

Abstract
Congenital disorders, cancer, trauma, or other conditions of the genitourinary tract can lead to significant organ damage or loss of function, necessitating eventual reconstruction or replacement of the damaged structures. However, current reconstructive techniques are limited by issues of tissue availability and compatibility. Physicians and scientists have begun to explore tissue engineering and regenerative medicine strategies for repair and reconstruction of the genitourinary tract. Tissue engineering allows the development of biological substitutes which could potentially restore normal function. Tissue engineering efforts designed to treat or replace most organs are currently being undertaken. Most of these efforts have occurred within the past decade. However, before these engineering techniques can be applied to humans, further studies are needed to ensure the safety and efficacy of these new materials. Recent progress suggests that engineered urologic tissues and cell therapy may soon have clinical applicability.
Keywords: tissue engineering, regenerative medicine, genitourinary tract, extracellular matrix (ECM), scaffold, penis
1. INTRODUCTION
Congenital disorders, cancer, trauma, or other conditions of the genitourinary tract can lead to significant organ damage or loss of function, necessitating eventual reconstruction or replacement of the damaged structures. However, current reconstructive techniques are limited by issues of tissue availability and compatibility. These techniques use nonurologic host tissues (skin, gastrointestinal segments, or mucosa from multiple body sites), donor tissues (cadaver fascia or cadaver or living donor kidney), heterologous tissues (bovine collagen), or artificial materials (silicone, polyurethane, or polytetrafluoroethylene) to reconstruct damaged organs. However, all of these materials can lead to significant complications resulting from immunologic rejection or functional mismatches between the native and implanted tissues.
In order to reduce or eliminate these complications, physicians and scientists have begun to explore tissue engineering and regenerative medicine strategies for repair and reconstruction of the genitourinary tract. Tissue engineering allows the development of biological substitutes which could potentially restore normal function. This may involve the use of synthetic or natural matrices termed scaffolds. When used alone, some scaffolds can facilitate the body's natural ability to regenerate by directing new tissue growth. Alternatively, scaffolds can be seeded with cells, and the resulting construct can be implanted into the patient in order to restore the structure and function of damaged tissues and organs. In recent years, novel methods of cell culture have been developed, and these methods allow autologous cells to be grown ex vivo from a small sample of a patient's own tissue. These cells can then be combined with an appropriate scaffold material. This process may be able to generate the large amounts of tissue required for genitourinary reconstruction without the donor site morbidity associated with grafting procedures. In addition, the engineered tissue would be biocompatible, and the risk of rejection would be eliminated.
In this paper, we will discuss various methods of generating engineered tissue. We will then focus on development of tissue-engineering approaches that are designed specifically to repair male genital tissue and restore normal appearance and function.
2. FUNDAMENTALS OF TISSUE ENGINEERING
2.1. Biomaterials
For cell-based tissue engineering, cells are generally seeded onto a synthesized scaffold. Biomaterials are used to replicate the biologic and mechanical function of the native extracellular matrix (ECM) found in tissues in the body by serving as an artificial ECM. Biomaterials can provide a three-dimensional space for the cells to form into new tissues with appropriate structure and function and also can allow for the delivery of cells and appropriate bioactive factors (e.g., cell adhesion peptides and growth factors) to desired sites in the body [1]. As the majority of mammalian cell types are anchorage dependent and will die if no cell-adhesion substrate is available, biomaterials provide a cell-adhesion substrate that can deliver cells to specific sites in the body. Furthermore, bioactive signals, such as cell-adhesion peptides and growth factors, can be loaded along with cells to help regulate cellular function.
Generally, three classes of biomaterials have been used for engineering tissues and organs: naturally derived materials, such as collagen, acellular tissue matrices, such as bladder submucosa and small-intestinal submucosa (SIS), and synthetic polymers, such as polyglycolic acid (PGA), polylactic acid (PLA), and poly(lactic-co-glycolic acid) (PLGA). Naturally derived materials and acellular tissue matrices have the potential advantage of biologic recognition, but synthetic polymers can be produced reproducibly on a large scale with controlled properties of strength, degradation rate, and microstructure.
Collagen is the most abundant and ubiquitous structural protein in the body, and it may be readily purified from both animal and human tissues with an enzyme treatment and salt/acid extraction [2]. Collagen has long been known to exhibit minimal inflammatory and antigenic responses [3], and it has been approved by the U.S. Food and Drug Administration for many types of medical applications [4]. This material can be processed into a wide variety of structures such as sponges, fibers, and films [5–7].
Acellular tissue matrices are collagen-rich matrices prepared by removing cellular components from tissues. The matrices are often prepared by mechanical and chemical manipulation of a segment of bladder tissue [8–11]. The matrices slowly degrade after implantation and are replaced and remodeled by ECM proteins synthesized and secreted by transplanted or ingrowing cells. Acellular tissue matrices have been proved to support cell ingrowth and regeneration of genitourinary tissues, including urethra and bladder, with no evidence of immunogenic rejection [11, 12]. Because the structures of the proteins (e.g., collagen and elastin) in acellular matrices are well conserved and normally arranged, the mechanical properties of the acellular matrices are not significantly different from those of native bladder submucosa [8].
Polyesters of naturally occurring α-hydroxy acids, including PGA, PLA, and PLGA, are widely used in regenerative medicine. The degradation products of PGA, PLA, and PLGA are nontoxic, natural metabolites that are eventually eliminated from the body in the form of carbon dioxide and water [13]. Because these polymers are thermoplastics, they can easily be formed into a three-dimensional scaffold with a desired microstructure, gross shape, and dimension by various techniques, including molding, extrusion [14], solvent casting [15], phase separation techniques, and gas-foaming techniques [16]. More recently, techniques such as electrospinning have been used to quickly create highly porous scaffolds in various conformations [17–20]. However, one drawback of the synthetic polymers is lack of biologic recognition.
2.2. Cells
Two main categories of stem cells are used in tissue engineering, pluripotent stem cells, and native progenitor cells. Embryonic stem cells exhibit three unique properties: the ability to proliferate in an undifferentiated but pluripotent state, the ability to differentiate into many specialized cell types, and the ability to form clonal populations [21]. This makes them an attractive resource for regenerative medicine techniques. They can be isolated by aspirating the inner cell mass from the embryo during the blastocyst stage [22]. Human embryonic stem cells have been shown to differentiate into cells from all three embryonic germ layers in vitro. The political controversy surrounding stem cells began in 1998 with the creation of human embryonic stem cells derived from discarded embryos. In addition to the ethical dilemma surrounding the use of embryonic stem cells, their clinical application is also limited, because they represent an allogenic resource and thus have the potential to evoke an immune response.
