

Abstract
Objective
To evaluate ecological model predictions of cross-level interactions among psychosocial and environmental correlates of physical activity in 719 community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008.
Method
Walkability, access to parks and recreation facilities and moderate-to-vigorous physical activity (MVPA) minutes per week (min/week) were measured objectively. Neighborhood aesthetics, walking facilities, social support, self-efficacy, barriers and transportation and leisure walking min/week were self-reported.
Results
Walkability interacted with social support in explaining total MVPA (B = 13.71) and with social support (B = 7.90), self-efficacy (B = 7.66) and barriers (B = −8.26) in explaining walking for transportation. Aesthetics interacted with barriers in explaining total MVPA (B = −12.20) and walking facilities interacted with self-efficacy in explaining walking for leisure (B = −10.88; Ps < .05). Summarizing across the interactions, living in a supportive environment (vs. unsupportive) was related to 30-59 more min/week of physical activity for participants with more positive psychosocial attributes, but only 0-28 more min/week for participants with less positive psychosocial attributes.
Conclusion
Results supported synergistic interactions between built environment and psychosocial factors in explaining physical activity among older adults. Findings suggest multilevel interventions may be most effective in increasing physical activity.
Keywords: ecological models, moderators, self-efficacy, social support, walkability
Physical activity is particularly important among older adults, who represent the least active population group yet can benefit greatly from increasing activity levels (Nelson et al., 2007; Troiano et al., 2008; USDHHS, 2008). Physical activity interventions in older adults often focus on changing psychosocial skills, barriers, self-efficacy and social support (Kahn et al., 2002; King et al., 1998; Marcus et al., 2006). Yet, built environment factors such as walkability and parks are also related to older adults’ physical activity (Frank et al., 2010a; Yen et al., 2009; Hall and McAuley, 2010; Clarke and Nieuwenhuijsen, 2009; van Cauwenberg et al., 2010). Older adults may be particularly susceptible to built environment influences because they may prefer shorter walking distances, require safe pedestrian facilities, and have more time to spend in parks.
Ecological models posit interactions among multiple levels of influence (e.g., individual, interpersonal, environmental) on behavior (McLeroy et al., 1988; Sallis et al., 2008; Stokols, 1996). An implication of these models is that programmatic interventions to enhance psychosocial constructs associated with physical activity may be more effective among people located in physical settings that enable rather than restrict physical activity. Conversely, improving the built environment to promote physical activity may be more effective where efforts are made to enhance psychosocial support and motivation.
Although studies have investigated multivariable models that include both environmental and psychosocial predictors of physical activity (e.g., Giles-Corti and Donovan, 2002; Giles-Corti and Donovan, 2003), only two studies have investigated interactions between environmental and psychosocial variables. One study investigating environment by psychosocial interactions found that access to recreation facilities was positively related to physical activity in participants with high levels of intention but negatively related to physical activity in participants with low levels of intention (Rhodes et al., 2006). Another study found that access to recreation facilities was positively associated with physical activity only in participants with low psychosocial attributes (i.e., self-efficacy and enjoyment) (Cerin et al., 2008). These inconsistent findings warrant further investigation.
Though general predictions about the relevance of correlates for various domains of physical activity can be derived from activity-specific ecological models (Saelens et al., 2003b; Sallis et al., 2006), there is no basis for predicting specific environment by psychosocial interactions. The present study explored interactions among individual, interpersonal, and environmental correlates of physical activity in a large sample of community-dwelling older adults. The psychosocial and environmental variables were chosen based on their conceptual relevance and empirical associations with different domains of physical activity in previous studies (Saelens et al., 2003a; Trost et al., 2002; van Cauwenberg et al., 2010). Walkability was expected to interact with the psychosocial variables in explaining walking for transportation, whereas access to parks and recreation facilities, neighborhood aesthetics, and walking infrastructure were expected to interact with the psychosocial variables in explaining walking for recreation. All of the environmental variables were expected to interact with the psychosocial variables in explaining total physical activity. In agreement with predictions from ecological models, it was hypothesized that individual/interpersonal and environmental factors would be synergistic in their relation with physical activity, such that physical activity minutes would be greatest when both factors were supportive of physical activity, lowest when neither factor was supportive, and in between when only one factor was supportive.
