

Abstract
Hair casts or pseudonits are thin, elongated, cylindrical concretions that encircle the hair shaft and can be easily dislodged. A case of pseudonits in a 9-year-old girl is reported. Though not unusual, false diagnoses are common.
Keywords: Hair casts, hair diseases, pseudonits, scalp dermatitis
INTRODUCTION
Hair casts or pseudonits are 2-7 mm long, discrete, firm, shiny, white, freely movable tubular accretions that encircle the hair shafts of the scalp.[1] Even though they are not unusual, there is scarce literature on them and underdiagnosis is common. They often occur in great numbers and must be correctly differentiated from pediculosis capitis. Hair casts are indeed common in psoriasis, pityriasis amiantacea, pityriasis capitis and seborrheic dermatitis.[2] False diagnoses are common, which implies inadequate treatment and becomes a reason for both patient and physician anxiety.[3] The objective of this article is to present a case of hair casts in a child mistreated previously and to discuss this relatively rare condition of the scalp.
CASE REPORT
A 9-year-old girl presented to consultation with asymptomatic small whitish lesions resembling nits, attached to the hair shaft. Nit like formations on the scalp had been noticed since the girl was 2 years old. Other family members were not affected by similar disorder. She was referred from a pediatric clinic with a diagnosis of pediculus capitis and had been treated with ketoconazole and scabicide shampoo, without any improvement. The dermatological examination showed white cylinders, easily deployable, located distal, medial and proximal to the hairs, especially on the occipital and parietal regions, bilaterally [Figure 1]. Mycological culture of hair casts and scalp were performed and both were negative. Capillaroscopy revealed a cylindrical and hyaline mass involving the hair shaft [Figure 2].
Figure 1.

White cylinders, easily deployable, located distal, medial and proximal to the hairs
Figure 2.
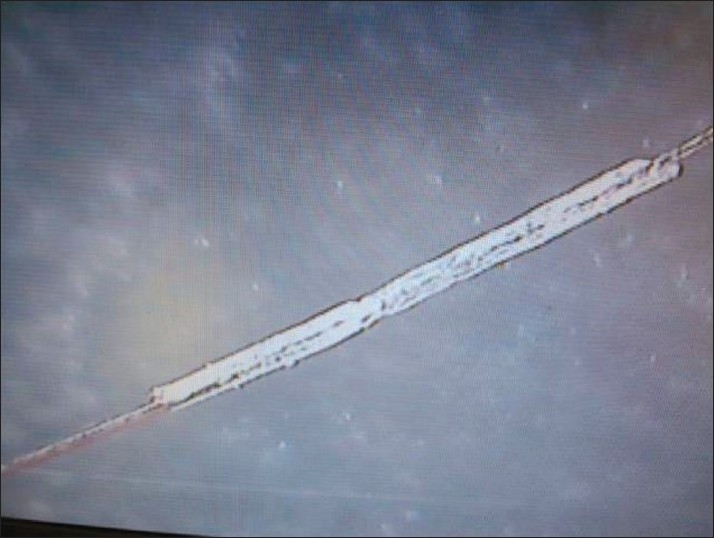
Capillaroscopy – Cylindrical and hyaline mass involving the hair shaft
DISCUSSION
Despite the small number of cases reported in literature, hair casts do not seem to be rare. Apparently, they are more common in females, particularly in patients who subject their hair to excessive traction for a long period.[4]
Casts seem to be most common among young adults.[4] The pathogenesis is often not clear, but their presence can be associated with pityriasis amiantacea, seborrheic dermatitis, hair nodes, scalp psoriasis, hairstyles with much traction and also the use of hair sprays. All these conditions lead to formation of more consistent root sheaths, which do not disintegrate during the hair growth.[5] However, they can occur without any previous abnormality.
Electron microscopy studies showed that the true peripillous hair casts are usually compounds of the outer root sheath and are rarely composed of the internal root sheath, and often some are made up of both the sheaths, internal and external.[6]
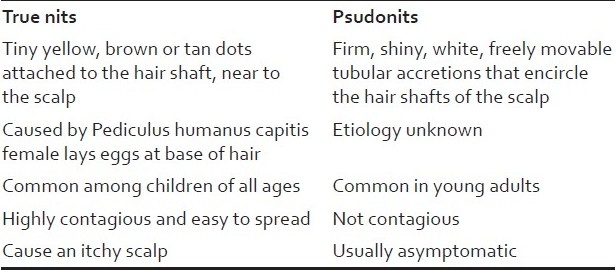
They can be easily slid along the hair shaft.[7,8] This characteristic is of paramount importance in their diagnosis and helps in differentiating them from other scalp disorders, such as pediculosis capitis, piedra, trichomycosis, trichonodosis and trichorrhexis nodosa.[9–11] As is often the case, hair casts may initially be misdiagnosed as the nits of pediculosis capitis [Table 1].