More recently, reports have been published of the transformation of adult cells isolated from organs or bone marrow into pluripotent stem cells through a type of genetic “reprogramming”. Reprogramming is a technique that involves dedifferentiation of adult somatic cells to produce patient-specific pluripotent stem cells without the use of embryos. Cells generated by reprogramming would be genetically identical to the somatic cells (and thus the patient who donated these cells) and would not be rejected. Mouse embryonic fibroblasts and adult mouse fibroblasts have been reprogrammed into an “induced pluripotent state (iPS)” [23]. When iPS cells were injected into mouse blastocysts, they contributed to a variety of cell types; however, they were not identical to embryonic stem cells, as chimeras made from iPS cells did not result in full-term pregnancies.
An alternate source of stem cells is the amniotic fluid and placenta. Amniotic fluid and the placenta contain multiple partially differentiated cell types derived from the developing fetus. Isolated stem-cell populations from these source have been shown to express embryonic and adult stem-cell markers [24]. The undifferentiated stem cells expand extensively without feeders and double every 36 hours. Unlike human embryonic stem cells, the amniotic fluid stem cells do not form tumors in vivo. Lines maintained for over 250 population doublings retained long telomeres and a normal karyotype. AFS cells are broadly multipotent.
An additional advantage in using native progenitor cells is that they can be obtained from the specific organ to be regenerated, expanded, and used in the same patient without rejection in an autologous manner [10, 25–41]. Bladder, ureter, and renal pelvis cells can equally be harvested, cultured, and expanded in a similar fashion. Normal human bladder epithelial and muscle cells can be efficiently harvested from surgical material, extensively expanded in culture, and their differentiation characteristics, growth requirements, and other biologic properties can be studied [33, 35, 36, 42–51]. Major advances in cell culture techniques have been made within the past decade, and these techniques make the use of autologous cells possible for clinical application.
When native cells are used for tissue reconstitution, donor tissue is dissociated into individual cells, which are either implanted directly into the host or expanded in culture, attached to a support matrix, and reimplanted after expansion. The implanted tissue can be heterologous, allogeneic, or autologous. Ideally, this approach allows lost tissue function to be restored or replaced in toto and with limited complications [31]. Native cells and tissues are usually preferable for reconstruction. In most cases, the replacement of lost or deficient tissues with functionally equivalent cells and tissues would improve the outcome for these patients. This goal may be attainable with the use of regenerative medicine techniques.
3. ENGINEERED PENILE PROSTHESES
Early procedures for penile reconstruction involved the use of rib cartilage as a stiffener; however, this method fell out of favor due to poor functional and cosmetic results [52]. This was followed by the use of extracavernosal acrylic stents, intracavernosal polypropylene rods, and finally silicone prostheses. While current surgical treatment works well, there are significant risks to the implantation of foreign materials into the penis including infection and erosion which may necessitate removal [53].
Of the natural tissues in the human body, cartilage would serve as an ideal material for prosthesis due to its rigidity and biochemical properties. Initial studies performed by Yoo et al. [54] have demonstrated that cartilage rods could be produced by seeding bovine chondrocytes onto polyglycolic acid polymer rods and implanting them into athymic nude mice. Compression, tension, and bending studies performed after harvesting demonstrated that the cartilaginous structures were readily elastic and withstood high degrees of pressure. All constructs showed mature well-formed chondrocytes.
Subsequent studies in rabbits by the same group [55] demonstrated the ability of cartilage rods to function in vivo. Chondrocytes were harvested from rabbit ears and seeded onto biodegradable poly-L-lactic acid coated polyglycolic acid polymer rods. They were then inserted into the corporal spaces of rabbits. Harvested tissues demonstrated that the scaffold had fully degraded within two months, and at six months, mature fully formed chondrocytes were present. There were no instances of infection or erosion of these cartilage prostheses.
4. TISSUE ENGINEERING OF SPECIFIC PENILE STRUCTURES
4.1. Urethra
In men, the urethra is divided into three parts on the basis of anatomical location. The prostatic urethra crosses through the prostate gland, the membranous urethra passes through the external urethral sphincter and is the narrowest part of the urethra, and the membranous or penile urethra runs along the length of the shaft of the penis through the corpus spongiosum. The urethral epithelium is primarily a continuation of the bladder mucosa and is composed of transitional cells. As the urethra approaches the meatus, the mucosa is made up of stratified columnar cells, followed by stratified squamous cells at the meatus itself. There are small periurethral glands which secrete mucus along the length of the urethra which help to protect the urethra from corrosive urine.
Congenital and acquired disorders of the urethra remain a challenge in the urology field. Numerous conditions including strictures, trauma, congenital defects, and cancer can often cause serious issues in voiding requiring additional tissues for reconstruction and repair. Often, there is a lack of native urethral tissue for adequate reconstruction requiring the use of tissue grafts of flaps from other sources [56]. However, the use of grafts and flaps can lead to significant complications, including stenosis, hair growth, and fistula formation [57, 58]. A variety of synthetic materials have also been proposed for use in urethral reconstruction, including silicone, Teflon, and polyvinyl. These materials also have significant complications including erosion, dislodgement, fistula formation, stenosis, and calcification [59, 60]. For these reasons, tissue-engineered biocompatible urethral segments would be a preferred material for urethroplasty [61].
4.1.1. Acellular Scaffolds in Urethral Repair
A number of acellular scaffolds have been used in animal models to facilitate the regeneration of urethral tissue, including polyglycolic acid- and acellular collagen-based scaffolds made from small intestine and bladder [62–66]. Biodegradable scaffolds such as polyglactin fiber mesh coated with polyhydroxybutyric acid have been used to reconstruct urethras in dogs [65]. A four centimeter segment of canine urethra was excised and replaced with this material. At 8–12 weeks after implantation, the acellular mesh had allowed for regeneration of the urothelium, surrounding smooth muscle, and vasculature. Polyglactin fiber mesh with hyaluronan benzyl ester has also been used in a similar fashion in a rabbit model. In this experiment, degradation of the biomaterial was apparent around day three after implantation, and epitheliailzation and collagen remodeling of the surrounding structures were seen within four weeks [67].