Methods
Design
The present analyses used data from the Senior Neighborhood Quality of Life Study (SNQLS) that was conducted in the Baltimore, Maryland-Washington, DC and Seattle-King County, Washington regions during 2005-2008 (King et al., under review). The primary aim of SNQLS was to investigate the relationship between built environment factors and physical activity in older adults. Census block groups (n = 216) were chosen to represent high and low walkability based on an index using parcel and street network data from which measures of residential density, land use mix, street connectivity, and retail floor area ratio were derived, as well as high and low income level based on census data (King et al., under review; Buman et al., 2010).
Participants
A total of 718 seniors who lived independently in the community were recruited. Households within each selected block group with an adult over age 65 years were identified by a marketing company. The sampling was designed to be balanced by gender and to approximate the ethnic distribution of the regions. Participants were ineligible if they were unable to walk or complete surveys in English. Participants were mailed an accelerometer and survey with instructions to complete the survey after wearing the accelerometer for one week. Participants returned the accelerometer and survey in the mail and received an incentive.
Measures
Demographics
Age, gender, ethnicity (non-Hispanic white vs. non-white), education (college degree vs. no college degree), number of adults and children in the household, length of time at current address, number of motor vehicles per adults in household, and marital status (married/living together vs. other) were collected by survey.
Psychosocial Measures
Self-efficacy for physical activity was assessed using a 3-item (α = 0.87) scale asking participants to rate their confidence in their ability to walk ½ block, 4 blocks, and 10 blocks on a 10-point scale. Psychosocial barriers to physical activity were assessed using a 4-item (α = 0.53) scale asking participants to rate barriers such as discomfort and time constraints (Marcus et al., 1992). Social support for physical activity was measured by asking participants to separately rate how often during the past 3 months their friends and family did supportive behaviors such as walk or exercise with them and gave them encouragement to do physical activity (4 items; α = 0.67) (Sallis et al., 1987). In a previous study, two-week ICCs for the barriers and social support scales were .61 and .67 and correlations with self-report physical activity were −.19 and .12 in women (Carlson et al., in press).
Objective Environment Measures
Data from the county-level tax assessor, land use at the parcel level, and street networks were integrated into GIS to create a walkability index for each participant based on a 500 meter buffer around his/her home. The index consisted of the sum of z-scores of measures of residential density, retail floor area ratio, intersection density and land use mix (Frank et al., 2010b). Parcel-level land use data, supplemented with lists from local parks agencies, were used to determine the number of parks within the 500 meter buffer around each participant’s home. Private recreation facilities (e.g., gyms, dance and martial arts studios) within each county were identified and geocoded (Abercrombie et al., 2008). The count of parks and private recreation facilities within 500 meters of each participant’s home was calculated and dichotomized as 0 or ≥ 1.
Perceived Environment Measures
Neighborhood aesthetics was assessed using the following items: “There are trees along the streets in my neighborhood”, “There are many interesting things to look at while walking in my neighborhood”, “There are many attractive natural sights in my neighborhood (such as landscaping, views)” and “There are attractive buildings/homes in my neighborhood” from the Neighborhood Environment Walkability Scale (NEWS; α = 0.77). Presence of walking/cycling facilities was measured using the items “There are sidewalks on most of the streets in my neighborhood”, “Sidewalks are separated from the road/traffic in my neighborhood by parked cars” and “There is a grass/dirt strip that separates the streets from the sidewalks in my neighborhood” from the NEWS (α = 0.74) (Saelens et al., 2003b).
Physical activity
ActiGraph accelerometers (Manufacturing Technology Incorporated, models 7164 and 71256; Fort Walton, FL) with a 60-second epoch setting were used to objectively measure participants’ total physical activity (Buman et al., 2010). For scoring, 5 valid days were required. A valid day contained at least 8 valid hours of wear time, and a valid hour contained no more than 45 consecutive zero counts. Average minutes per week (min/week) of moderate to vigorous physical activity (MVPA) were calculated using previously established cut-points (1953-10000 counts) (Freedson et al., 1998).
The Community Healthy Activities Model Program for Seniors (CHAMPS) survey was used to assess self-reported physical activity. Six-month stability was acceptable (ICCs 0.58-0.67), and the measure was able to discriminate between inactive, somewhat active, and active persons (Stewart et al., 2001). An average min/week variable was computed for the walking for transportation and walking for leisure single item scales.
