

Abstract
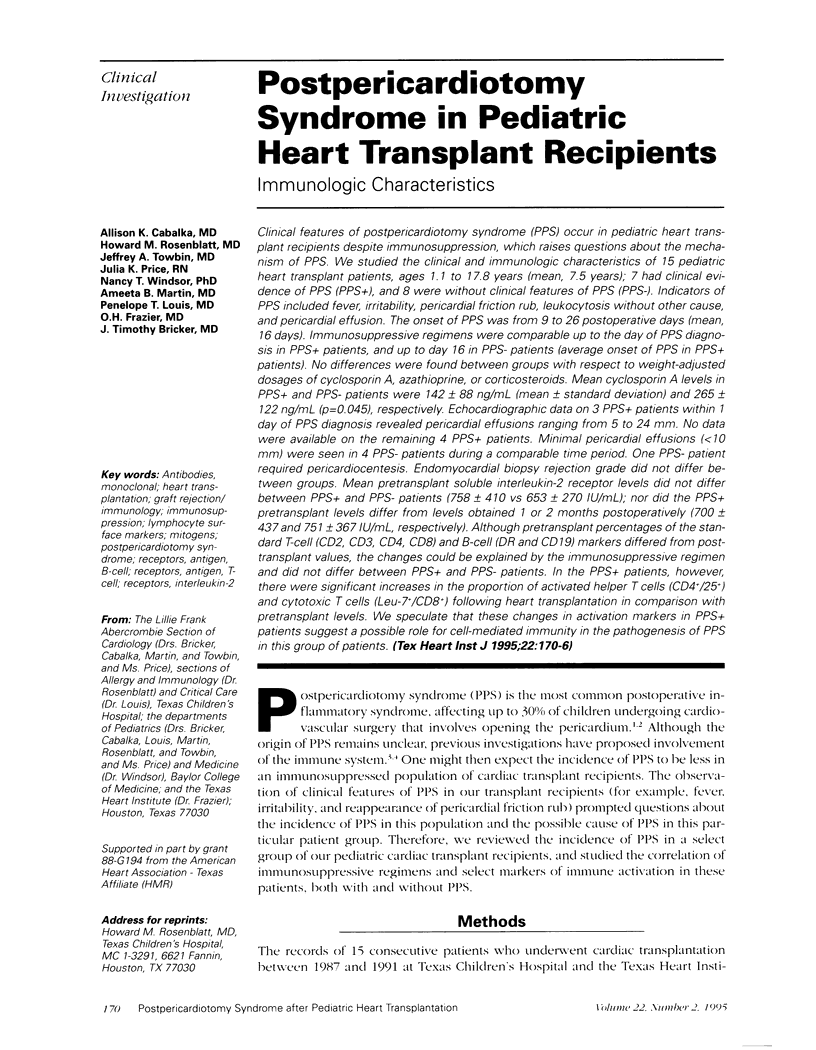
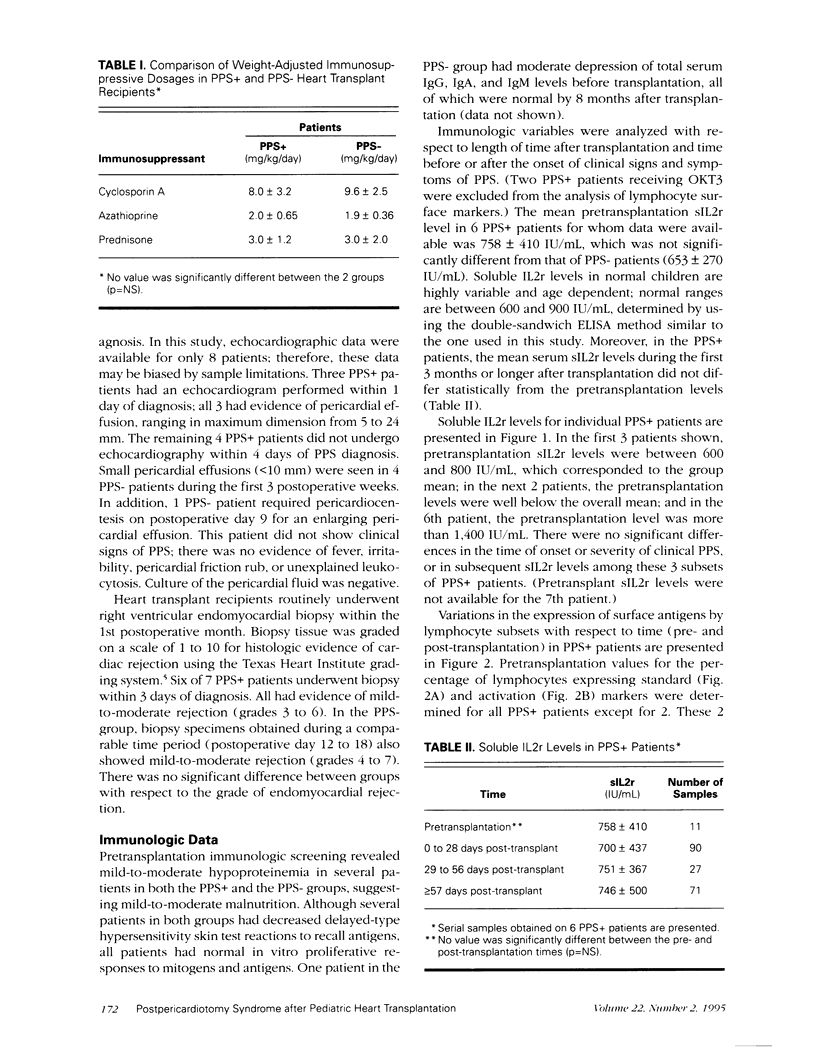
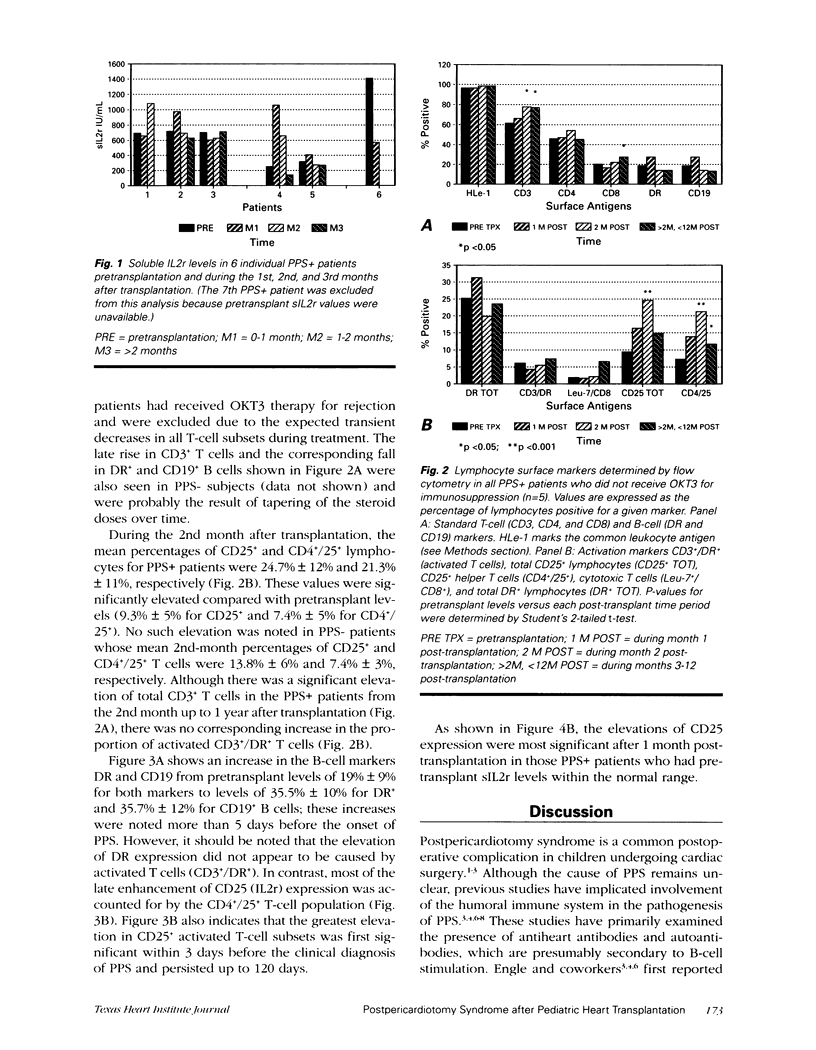
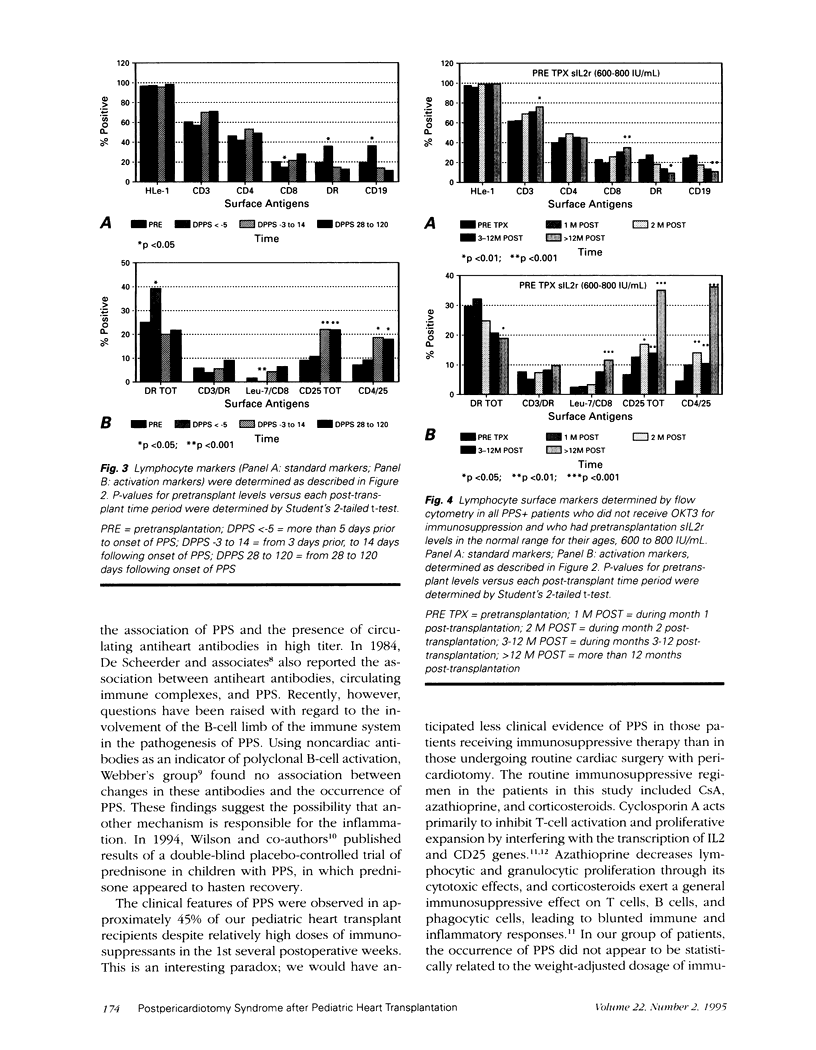
Clinical features of postpericardiotomy syndrome (PPS) occur in pediatric heart transplant recipients despite immunosuppression, which raises questions about the mechanism of PPS. We studied the clinical and immunologic characteristics of 15 pediatric heart transplant patients, ages 1.1 to 17.8 years (mean, 7.5 years); 7 had clinical evidence of PPS (PPS+), and 8 were without clinical features of PPS (PPS-). Indicators of PPS included fever, irritability, pericardial friction rub, leukocytosis without other cause, and pericardial effusion. The onset of PPS was from 9 to 26 postoperative days (mean, 16 days). Immunosuppressive regimens were comparable up to the day of PPS diagnosis in PPS+ patients, and up to day 16 in PPS- patients (average onset of PPS in PPS+ patients). No differences were found between groups with respect to weight-adjusted dosages of cyclosporin A, azathioprine, or corticosteroids. Mean cyclosporin A levels in PPS+ and PPS- patients were 142 +/- 88 ng/mL (mean +/- standard deviation) and 265 +/- 122 ng/mL (p = 0.045), respectively. Echocardiographic data on 3 PPS+ patients within 1 day of PPS diagnosis revealed pericardial effusions ranging from 5 to 24 mm. No data were available on the remaining 4 PPS+ patients. Minimal pericardial effusions (< 10 mm) were seen in 4 PPS- patients during a comparable time period. One PPS- patient required pericardiocentesis. Endomyocardial biopsy rejection grade did not differ between groups. Means pretransplant soluble interleukin-2 