Native structures have also been used as scaffolds. Urethral reconstruction with tubularized peritoneum has been attempted in a rabbit model, and this resulted in good epithelialization of the neourethra. However, there was a high rate of fistula formation with two of twelve animals developing fistulas [68]. Initial studies using small bowel submucosa have also shown urethral regeneration supported by vascularization and smooth muscle formation [64]. However, more recent studies of a commercially available small bowel submucosal patch did not show any improvement in regeneration of the urethra versus native healing in a rabbit model of urethral injury [69].
Bladder-derived acellular collagen matrix has proved to be a suitable graft for repair of urethral defects [70]. In a rabbit model, segments of urethra have been resected and replaced with acellular collagen scaffolds in an onlay fashion, and the animals were able to successfully void through the reconstructed urethra [11]. This model has been applied clinically in patients with hypospadias who had undergone previous repair and had a paucity of tissue for repeat reconstruction [71]. Cadaveric bladders were microdissected, and the submucosal layer was isolated, washed, and decellularized. The collagen scaffold was then trimmed to size and applied in an onlay fashion to the urethral plate using 6-0 absorbable sutures. After a mean followup of nearly two years, three of four patients had good function and cosmesis. One patient developed a subglandular fistula.
Similar collagen scaffolds have also been used in urethral stricture disease [72]. Scaffolds were prepared in a similar fashion as above and applied to the urethral plate using 6-0 absorbable sutures. After mean followup of 37 months, 24 of the 28 patients had a successful outcome with no decrease in urethral caliber. The remaining four patients had a slight caliber decrease at the anastomotic sites on urethrography. A subcoronal fistula developed in one patient which closed spontaneously one year after repair. Mean maximum urine flow rate increased from a mean preoperative value of 9 mL/sec to 19.7 mL/sec postoperatively. These studies demonstrate that collagen scaffolds appear to be beneficial for patients with abnormal urethral conditions. In followup with these patients three years later, they continued to do well with no clinical changes from the initial postoperative period [73].
4.1.2. Cell-Seeded Scaffolds in Urethral Repair
Despite the successes in onlay repairs, it has been shown that tubularized urethral repairs with acellular scaffolds are not feasible, as native cells are not able to fully incorporate into the circumferential scaffold for defects greater than 0.5 cm [74]. In these situations, cell seeded collagen scaffolds are preferable [75]. One of the initial limitations to using cell-based therapy for genitourinary applications had been the ability to grow urothelial cells in large quantities. Normal urothelial cells could be harvested and grown but with limited expansion potential. More recently, a number of techniques have been developed which allow for the large-scale expansion of these cells without the need for enzymatic digestion or serum [76–78]. With the development of these techniques, it is now possible to collect autologous urothelial cells from patients, expand them in culture, and return them to the host in quantities necessary for reconstructive procedures.
De Filippo et al. [75] have demonstrated the ability to perform circumferential urethroplasties using cell-seeded scaffolds. Autologous bladder epithelium and smooth muscle from rabbits was harvested and seeded onto tubularized collagen constructs. The entire urethra of male rabbits was excised, and urethroplasty was performed. Nine animals were reconstructed with cell-seeded scaffolds, and six animals were reconstructed with acellular scaffolds. Serial urethrograms were performed showing a wide caliber urethra in all animals implanted with the cell-seeded scaffold, while all animals repaired with the acellular scaffold showed areas of significant narrowing. Histologically, a transitional epithelial layer surrounded by increasingly organized smooth muscle bundles was seen in the cell-seeded scaffold group. However, histology from the acellular scaffold group showed transitional cells surrounded by limited unorganized smooth muscle. The cell-seeded scaffolds produced tissue which is histologically and functionally similar to native urethra.
Biocompatible uretheral stents have also been created using chondrocyte seeded polymer matrices [79]. 10 mm cartilaginous cylinder were developed with an outer diameter of 9 mm from from polyglycolic acid mesh coated with 50 : 50 polylactic-co-glycolic acid and were seeded with bovine chondrocytes and implanted subcutaneously in nude mice. Biomechanical testing demonstrated that the cartilaginous cylinders in each group were readily elastic and withstood high degrees of pressure.
4.2. Corporal Bodies
The anatomy of the penis is complex and composed of three separate cylinders. Two paired cylinders called the corpora cavernosa make up the majority of the penis and are the primary structures involved in erectile function. The corpora cavernosa consist of a network of large venous sinuses separated by dense connective tissue called trabeculae. During erection, blood enters the corpora from the central artery into helicine arteries and finally into the sinuses. These sinuses are later drained by smaller veins emptying into the dorsal vein. The third cylinder is called the corpus spongiosum, and it houses the urethra. Each of the three corpora is covered by a thick fibrous covering called the tunica albuginea. All three of these cylinders are covered by a thick membrane known as Buck's fascia. Finally, Collie's fascia, which is continuous with the abdominal wall, covers the entire structure.
Extensive reconstructive procedures involving the corporal bodies may be needed in patients with congenital malformation, malignancy, or trauma. Due to the shortage of autologous tissues, these surgical procedures are typically staged and often utilize nongenital tissues as a grafting source. These procedures have a high risk of complication due to infection, donor site morbidity, and graft failure [80, 81]. The creation of alternative materials is a major challenge for phallic reconstruction due to the unique anatomical architecture of the corporal bodies.
Although the corporal bodies only contain two primary cell types, smooth muscle, and endothelium, engineering this tissue remains a challenge. Experiments by Kershen et al. [82] looked at the feasibility of using human corporal smooth muscle cells for reconstructive procedures. Human corpus cavernosum smooth muscle cells were harvested during surgical procedures, isolated, and cultured. They were then seeded on polymer scaffolds and implanted subcutaneously into nude mice. Histology demonstrated smooth muscle multilayers as well as ingrowth into the scaffold. Initial studies by Falke et al. were aimed at replacing short segments of the corporal body by using natural collagen scaffolds and autologous cells [83]. This was accomplished by harvesting donor rabbit corpora and decellularizing them. Human corporal smooth muscle and endothelial cells [84, 85] were then seeded in a stepwise fashion, and the constructs were implanted into athymic nude mice. Tissues were harvested at sequential time points after implantation and demonstrated the presence of neovascularity in the sinusoidal spaces with increasing organization of smooth muscle and collagen over time. Organ bath studies demonstrated the ability of these harvested tissues to contract. No response was seen in unseeded control specimens.
