investigation was conducted. Out of the 15 stool samples, stool culture of three patients grew the V. cholerae O1, biotype El Tor, serotype Ogawa. Out of five water samples, two from the well and one from the water stream showed similar results on the next day. These laboratory findings later supported our earlier epidemiological hypothesis of an acute outbreak (point source) of gastroenteritis and the source of infection being well water. The outbreak was brought under control by our timely intervention.
A simple and rapid epidemiological investigation can control an impending epidemic, if done vigilantly.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Chakraborty S, Ray K, Misra BS, Ghosh TK. An outbreak of cholera in Indore City, Madhya Pradesh. Some epidemiological observations. J Commun Dis. 1980;13:152–9. [PubMed] [Google Scholar]
- 2.Baveja CP, Chattopadhya D, Kumari S, Dutta KK, Sehgal S. Bacteriological study of drinking water during epidemic of cholera in Delhi. J Commun Dis. 1989;21:59–61. [PubMed] [Google Scholar]
- 3.Ananthanarayan R, Panikar CKJ. Vibrio. In: Ananthanarayan R., editor. Ananthanarayan Panikar's Textbook of Microbiology. 8th ed. Hydrabad: Universities Press; 2009. pp. 303–14. [Google Scholar]
- 4.Central Bureau of Health Intelligence. Ministry of Health and Family Welfare. New Delhi: Government of India; [Last cited on 2010, Dec 5]. National health profile 2008. Available from: www.cbhidghs.nic.in . [Google Scholar]
- 5.Bara D, Dhariwal AC, Jain DC, Sachdeva V, Vohra JG, Prakash RM, et al. Vibrio cholerae 01 outbreak in remote villages of Shimla district, Himachal Pradesh, 1994. J commun Dis. 1997;29:121–5. [PubMed] [Google Scholar]
- 6.Khera AK, Jain DC, Datta KK. Profile of epidemic emergencies in India during 1991 - 1995. J commun dis. 1996;28:129–38. [PubMed] [Google Scholar]
- 7.Ghosh S, Sircar BL. Investigation of an outbreak of acute diarrhoeal disease in Malda district of West Bengal. National Institute of Cholera and Enteric disease (NICED),Kolkata Annual Report. 2003-2004 [Google Scholar]
- 8.Radhakutty G, Sircar BK, Mondal SK, Mukhopadhyay AK, Mitra RK, Basu A, et al. Department of Microbiology, T.D. Medical College, Alleppey Investigation of cholera outbreak in Alleppey and Palghat district, South India. Indian J Med Res. 1997;106:455–7. [PubMed] [Google Scholar]
- 9.Singh MM, Gupta SS, Thakur JS, Kumar R, Ray P, Jain S, et al. Cholera in a periurban slum colony near Chandigarh. Bull PGI. 1998;32:59–62. [Google Scholar]
- 10.Sur D, Dutta P, Nair GB, Bhattacharya SK. National Institute of Cholera and Enteric Diseases (ICMR), Calcutta. Severe Cholera outbreak following floods in northern districts of West Bengal. Indian J Med Res. 2000;112:178–82. [PubMed] [Google Scholar]