receptor levels did not differ between PPS+ and PPS- patients (758 +/- 410 vs 653 +/- 270 IU/mL); nor did the PPS+ pretransplant levels differ from levels obtained 1 or 2 months postoperatively (700 +/- 437 and 751 +/- 367 IU/mL, respectively). Although pretransplant percentages of the standard T-cell (CD2, CD3, CD4, CD8) and B-cell (DR and CD19) markers differed from post-transplant values, the changes could be explained by the immunosuppressive regimen and did not differ between PPS+ and PPS- patients. In the PPS+ patients, however, there were significant increases in the proportion of activated helper T cells (CD4+/25+) and cytotoxic T cells (Leu-7+/CD8+) following heart transplantation in comparison with pretransplant levels. We speculate that these changes in activation marker in PPS+ patients suggest a possible role for cell-mediated immunity in the pathogenesis of PPS in this group of patients.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- DRUSIN L. M., ENGLE M. A., HAGSTROM J. W., SCHWARTZ M. S. THE POSTPERICARDIOTOMY SYNDROME: A SIX-YEAR EPIDEMIOLOGIC STUDY. N Engl J Med. 1965 Mar 25;272:597–602. doi: 10.1056/NEJM196503252721201. [DOI] [PubMed] [Google Scholar]
- De Scheerder I., Wulfrank D., Van Renterghem L., Sabbe L., Robbrecht D., Clement D., Derom F., Plum J., Verdonk G. Association of anti-heart antibodies and circulating immune complexes in the post-pericardiotomy syndrome. Clin Exp Immunol. 1984 Aug;57(2):423–428. [PMC free article] [PubMed] [Google Scholar]
- Engle M. A., McCabe J. C., Ebert P. A., Zabriskie J. The Postpericardiotomy syndrome and antiheart antibodies. Circulation. 1974 Mar;49(3):401–406. doi: 10.1161/01.cir.49.3.401. [DOI] [PubMed] [Google Scholar]