This work was recently taken one step further by the same group. They demonstrated the ability to bioengineer entire pendular penile corporal bodies in a rabbit model [86]. Decellularized donor corporal bodies were seeded with autologous smooth muscle and endothelial cells in a stepwise fashion (Figure 1). Rabbits then underwent complete excision of the corporal bodies followed by implantation of seeded scaffolds, unseeded scaffolds, or no construct. The group implanted with seeded scaffolds demonstrated normal intracavernosal pressures within six months of surgery (Figure 2), and 10 out of 12 rabbits were able to successfully mate with female rabbits, defined as a positive vaginal swab for semen or pregnancy. None of the unseeded scaffold group or negative controls was able to have successful intercourse.
Figure 1.
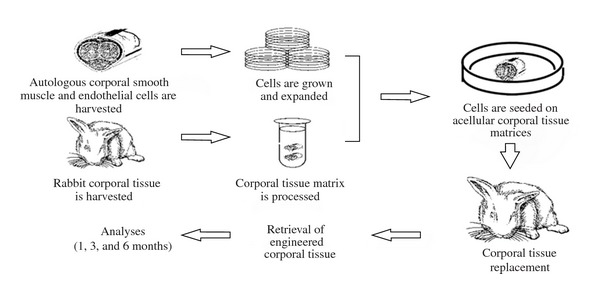
Using tissue engineering techniques to create entire penile corpora.
Figure 2.
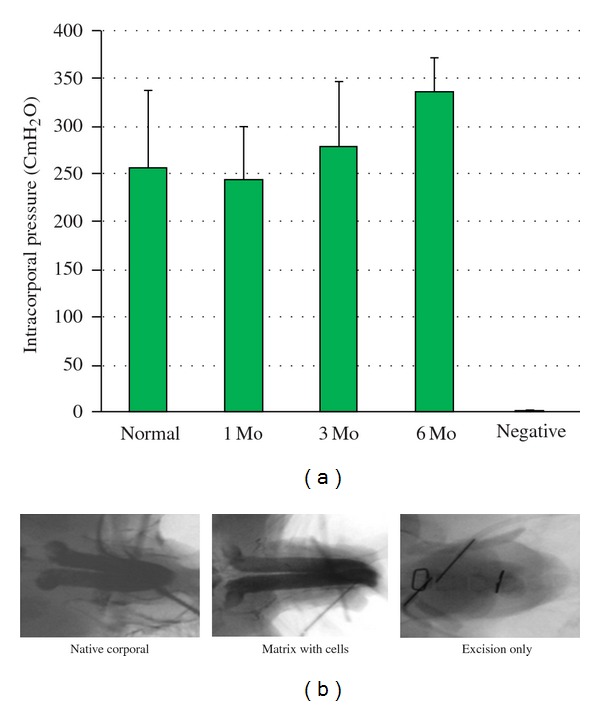
(a) Cavernosometry shows that all rabbits implanted with the bioengineered corpora after complete pendular penile corporal excision had sufficient intracorporal pressure (ICP) to attain erection. The levels of ICP were comparable to native corpora. (b) Cavernosography shows a homogenous appearance of corpora in the bioengineered group, similar to the native corpora, and multiple filling defects in the negative control group.
To improve the cellular content of these bioengineered corporal bodies, corporal cells were seeded dynamically onto acellular corporal tissue matrcies and placed in a mechanical bioreactor for 48 hours. These constructs were then implanted into nude mice. Histology demonstrated that dynamically seeded scaffolds lead to biochemically improved corporal tissues [87].
4.3. Tunica Albuginea
Patients with deformities of the penis, particularly Peyronie's disease, can experience significant pain and functional problems due to plaque formation and curvature of the penis. Currently, diseases such as Peyronie's are treated with plaque excision or incision and grafting of the tunica albuginea with materials such as small intestinal submucosa, fascia, and pericardium [88]. All of these materials have drawbacks, including limited availability, donor site morbidity, and limited effectiveness. The use of a bioengineered tissue would be able to overcome most of the limitations of current techniques while allowing for lasting results.
Schultheiss et al. [89] isolated porcine fibroblasts from open fascia biopsies and seeded them on decellularized collagen matrices. The seeded matrices were then cultivated in a bioreactor under continuous multiaxial stress for 21 days. Static cultures without mechanical stress served as controls. Mechanically strained cultures of fibroblasts showed a homogeneous multilayer matrix infiltration and a regular cell alignment in the direction of strain axis after 7 days as well as increased production of extracellular matrix proteins compared to the static control.
Similar work has been performed using an acellular bladder mucosal graft [90]. Acellular matrices were constructed from pigs' bladders by cell lysis. A segment of the tunica albuginea of nine rabbits was excised, and the defect was covered with porcine bladder acellular matrix. Histology of the resected graft showed collagen fibers with many pores. Two months after implantation, the graft sites exhibited excellent healing without contracture, and the fusion between the graft and the neighboring normal TA appeared to be well established. There were no significant histological differences between the implanted tunica and the normal control tunica at 6 months after implantation.
5. CONCLUSION
Tissue-engineering efforts designed to treat or replace most organs are currently being undertaken. Most of these efforts have occurred within the past decade. However, before these engineering techniques can be applied to humans, further studies are needed to ensure the safety and efficacy of these new materials. Recent progress suggests that engineered urologic tissues and cell therapy may soon have clinical applicability.
ACKNOWLEDGMENT
The authors wish to thank Dr. Jennifer Olson for editorial assistance with this paper.