Analysis
Mixed effects regression models were conducted using SPSS version 17.0 with block group entered as a random effect cluster variable. The intraclass correlation coefficient (ICC) assessing proportion of variance between block groups was examined for each outcome variable with no other variables in the model. One model was estimated for each outcome variable that included the psychosocial variables, environmental variables, and their interactions (3 models total). Continuous independent variables were standardized to have a mean of zero and standard deviation (SD) of 1, so the unstandardized coefficients (B) with 95% confidence intervals (CI) could be interpreted as change in min/week of physical activity for every 1 SD change in the predictor. Standardized coefficients (β) were calculated by standardizing the outcome variables to have a mean of zero and standard deviation of 1. A p-value of 0.05 was used to interpret significance. Significant demographic variables respective to each outcome were controlled for in each model. Line graphs were created for significant interactions by plotting predicted physical activity (in min/week) from the regression equation. Graphs included the effect of the environmental variable (at −1 and +1 SD for continuous variables, and at 0 and 1 for the parks and recreation facilities variables) for each level of the psychosocial variable (at −1 and +1 SD).
Results
Participant demographic characteristics are presented in Table 1 and descriptive statistics of independent variables are presented in Table 2. Final sample size ranged from 687 to 709 due to missing data. Participants engaged in an average of 93.6 min/week of total MVPA, 40.9 min/week of walking for transportation, and 99.5 min/week of walking for leisure (see Table 3). Table 4 shows the relation of the environmental and psychosocial variables to min/week of physical activity.
Table 1.
Participant Demographic Characteristics (n = 718)
| % | |
|---|---|
| Women | 53.1 |
| Non-Hispanic white | 70.7 |
| With college degree | 48.8 |
| Married or living with partner | 56.8 |
| Residing in the Baltimore region | 49.3 |
| Mode | |
| Number of vehicles in household | 1.0 |
| Mean (SD) | |
| Number of vehicles in household | 0.9 (0.5) |
| Age in years | 74.4 (6.3) |
| Number of people in household | 1.8 (0.8) |
| Years at current address | 24.7 (12.5) |
SD = standard deviation
This study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Table 2.
Descriptive Statistics for Independent Variables (n = 718)
| Mean (SD) | Range | |
|---|---|---|
| Social Support | 2.4 (1.0) | 1 – 5 |
| Self-Efficacy | 8.3 (2.6) | 1 – 10 |
| Barriers | 1.6 (0.6) | 1 – 5 |
| Walkability Index | −0.1 (2.8) | −4.1 – 12.5 |
| Perceived Aesthetics | 3.1 (0.7) | 1 – 4 |
| Perceived Walking Facilities | 2.8 (0.9) | 1 – 4 |
| Range % |
||
|---|---|---|
| Lower Dichotomy | Upper Dichotomy | |
| Number Parks | 0 | 1.0 – 7.00 |
| 39.7% | 60.3% | |
| Number Recreation Facilities | 0 | 1.00 – 31.00 |
| 57.7% | 42.3% | |
SD = standard deviation
This study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Table 3.
Participants’ Minutes of Physical Activity
| Median | Mean (SD) | Range | |
|---|---|---|---|
| Total MVPA min/week (n = 687) | 44.0 | 93.6 (115.4) | 0 – 825.0 |
| Walking for transportation min/week (n = 707) | 0.0 | 40.9 (82.6) | 0 – 585.0 |
| Walking for leisure min/week (n = 709) | 105.0 | 99.5 (125.9) | 0 – 585.0 |
MVPA = moderate to vigorous physical activity
Min/week = minutes per week
SD = standard deviation
This study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Table 4.