- Engle M. A., Zabriskie J. B., Senterfit L. B., Gay W. A., Jr, O'Loughlin J. E., Jr, Ehlers K. H. Viral illness and the postpericardiotomy syndrome. A prospective study in children. Circulation. 1980 Dec;62(6):1151–1158. doi: 10.1161/01.cir.62.6.1151. [DOI] [PubMed] [Google Scholar]
- Engle M. A., Zabriskie J. B., Senterfit L. B., Tay D. J., Ebert P. A. Immunologic and virologic studies in the postpericardiotomy syndrome. J Pediatr. 1975 Dec;87(6 Pt 2):1103–1108. doi: 10.1016/s0022-3476(75)80122-3. [DOI] [PubMed] [Google Scholar]
- Kahan B. D. Cyclosporine. N Engl J Med. 1989 Dec 21;321(25):1725–1738. doi: 10.1056/NEJM198912213212507. [DOI] [PubMed] [Google Scholar]
- Kopp E., Ghosh S. Inhibition of NF-kappa B by sodium salicylate and aspirin. Science. 1994 Aug 12;265(5174):956–959. doi: 10.1126/science.8052854. [DOI] [PubMed] [Google Scholar]
- Krensky A. M., Weiss A., Crabtree G., Davis M. M., Parham P. T-lymphocyte-antigen interactions in transplant rejection. N Engl J Med. 1990 Feb 22;322(8):510–517. doi: 10.1056/NEJM199002223220805. [DOI] [PubMed] [Google Scholar]
- Maisch B., Berg P. A., Kochsiek K. Clinical significance of immunopathological findings in patients with post-pericardiotomy syndrome. I. Relevance of antibody pattern. Clin Exp Immunol. 1979 Nov;38(2):189–197. [PMC free article] [PubMed] [Google Scholar]
- McAllister H. A., Jr, Schnee M. J., Radovancević B., Frazier O. H. A system for grading cardiac allograft rejection. Tex Heart Inst J. 1986 Mar;13(1):1–3. [PMC free article] [PubMed] [Google Scholar]