References
- 1.Kim BS, Mooney DJ. Development of biocompatible synthetic extracellular matrices for tissue engineering. Trends in Biotechnology. 1998;16(5):224–229. doi: 10.1016/s0167-7799(98)01191-3. [DOI] [PubMed] [Google Scholar]
- 2.Li ST. Biologic biomaterials: tissue derived biomaterials (collagen) In: Bronzino JD, editor. The Biomedical Engineering Handbook. Boca Raton, Fla, USA: CRS Press; 1995. pp. 627–647. [Google Scholar]
- 3.Furthmayr H, Timpl R. Immunochemistry of collagens and procollagens. International Review of Connective Tissue Research. 1976;7:61–99. doi: 10.1016/b978-0-12-363707-9.50008-3. [DOI] [PubMed] [Google Scholar]
- 4.Cen L, Liu W, Cui L, Zhang W, Cao Y. Collagen tissue engineering: development of novel biomaterials and applications. Pediatric Research. 2008;63(5):492–496. doi: 10.1203/PDR.0b013e31816c5bc3. [DOI] [PubMed] [Google Scholar]
- 5.Yannas IV, Burke JF, Gordon PL. Design of an artificial skin. II. Control of chemical composition. Journal of Biomedical Materials Research. 1980;14(2):107–131. doi: 10.1002/jbm.820140203. [DOI] [PubMed] [Google Scholar]
- 6.Yannas IV, Burke JF. Design of an artificial skin. I. Basic design principles. Journal of Biomedical Materials Research. 1980;14(1):65–81. doi: 10.1002/jbm.820140108. [DOI] [PubMed] [Google Scholar]
- 7.Cavallaro JF, Kemp PD, Kraus KH. Collagen fabrics as biomaterials. Biotechnology and Bioengineering. 1994;43(8):781–791. doi: 10.1002/bit.260430813. [DOI] [PubMed] [Google Scholar]
- 8.Dahms SE, Piechota HJ, Dahiya R, Lue TF, Tanagho EA. Composition and biomechanical properties of the bladder acellular matrix graft: comparative analysis in rat, pig and human. British Journal of Urology. 1998;82(3):411–419. doi: 10.1046/j.1464-410x.1998.00748.x. [DOI] [PubMed] [Google Scholar]
- 9.Piechota HJ, Dahms SE, Nunes LS, Dahiya R, Lue TF, Tanagho EA. In vitro functional properties of the rat bladder regenerated by the bladder acellular matrix graft. Journal of Urology. 1998;159(5):1717–1724. doi: 10.1097/00005392-199805000-00100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yoo JJ, Meng J, Oberpenning F, Atala A. Bladder augmentation using allogenic bladder submucosa seeded with cells. Urology. 1998;51(2):221–225. doi: 10.1016/s0090-4295(97)00644-4. [DOI] [PubMed] [Google Scholar]
- 11.Chen F, Yoo JJ, Atala A. Acellular collagen matrix as a possible “off the shelf” biomaterial for urethral repair. Urology. 1999;54(3):407–410. doi: 10.1016/s0090-4295(99)00179-x. [DOI] [PubMed] [Google Scholar]
- 12.Probst M, Dahiya R, Carrier S, Tanagho EA. Reproduction of functional smooth muscle tissue and partial bladder replacement. British Journal of Urology. 1997;79(4):505–515. doi: 10.1046/j.1464-410x.1997.00103.x. [DOI] [PubMed] [Google Scholar]
- 13.Gilding D. Biodegradable polymers. In: Williams D, editor. Biocompatibility of Clinical Implant Materials. Boca Raton, Fla, USA: CRC Press; 1981. pp. 209–232. [Google Scholar]
- 14.Freed LE, Vunjak-Novakovic G, Biron RJ, et al. Biodegradable polymer scaffolds for tissue engineering. Bio/Technology. 1994;12(7):689–693. doi: 10.1038/nbt0794-689. [DOI] [PubMed] [Google Scholar]
- 15.Mikos AG, Lyman MD, Freed LE, Langer R. Wetting of poly(L-lactic acid) and poly(DL-lactic-co-glycolic acid) foams for tissue culture. Biomaterials. 1994;15(1):55–58. doi: 10.1016/0142-9612(94)90197-x. [DOI] [PubMed] [Google Scholar]
- 16.Harris LD, Kim BS, Mooney DJ. Open pore biodegradable matrices formed with gas foaming. Journal of Biomedical Materials Research. 1998;42(3):396–402. doi: 10.1002/(sici)1097-4636(19981205)42:3<396::aid-jbm7>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 17.Han D, Gouma PI. Electrospun bioscaffolds that mimic the topology of extracellular matrix. Nanomedicine. 2006;2(1):37–41. doi: 10.1016/j.nano.2006.01.002. [DOI] [PubMed] [Google Scholar]
- 18.Choi JS, Lee SJ, Christ GJ, Atala A, Yoo JJ. The influence of electrospun aligned poly(ε-caprolactone)/collagen nanofiber meshes on the formation of self-aligned skeletal muscle myotubes. Biomaterials. 2008;29(19):2899–2906. doi: 10.1016/j.biomaterials.2008.03.031. [DOI] [PubMed] [Google Scholar]
- 19.Lee SJ, Liu J, Oh SH, Soker S, Atala A, Yoo JJ. Development of a composite vascular scaffolding system that withstands physiological vascular conditions. Biomaterials. 2008;29(19):2891–2898. doi: 10.1016/j.biomaterials.2008.03.032. [DOI] [PubMed] [Google Scholar]
- 20.Lee SJ, Oh SH, Liu J, Soker S, Atala A, Yoo JJ. The use of thermal treatments to enhance the mechanical properties of electrospun poly(ε-caprolactone) scaffolds. Biomaterials. 2008;29(10):1422–1430. doi: 10.1016/j.biomaterials.2007.11.024. [DOI] [PubMed] [Google Scholar]
- 21.Brivanlou AH, Gage FH, Jaenisch R, Jessell T, Melton D, Rossant J. Setting standards for human embryonic stem cells. Science. 2003;300(5621):913–916. doi: 10.1126/science.1082940. [DOI] [PubMed] [Google Scholar]
- 22.Richards M, Fong CY, Chan WK, Wong PC, Bongso A. Human feeders support prolonged undifferentiated growth of human inner cell masses and embryonic stem cells. Nature Biotechnology. 2002;20(9):933–936. doi: 10.1038/nbt726. [DOI] [PubMed] [Google Scholar]
- 23.Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663–676. doi: 10.1016/j.cell.2006.07.024. [DOI] [PubMed] [Google Scholar]