Relation of Environment and Psychosocial Factors to Physical Activity in Older Adults
| Model 1: Total MVPA min/weeka n = 687; ICC = .11d |
Model 2: Walking for Transportation min/weekb n = 707; ICC = .31d |
Model 3: Walking for Leisure min/weekc n = 709; ICC = .04d |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| B (95% CI) | β (95% CI) | p | B (95% CI) | β (95% CI) | p | B (95% CI) | β (95% CI) | p | |
| Intercept | 85.75 | −0.07 | - | 30.57 | −0.13 | - | 101.09 | 0.01 | - |
| Walkability | 13.83 (5.02, 22.63) | 0.12 (0.04, 0.20) | 0.002** | 21.52 (14.91, 28.14) | 0.26 (0.18, 0.34) | <0.001** | 12.52 (2.03, 23.01) | 0.10 (0.02, 0.18) | 0.019* |
| Parks and Recreation Facilities | 7.59 (−10.86, 26.03) | 0.07 (−0.09, 0.23) | 0.419 | 9.12 (−4.18, 22.42) | 0.11 (−0.05, 0.27) | 0.178 | −8.09 (−29.72, 13.53) | −0.06, (−0.24, 0.11) | 0.463 |
| Aesthetics | 2.99 (−5.28, 11.27) | 0.03 (−0.05, 0.10) | 0.478 | 0.45 (−5.60, 6.51) | 0.01 (−0.07, 0.08) | 0.883 | 0.09 (−9.82, 9.99) | 0.00 (−0.08, 0.08) | 0.986 |
| Walking Facilities | −3.54 (−11.87, 4.78) | −0.03 (−0.10, 0.04) | 0.403 | −1.14 (−7.19, 4.91) | −0.01 (−0.09, 0.06) | 0.711 | −3.13 (−12.95, 6.69) | −0.02 (−0.10, 0.05) | 0.532 |
| Social Support | 14.35 (5.76, 22.94) | 0.12 (0.05, 0.20) | 0.001** | 7.36 (1.13, 13.59) | 0.09 (0.01, 0.16) | 0.021* | 26.28 (16.08, 36.47) | 0.21 (0.13, 0.29) | <0.001** |
| Self-Efficacy | 26.59 (17.47, 35.70) | 0.23 (0.15, 0.310 | <0.001** | 15.13 (8.67, 21.59) | 0.18 (0.10, 0.26) | <0.001** | 20.45 (10.13, 30.77) | 0.16 (0.08, 0.24) | <0.001** |
| Barriers | −3.47 (−12.06, 5.12) | −0.03 (−0.10, 0.04) | 0.428 | −2.57 (−8.72, 3.58) | −0.03 (−0.11, 0.04) | 0.412 | −2.60 (−12.75, 7.55) | −0.02 (−0.10, 0.06) | 0.616 |
| Walkability X Social Support | 13.71 (4.73, 22.70) | 0.12 (0.04, 0.20) | 0.003** | 7.90 (1.42, 14.37) | 0.10 (0.02, 0.17) | 0.017* | 6.35 (−4.34, 17.04) | 0.05 (−0.03, 0.14) | 0.244 |
| Walkability X Self-Efficacy | −2.98 (−11.88, 5.93) | −0.03 (−0.10, 0.05) | 0.512 | 7.66 (1.21, 14.11) | 0.09 (0.01, 0.17) | 0.020* | −1.26 (−11.90, 9.38) | −0.01 (−0.09, 0.07) | 0.817 |
| Walkability X Barriers | −4.06 (−13.06, 4.94) | −0.04 (−0.11, 0.04) | 0.376 | −8.26 (−14.80, −1.72) | −0.10 (−0.18, −0.02) | 0.013* | −2.65 (−13.43, 8.12) | −0.02 (−0.11, 0.06) | 0.629 |
| Parks and Recreation Facilities X | −11.34 (−29.49, 6.81) | −0.10 (−0.26, 0.06) | 0.220 | 1.92 (−11.30, 15.15) | 0.02 (−0.14, 0.18) | 0.775 | −20.84 (−42.51, 0.83) | −0.17 (−0.34, 0.01) | 0.059 |
| Social Support | |||||||||
| Parks and Recreation Facilities X | 11.04 (−7.55, 29.63) | 0.10 (−0.07, 0.26) | 0.244 | 2.99 (−10.42, 16.40) | 0.04 (−0.13, 0.18) | 0.662 | −0.21 (−22.19, 21.77) | 0.00 (−0.18, 0.17) | 0.985 |
| Self-Efficacy | |||||||||
| Parks and Recreation Facilities X | −8.42 (−27.39, 10.54) | −0.07 (−0.24, 0.09) | 0.383 | 11.75 (−1.87, 25.37) | 0.14 (−0.02, 0.31) | 0.091 | 8.48 (−14.00, 30.97) | 0.07 (−0.11, 0.25) | 0.459 |
| Barriers | |||||||||
| Aesthetics X Social Support | −5.86 (−13.69, 1.98) | −0.05 (−0.12, 0.02) | 0.143 | −5.38 (−11.12, 0.35) | −0.07 (−0.13, 0.00) | 0.066 | −8.43 (−17.80, 0.94) | −0.07 (−0.14, 0.01) | 0.078 |
| Aesthetics X Self-Efficacy | 4.12 (−3.89, 12.12) | 0.04 (−0.03, 0.11) | 0.313 | 5.11 (−0.58, 10.79) | 0.06 (−0.01, 0.13) | 0.078 | 2.64 (−6.73, 12.02) | 0.02 (−0.05, 0.10) | 0.580 |