- Mestre M., González C., Griño J. M., Valls A., Bonete J., Mané E., Corominas M., Bas J., Romeu A., Buendia E. Sequential monitoring of immunoregulatory T cell subsets in renal transplantation. Transplant Proc. 1992 Feb;24(1):73–75. [PubMed] [Google Scholar]
- Waldmann T. A., Pastan I. H., Gansow O. A., Junghans R. P. The multichain interleukin-2 receptor: a target for immunotherapy. Ann Intern Med. 1992 Jan 15;116(2):148–160. doi: 10.7326/0003-4819-116-2-148. [DOI] [PubMed] [Google Scholar]
- Webber S. A., Wilson N. J., Fung M. Y., Malleson P. N., Petty R. E., Patterson M. W., Sandor G. G. Autoantibody production after cardiopulmonary bypass with special reference to postpericardiotomy syndrome. J Pediatr. 1992 Nov;121(5 Pt 1):744–747. doi: 10.1016/s0022-3476(05)81907-9. [DOI] [PubMed] [Google Scholar]
- Wilson N. J., Webber S. A., Patterson M. W., Sandor G. G., Tipple M., LeBlanc J. Double-blind placebo-controlled trial of corticosteroids in children with postpericardiotomy syndrome. Pediatr Cardiol. 1994 Mar-Apr;15(2):62–65. doi: 10.1007/BF00817608. [DOI] [PubMed] [Google Scholar]
- Young J. B., Lloyd K. S., Windsor N. T., Cocanougher B., Weilbaecher D. G., Kleiman N. S., Smart F. W., Nelson D. L., Lawrence E. C. Elevated soluble interleukin-2 receptor levels early after heart transplantation and long-term survival and development of coronary arteriopathy. J Heart Lung Transplant. 1991 Mar-Apr;10(2):243–250. [PubMed] [Google Scholar]
- Young J. B., Windsor N. T., Smart F. W., Kleiman N. S., Weilbaecher D. G., Noon G. P., Nelson D. L., Lawrence E. C. Inability of isolated soluble interleukin-2 receptor levels to predict biopsy rejection scores after heart transplantation. Transplantation. 1991 Mar;51(3):636–641. doi: 10.1097/00007890-199103000-00018. [DOI] [PubMed] [Google Scholar]