- 24.De Coppi P, Bartsch G, Jr., Siddiqui MM, et al. Isolation of amniotic stem cell lines with potential for therapy. Nature Biotechnology. 2007;25(1):100–106. doi: 10.1038/nbt1274. [DOI] [PubMed] [Google Scholar]
- 25.Atala A, Vacanti JP, Peters CA, Mandell J, Retik AB, Freeman MR. Formation of urothelial structures in vivo from dissociated cells attached to biodegradable polymer scaffolds in vitro. Journal of Urology. 1992;148(2):658–662. doi: 10.1016/s0022-5347(17)36685-5. [DOI] [PubMed] [Google Scholar]
- 26.Atala A, Cima LG, Kim W, et al. Injectable alginate seeded with chondrocytes as a potential treatment for vesicoureteral reflux. Journal of Urology. 1993;150(2, part 2):745–747. doi: 10.1016/s0022-5347(17)35603-3. [DOI] [PubMed] [Google Scholar]
- 27.Atala A, Freeman MR, Vacanti JP, Shepard J, Retik AB. Implantation in vivo and retrieval of artificial structures consisting of rabbit and human urothelium and human bladder muscle. Journal of Urology. 1993;150(2, part 2):608–612. doi: 10.1016/s0022-5347(17)35561-1. [DOI] [PubMed] [Google Scholar]
- 28.Atala A, Kim W, Paige KT, Vacanti CA, Retik AB. Endoscopic treatment of vesicoureteral reflux with a chondrocyte-alginate suspension. Journal of Urology. 1994;152(2, part 2):641–643. doi: 10.1016/s0022-5347(17)32671-x. [DOI] [PubMed] [Google Scholar]
- 29.Atala A, Schlussel RN, Retik AB. Renal cell growth in vivo after attachment to biodegradable polymer scaffolds. Journal of Urology. 1995;153(4) [Google Scholar]
- 30.Atala A, Guzman L, Retik AB. A novel inert collagen matrix for hypospadias repair. Journal of Urology. 1999;162(3, part 2):1148–1151. doi: 10.1016/S0022-5347(01)68105-9. [DOI] [PubMed] [Google Scholar]
- 31.Atala A. Tissue engineering in the genitourinary system. In: Atala A, Mooney DJ, editors. Tissue Engineering. Boston, Mass, USA: Birkhauser Press; 1997. p. 149. [Google Scholar]
- 32.Atala A. Autologous cell transplantation for urologic reconstruction. Journal of Urology. 1998;159(1):2–3. doi: 10.1016/s0022-5347(01)63994-6. [DOI] [PubMed] [Google Scholar]
- 33.Cilento BG, Freeman MR, Schneck FX, Retik AB, Atala A. Phenotypic and cytogenetic characterization of human bladder urothelia expanded in vitro. Journal of Urology. 1994;152(2, part 2):665–670. doi: 10.1016/s0022-5347(17)32676-9. [DOI] [PubMed] [Google Scholar]
- 34.Yoo JJ, Atala A. A novel gene delivery system using urothelial tissue engineered neo- organs. Journal of Urology. 1997;158(3):1066–1070. doi: 10.1097/00005392-199709000-00098. [DOI] [PubMed] [Google Scholar]
- 35.Fauza DO, Fishman SJ, Mehegan K, Atala A. Videofetoscopically assisted fetal tissue engineering: skin replacement. Journal of Pediatric Surgery. 1998;33(2):357–361. doi: 10.1016/s0022-3468(98)90462-6. [DOI] [PubMed] [Google Scholar]
- 36.Fauza DO, Fishman SJ, Mehegan K, Atala A. Videofetoscopically assisted fetal tissue engineering: bladder augmentation. Journal of Pediatric Surgery. 1998;33(1):7–12. doi: 10.1016/s0022-3468(98)90350-5. [DOI] [PubMed] [Google Scholar]
- 37.Machluf M, Atala A. Emerging concepts for tissue and organ transplantation. Grafting. 1998;1(1):31–37. [Google Scholar]
- 38.Amiel GE, Atala A. Current and future modalities for functional renal replacement. Urologic Clinics of North America. 1999;26(1):235–246. doi: 10.1016/s0094-0143(99)80019-6. [DOI] [PubMed] [Google Scholar]
- 39.Kershen RT, Atala A. New advances in injectable therapies for the treatment of incontinence and vesicoureteral reflux. Urologic Clinics of North America. 1999;26(1):81–94. doi: 10.1016/s0094-0143(99)80008-1. [DOI] [PubMed] [Google Scholar]
- 40.Oberpenning F, Meng J, Yoo JJ, Atala A. De novo reconstitution of a functional mammalian urinary bladder by tissue engineering. Nature Biotechnology. 1999;17(2):149–155. doi: 10.1038/6146. [DOI] [PubMed] [Google Scholar]
- 41.Park HJ, Yoo JJ, Kershen RT, Moreland R, Atala A. Reconstitution of human corporal smooth muscle and endothelial cells in vivo. Journal of Urology. 1999;162(3, part 2):1106–1109. doi: 10.1016/S0022-5347(01)68084-4. [DOI] [PubMed] [Google Scholar]
- 42.Liebert M, Hubbel A, Chung M, et al. Expression of mal is associated with urothelial differentiation in vitro: identification by differential display reverse-transcriptase polymerase chain reaction. Differentiation. 1997;61(3):177–185. doi: 10.1046/j.1432-0436.1997.6130177.x. [DOI] [PubMed] [Google Scholar]
- 43.Liebert M, Wedemeyer G, Abruzzo LV, et al. Stimulated urothelial cells produce cytokines and express an activated cell surface antigenic phenotype. Seminars in Urology. 1991;9(2):124–130. [PubMed] [Google Scholar]
- 44.Tobin MS, Freeman MR, Atala A. Maturational response of normal human urothelial cells in culture is dependent on extracellular matrix and serum additives. Surgery Forum. 1994;45:p. 786. [Google Scholar]
- 45.Harriss DR. Smooth muscle cell culture: a new approach to the study of human detrusor physiology and pathophysiology. British Journal of Urology. 1995;75(supplement 1):18–26. [PubMed] [Google Scholar]
- 46.Freeman MR, Yoo JJ, Raab G, et al. Heparin-binding EGF-like growth factor is an autocrine growth factor for human urothelial cells and is synthesized by epithelial and smooth muscle cells in the human bladder. Journal of Clinical Investigation. 1997;99(5):1028–1036. doi: 10.1172/JCI119230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Solomon LZ, Jennings AM, Sharpe P, Cooper AJ, Malone PS. Effects of short-chain fatty acids on primary urothelial cells in culture: implications for intravesical use in enterocystoplasties. Journal of Laboratory and Clinical Medicine. 1998;132(4):279–283. doi: 10.1016/s0022-2143(98)90040-3. [DOI] [PubMed] [Google Scholar]