| Aesthetics X Barriers | −12.20 (−20.00, −4.41) | −0.11 (−0.17, −0.04) | 0.002** | 1.08 (−4.53, 6.69) | 0.01 (−0.05, 0.08) | 0.706 | 1.75 (−7.52, 11.01) | 0.01 (−0.06, 0.09) | 0.711 |
| Walking Facilities X Social | −3.61 (−11.79, 4.58) | −0.03 (−0.10, 0.04) | 0.387 | 0.80 (−5.23, 6.84) | 0.01 (−0.06, 0.08) | 0.795 | 1.11 (−8.70, 10.92) | 0.01 (−0.07, 0.09) | 0.825 |
| Support | |||||||||
| Walking Facilities X Self-Efficacy | −5.12 (−13.18, 2.93) | −0.04 (−0.11, 0.03) | 0.212 | −3.13 (−8.82, 2.56) | −0.04 (−0.11, 0.03) | 0.281 | −10.88 (−20.21, −1.56) | −0.09 (−0.16, −0.01) | 0.022* |
| Walking Facilities X Barriers | 3.51 (−4.84, 11.86) | 0.03 (−0.04, 0.10) | 0.409 | −1.67 (−7.74, 4.39) | −0.02 (−0.09, 0.05) | 0.588 | −3.59 (−13.58, 6.39) | −0.03 (−0.11, 0.05) | 0.480 |
MVPA = moderate to vigorous physical activity
Min/week = minutes per week
ICC = intraclass correlation coefficient
B = unstandardized regression coefficient β = regression coefficient when outcome variable was standardized to have a mean of zero and standard deviation of 1 CI = confidence interval
p < .05;
p < .01
Controlling for age, ethnicity and gender
Controlling for age, ethnicity, months at address and number of vehicles per adult
Controlling for ethnicity and months at address
ICCs (intraclass correlation coefficient assessing proportion of variance between block groups) are for the empty model containing only the block group variable Grey = expected interactions
This study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Total MVPA
Walkability (B = 13.83), social support (B = 14.35) and self-efficacy (B = 26.59) were associated with total MVPA min/week (p values < 0.01). There was a positive interaction between walkability and social support (B = 13.71) and a negative interaction between aesthetics and barriers (B = −12.20) in explaining total MVPA min/week (p < 0.01). For participants with high social support, high vs. low walkability accounted for 56 additional min/week of MVPA; for participants with low social support, walkability was not associated with MVPA (see Figure 1a). For participants with few barriers, high vs. low aesthetics accounted for 30 additional min/week of MVPA; for participants with more barriers, high vs. low aesthetics accounted for 18 fewer min/week of MVPA (see Figure 1b).
Figure 1. Environment by Psychosocial Interactions Explaing Total MVPA.
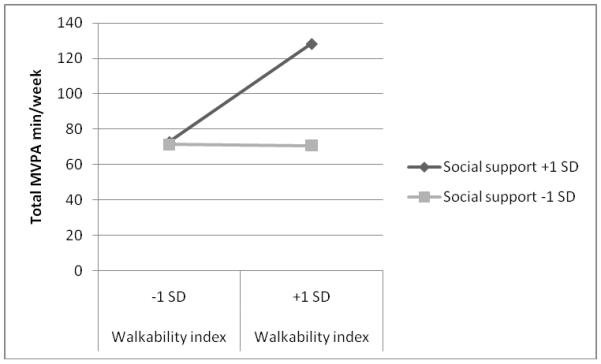

Note: MVPA = moderate to vigorous physical activity; min/week = minutes per week; this study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Walking for Transportation
Walkability (B = 21.52), social support (B = 7.36), and self-efficacy (B = 15.13) were associated with min/week of walking for transportation (p < .05). There were positive interactions between walkability and social support (B = 7.90) and walkability and self-efficacy (B = 7.66), and a negative interaction between walkability and barriers (B = −8.26) in explaining min/week of walking for transportation (p < .05). The effect of high vs. low walkability was 59 min/week of walking for transportation for participants with high social support, 27 min/week for those with low social support, 58 min/week for those with high self-efficacy, 28 min/week for those with low self-efficacy, 58 min/week for those with few barriers, and 28 min/week for those with greater barriers (see Figure 2).