Table 1.
Comparison of true nits and pseudonits
Even though they are benign and have low-morbidity conditions, the fact that they are barely known leads to frequent diagnostic confusion, which may generate unnecessary costs and anxiety for both patients and physicians.[3,4,9,12]
Treatment with keratolitic or coaltar shampoos is ineffective. The best result is obtained with a solution of 0.025% retinoic acid combined with manual removal of the cylinders with comb, but the condition can recur after stopping medication.[8,13–15] A review conducted by the authors found a notable decrease in the number of articles addressing hair casts in the last two decades and new generations of dermatologists have not incorporated it into their list of diagnosis for diseases of the scalp.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Held JL, Bernstein RM. Hair casts or pseudonits acquired following psychological trauma. Cutis. 1989;43:380–1. [PubMed] [Google Scholar]
- 2.Dawber RP. Hair casts. Br J Dermatol. 1979;100:417–21. doi: 10.1111/j.1365-2133.1979.tb01642.x. [DOI] [PubMed] [Google Scholar]
- 3.Minelli L, Gon AS, Sales NCMM. Casts: three cases report and literature review. An Bras Dermatol. 2006;81:159–62. [Google Scholar]
- 4.Zhang W. Epidemiological and etiological studies on hair casts. Clin Exp Dermatol. 1995;20:202–7. doi: 10.1111/j.1365-2230.1995.tb01302.x. [DOI] [PubMed] [Google Scholar]
- 5.Dawber R, Van ND. Doenças dos cabelos e do couro cabeludo: Sinais comuns de apresentação, diagnóstico diferencial e tratamento. São Paulo: Ed Manole; 1996. pp. 205–7. [Google Scholar]
- 6.Taïeb A, Surlève-Bazeille JE, Maleville J. Hair casts: A clinical and morphological study. Arch Dermatol. 1985;121:l009–13. [PubMed] [Google Scholar]
- 7.Kligman AM. Hair casts; parakeratotic comedones of the scalp. AMA Arch Derm. 1957;75:509–11. doi: 10.1001/archderm.1957.01550160035004. [DOI] [PubMed] [Google Scholar]
- 8.Kohn SR. Hair casts or psuedonits. JAMA. 1977;238:2058–9. [PubMed] [Google Scholar]
- 9.Thappa DM, Kumar V, Sharma RC, Lal S. Hair casts. Indian J Dermatol Venereol Leprol. 1993;59:201–2. [Google Scholar]
- 10.Keipert JA. Hair Casts: Review and suggestion regarding nomenclature. Arch Dermatol. 1986;122:927–930. doi: 10.1001/archderm.122.8.927. [DOI] [PubMed] [Google Scholar]
- 11.Herman PS. Peripilar casts. Arch Dermatol Forsch. 1974;248:321–7. doi: 10.1007/BF00595550. [DOI] [PubMed] [Google Scholar]
- 12.Scott MJ, Jr, Roenigk HH., Jr Hair casts classification, staining characteristics and differential diagnosis. J Am Acad Dermatol. 1983;8:27–32. doi: 10.1016/s0190-9622(83)70003-4. [DOI] [PubMed] [Google Scholar]
- 13.Fabbri P, Difonozo EM, Palleschi GM, Pacini P. Hair casts. Int J Dermatol. 1988;27:319–21. doi: 10.1111/j.1365-4362.1988.tb02361.x. [DOI] [PubMed] [Google Scholar]
- 14.Zhu WY, Xia MY, Wu JH, Do DA. Hair casts: A clinical and electron microscopic study. Pediatr Dermatol. 1990;7:270–4. doi: 10.1111/j.1525-1470.1990.tb01023.x. [DOI] [PubMed] [Google Scholar]
- 15.Keipert JA. Peripilar keratin casts in boys. Med J Aust. 1975;16(2):275. [PubMed] [Google Scholar]