- 48.Lobban ED, Smith BA, Hall GD, et al. Uroplakin gene expression by normal and neoplastic human urothelium. American Journal of Pathology. 1998;153(6):1957–1967. doi: 10.1016/S0002-9440(10)65709-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Nguyen HT, Park JM, Peters CA, et al. Cell-specific activation of the HB-EGF and ErbB1 genes by stretch in primary human bladder cells [3] In Vitro Cellular and Developmental Biology—Animal. 1999;35(7):371–375. doi: 10.1007/s11626-999-0110-9. [DOI] [PubMed] [Google Scholar]
- 50.Puthenveettil JA, Burger MS, Reznikoff CA. Replicative senescence in human uroepithelial cells. Advances in Experimental Medicine and Biology. 1999;462:83–91. doi: 10.1007/978-1-4615-4737-2_7. [DOI] [PubMed] [Google Scholar]
- 51.Rackley RR, Bandyopadhyay SK, Fazeli-Matin S, Shin MS, Appell R. Immunoregulatory potential of urothelium: characterization of NF-κB signal transduction. Journal of Urology. 1999;162(5):1812–1816. doi: 10.1016/s0022-5347(05)68243-2. [DOI] [PubMed] [Google Scholar]
- 52.Bretan PN., Jr. History of the prosthetic treatment of impotence. Urologic Clinics of North America. 1989;16(1):1–5. [PubMed] [Google Scholar]
- 53.Nukui F, Okamoto S, Nagata M, Kurokawa J, Fukui J. Complications and reimplantation of penile implants. International Journal of Urology. 1997;4(1):52–54. doi: 10.1111/j.1442-2042.1997.tb00140.x. [DOI] [PubMed] [Google Scholar]
- 54.Yoo JJ, Lee I, Atala A. Cartilage rods as a potential material for penile reconstruction. Journal of Urology. 1998;160(3, part 2):1164–1168. doi: 10.1097/00005392-199809020-00056. [DOI] [PubMed] [Google Scholar]
- 55.Yoo JJ, Park HJ, Lee I, Atala A. Autologous engineered cartilage rods for penile reconstruction. Journal of Urology. 1999;162(3, part 2):1119–1121. doi: 10.1016/S0022-5347(01)68090-X. [DOI] [PubMed] [Google Scholar]
- 56.Xu Y, Qiao Y, Sa Y, et al. An experimental study of colonic mucosal graft for urethral reconstruction. Chinese Medical Journal. 2002;115(8):1163–1165. [PubMed] [Google Scholar]
- 57.Hardy Hendren W, Reda EF. Bladder mucosa graft for construction of male urethra. Journal of Pediatric Surgery. 1986;21(3):189–192. doi: 10.1016/s0022-3468(86)80828-4. [DOI] [PubMed] [Google Scholar]
- 58.Hensle TW, Kearney MC, Bingham JB, et al. Buccal mucosa grafts for hypospadias surgery: long-term results. Journal of Urology. 2002;168(4):1734–1737. doi: 10.1097/01.ju.0000027178.94140.00. [DOI] [PubMed] [Google Scholar]
- 59.Vozzi G, Flaim CJ, Bianchi F, Ahluwalia A, Bhatia S. Microfabricated PLGA scaffolds: a comparative study for application to tissue engineering. Materials Science and Engineering C. 2002;20(1-2):43–47. [Google Scholar]
- 60.Guzman L. Neourethra with rectum, posterior sagittal approach. In: Erhrlich RM, Atlter GJ, editors. Reconstructive and Plastic Surgery of the External Genitalia: Adult and Pediatric. Philadelphia, Pa, USA: WB Saunders; 1999. p. 101. [Google Scholar]
- 61.Atala A. Experimental and clinical experience with tissue engineering techniques for urethral reconstruction. Urologic Clinics of North America. 2002;29(2):485–492. doi: 10.1016/s0094-0143(02)00033-2. [DOI] [PubMed] [Google Scholar]
- 62.Atala A, Vacanti JP, Peters CA, Mandell J, Retik AB, Freeman MR. Formation of urothelial structures in vivo from dissociated cells attached to biodegradable polymer scaffolds in vitro. Journal of Urology. 1992;148(2, part 2):658–662. doi: 10.1016/s0022-5347(17)36685-5. [DOI] [PubMed] [Google Scholar]
- 63.Bazeed MA, Thuroff JW, Schmidt RA, Tanagho EA. New treatment for urethral strictures. Urology. 1983;21(1):53–57. doi: 10.1016/0090-4295(83)90123-1. [DOI] [PubMed] [Google Scholar]
- 64.Kropp BP, Ludlow JK, Spicer D, et al. Rabbit urethral regeneration using small intestinal submucosa onlay grafts. Urology. 1998;52(1):138–142. doi: 10.1016/s0090-4295(98)00114-9. [DOI] [PubMed] [Google Scholar]
- 65.Olsen L, Bowald S, Busch C, Carlsten J, Eriksson I. Urethral reconstruction with a new synthetic absorbable device. An experimental study. Scandinavian Journal of Urology and Nephrology. 1992;26(4):323–326. doi: 10.3109/00365599209181220. [DOI] [PubMed] [Google Scholar]
- 66.Sievert KD, Bakircioglu ME, Nunes L, Tu R, Dahiya R, Tanagho EA. Homologous acellular matrix graft for urethral reconstruction in the rabbit: histological and functional evaluation. Journal of Urology. 2000;163(6):1958–1965. [PubMed] [Google Scholar]
- 67.Italiano G, Abatangelo G, Jr., Calabro’ A, et al. Reconstructive surgery of the urethra: a pilot study in the rabbit on the use of hyaluronan benzyl ester (Hyaff-11) biodegradable grafts. Urological Research. 1997;25(2):137–142. doi: 10.1007/BF01037930. [DOI] [PubMed] [Google Scholar]
- 68.Shaul DB, Xie HW, Diaz JF, Mahnovski V, Hardy BE. Use of tubularized peritoneal free grafts as urethral substitutes in the rabbit. Journal of Pediatric Surgery. 1996;31(2):225–228. doi: 10.1016/s0022-3468(96)90002-0. [DOI] [PubMed] [Google Scholar]