Figure 2. Environment by Psychosocial Interactions Explaing Walking for Transportation.
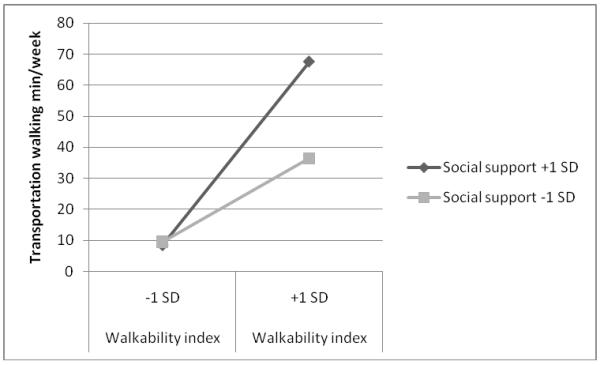
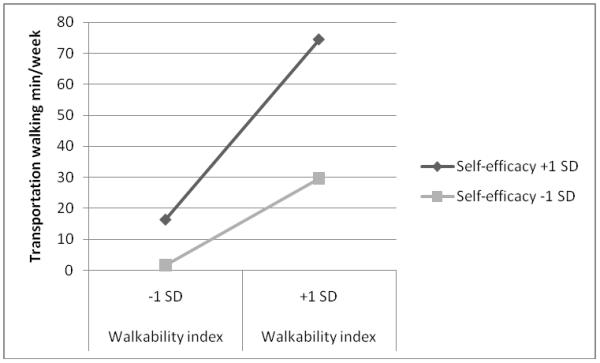
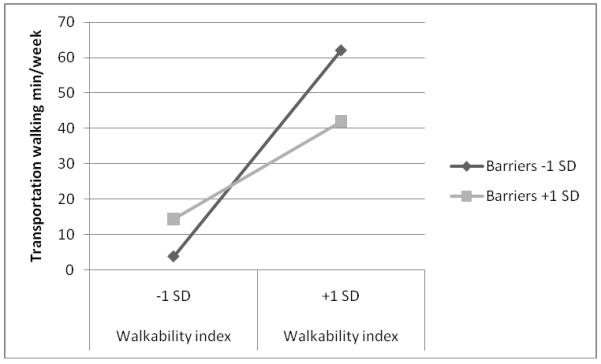
Note: Min/week = minutes per week; this study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Walking for Leisure
Walkability (B = 12.52), social support (B = 26.28) and self-efficacy (B = 20.45) were associated with min/week of walking for leisure (p < .05). There was a negative interaction between aesthetics and social support (B = −10.88) in explaining min/week of walking for leisure (p < .05). For participants with high self-efficacy, high vs. low walkability accounted for 26 fewer min/week of walking for leisure; for participants with low self-efficacy, high vs. low walkability accounted for 15 additional min/week of walking for leisure (see Figure 3).
Figure 3. Environment by Psychosocial Interactions Explaing Walking for Leisure.
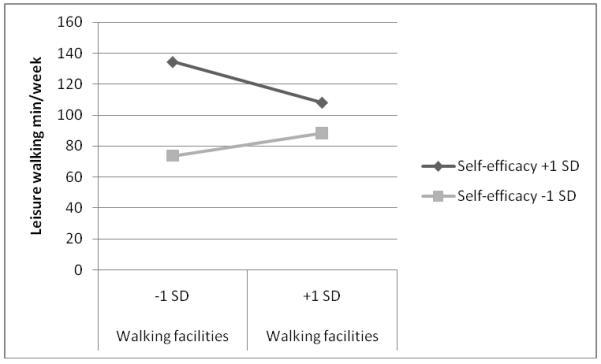
Note: Min/week = minutes per week; this study included community-dwelling older adults in the Baltimore, Maryland and Seattle, Washington areas during 2005-2008
Discussion
The present study provided some support for ecological model-predicted interactions between built environment and psychosocial factors in explaining physical activity among older adults. Six significant interactions were found (p < 0.05) and an additional 5 interaction terms displayed a trend for significance (p < 0.10) across the three physical activity metrics examined. For 5 of the 6 significant interactions, physical activity minutes were greater when both psychosocial and environmental factors were supportive of physical activity. Summarizing across the interactions, living in a supportive environment (vs. unsupportive) was related to 30-59 more minutes of physical activity per week for participants with more positive psychosocial attributes, but only 0-28 more minutes per week for participants with less positive psychosocial attributes.