- 69.El-Assmy A, El-Hamid MA, Hafez AT. Urethral replacement: a comparison between small intestinal submucosa grafts and spontaneous regeneration. BJU International. 2004;94(7):1132–1135. doi: 10.1111/j.1464-410X.2004.05115.x. [DOI] [PubMed] [Google Scholar]
- 70.El Kassaby A, AbouShwareb T, Atala A. Randomized comparative study between buccal mucosal and acellular bladder matrix grafts in complex anterior urethral strictures. Journal of Urology. 2008;179(4):1432–1436. doi: 10.1016/j.juro.2007.11.101. [DOI] [PubMed] [Google Scholar]
- 71.Atala A, Guzman L, Retik AB. A novel inert collagen matrix for hypospadias repair. Journal of Urology. 1999;162(3, part 2):1148–1151. doi: 10.1016/S0022-5347(01)68105-9. [DOI] [PubMed] [Google Scholar]
- 72.El-Kassaby AW, Retik AB, Yoo JJ, Atala A. Urethral stricture repair with an off-the-shelf collagen matrix. Journal of Urology. 2003;169(1):170–173. doi: 10.1016/S0022-5347(05)64060-8. [DOI] [PubMed] [Google Scholar]
- 73.Chen F, Yoo JJ, Atala A. Experimental and clinical experience using tissue regeneration for urethral reconstruction. World Journal of Urology. 2000;18(1):67–70. doi: 10.1007/s003450050012. [DOI] [PubMed] [Google Scholar]
- 74.Dorin RP, Pohl HG, De Filippo RE, Yoo JJ, Atala A. Tubularized urethral replacement with unseeded matrices: what is the maximum distance for normal tissue regeneration? World Journal of Urology. 2008;26(4):323–326. doi: 10.1007/s00345-008-0316-6. [DOI] [PubMed] [Google Scholar]
- 75.De Filippo RE, Yoo JJ, Atala A. Urethral replacement using cell seeded tubularized collagen matrices. Journal of Urology. 2002;168(4):1789–1792. doi: 10.1097/01.ju.0000027662.69103.72. [DOI] [PubMed] [Google Scholar]
- 76.Cilento BG, Freeman MR, Schneck FX, Retik AB, Atala A. Phenotypic and cytogenetic characterization of human bladder urothelia expanded in vitro. Journal of Urology. 1994;152(2, part 2):665–670. doi: 10.1016/s0022-5347(17)32676-9. [DOI] [PubMed] [Google Scholar]
- 77.Puthenveettil JA, Burger MS, Reznikoff CA. Replicative senescence in human uroepithelial cells. Advances in Experimental Medicine and Biology. 1999;462:83–91. doi: 10.1007/978-1-4615-4737-2_7. [DOI] [PubMed] [Google Scholar]
- 78.Scriven SD, Booth C, Thomas DFM, et al. Reconstitution of human urothelium from monolayer cultures. Journal of Urology. 1997;158(3, part 2):1147–1153. doi: 10.1097/00005392-199709000-00115. [DOI] [PubMed] [Google Scholar]
- 79.Amiel GE, Yoo JJ, Kim BS, Atala A. Tissue engineered stents created from chondrocytes. Journal of Urology. 2001;165(6, part 1):2091–2095. doi: 10.1097/00005392-200106000-00076. [DOI] [PubMed] [Google Scholar]
- 80.Horton CE, Dean JA. Reconstruction of traumatically acquired defects of the phallus. World Journal of Surgery. 1990;14(6):757–762. doi: 10.1007/BF01670522. [DOI] [PubMed] [Google Scholar]
- 81.Sharaby JS, Benet AE, Melman A. Penile revascularization. Urologic Clinics of North America. 1995;22(4):821–832. [PubMed] [Google Scholar]
- 82.Kershen RT, Yoo JJ, Moreland RB, Krane RJ, Atala A. Reconstitution of human corpus cavernosum smooth muscle in vitro and in vivo. Tissue Engineering. 2002;8(3):515–524. doi: 10.1089/107632702760184754. [DOI] [PubMed] [Google Scholar]
- 83.Falke G, Yoo JJ, Kwon TG, Moreland R, Atala A. Formation of corporal tissue architecture in vivo using human cavernosal muscle and endothelial cells seeded on collagen matrices. Tissue Engineering. 2003;9(5):871–879. doi: 10.1089/107632703322495529. [DOI] [PubMed] [Google Scholar]
- 84.Jackson CJ, Garbett PK, Nissen B, Schrieber L. Binding of human endothelium to Ulex europaeus I-coated Dynabeads: application to the isolation of microvascular endothelium. Journal of Cell Science. 1990;96, part 2:257–262. doi: 10.1242/jcs.96.2.257. [DOI] [PubMed] [Google Scholar]
- 85.Krǎling BM, Bischoff J. A simplified method for growth of human microvascular endothelial cells results in decreased senescence and continued responsiveness to cytokines and growth factors. In Vitro Cellular and Developmental Biology—Animal. 1998;34(4):308–315. doi: 10.1007/s11626-998-0007-z. [DOI] [PubMed] [Google Scholar]
- 86.Chen KL, Eberli D, Yoo JJ, Atala A. Bioengineered corporal tissue for structural and functional restoration of the penis. Proceedings of the National Academy of Sciences of the United States of America. 2010;107(8):3346–3350. doi: 10.1073/pnas.0909367106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Eberli D, Susaeta R, Yoo JJ, Atala A. A method to improve cellular content for corporal tissue engineering. Tissue Engineering—Part A. 2008;14(10):1581–1589. doi: 10.1089/ten.tea.2007.0249. [DOI] [PubMed] [Google Scholar]
- 88.Kadioglu A, Sanli O, Akman T, Ersay A, Guven S, Mammadov F. Graft materials in peyronie’s disease surgery: a comprehensive review. Journal of Sexual Medicine. 2007;4(3):581–595. doi: 10.1111/j.1743-6109.2007.00461.x. [DOI] [PubMed] [Google Scholar]
- 89.Schultheiss D, Lorenz RR, Meister R, et al. Functional tissue engineering of autologous tunica albuginea: a possible graft for Peyronie’s disease surgery. European Urology. 2004;45(6):781–786. doi: 10.1016/j.eururo.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 90.Joo KJ, Kim BS, Han JH, Kim CJ, Kwon CH, Park HJ. Porcine vesical acellular matrix graft of tunica albuginea for penile reconstruction. Asian Journal of Andrology. 2006;8(5):543–548. doi: 10.1111/j.1745-7262.2006.00192.x. [DOI] [PubMed] [Google Scholar]