Interactions were found for objectively measured total MVPA, walking for transportation, and walking for leisure outcomes. As expected based on ecological models (Saelens et al., 2003a; Sallis et al., 2006), the interactions related to walking for transportation involved walkability, while the interactions related to walking for leisure tended to involve walking infrastructure (interactions involving access to parks and recreation facilities and neighborhood aesthetics displayed a trend for significance). There were fewer significant interactions explaining total MVPA, which could be because total MVPA captures multiple domains of physical activity, so has less specific conceptual matches with environmental variables.
Walkability, social support, and self-efficacy were consistently related to physical activity. Walkability interacted with social support to explain total MVPA and walking for transportation. The combination of a walking partner and a supportive environment may be particularly effective in facilitating older adults’ physical activity. It is possible that environments that are less conducive to physical activity have fewer opportunities for social support enhancement.
Though most of the significant interactions indicated synergistic effects, there were some interesting exceptions. For participants with greater psychosocial barriers to physical activity, aesthetics seemed to have a slightly negative association with total MVPA. This suggests that sometimes built environment supports cannot make up for low psychosocial resources. Even more unexpected was that more positive walking facilities were related to less walking for leisure in participants who had high self-efficacy. However, this is similar to findings from a study by Cerin and colleagues (Cerin et al., 2008). Older adults who walk for leisure more in their neighborhoods and who have higher confidence in their ability to be active are perhaps more likely to be critical of the existing walking infrastructure and have a desire for more walking infrastructure. In contrast, older adults not out leisure walking in their neighborhood may assume such infrastructure is sufficient.
Most participants were non-Hispanic white and almost half had a college degree. This may limit generalizability to more ethnically and/or economically diverse samples. Future studies should examine whether psychosocial factors interact with environmental features differently by personal income, ethnicity, age, and gender combinations that extend beyond the capabilities of the current dataset. For example, social support and walkability may have greater synergistic effects for older women than younger men. Future studies should also investigate other aspects of the built environment that are related to physical activity in older adults such as access to benches and resting places (Joseph et al., 2005). Finally, the accelerometer cut points were derived in adults as opposed to older adults; although the same cut points have been used in studies including older adults, it is possible that a lower cut point has greater validity in this population (Miller et al., 2010; Pruitt et al., 2008).
Conclusions
Experience with multilevel community interventions is accumulating (Bors et al., 2009), but evaluations have not been sufficient to understand their effects (Samuels et al., 2010). The present findings, if suitably replicated, imply that multilevel interventions that change both psychosocial and environmental variables may be most effective in increasing physical activity. The results also suggest considerable utility can be gained by targeting populations that rank high on one but not the other. For example, in areas where walkable communities are being created through new construction or redevelopment, individually targeted behavior change techniques may be especially beneficial. These types of multilevel interventions are likely to be required to increase physical activity levels in older adults above the current low prevalence levels (Troiano et al., 2008). Policy makers should consider how to provide both psychosocial and built environment resources to support seniors’ physical activity.
Supplementary Material
Highlights.
Built environment and psychosocial factors interact in influencing physical activity.
Older adults are the least active age group.
Environment and psychosocial factors together generally influenced activity the most.
Interventions to increase activity should focus on both levels of factors.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Jordan A. Carlson, Joint Doctoral Program in Public Health San Diego State University & University of California, San Diego 3900 Fifth Avenue, Suite 310 San Diego, CA 92103 USA jcarlson@projects.sdsu.edu
Terry L. Conway, Graduate School of Public Health San Diego State University 3900 Fifth Avenue, Suite 310 San Diego, CA 92103 USA tconway@mail.sdsu.edu
Brian E. Saelens, Department of Pediatrics University of Washington & Children’s Hospital and Regional Medical Center 1100 Olive Way, Suite 500 Seattle, WA 98101 USA bsaelens@u.washington.edu
Lawrence D. Frank, School of Community and Regional Planning University of British Columbia, Vancouver BC #433-6333 Memorial Road Vancouver, BC V6T 1Z2 CANADA ldfrank@urbandesign4health.com
Jacqueline Kerr, Department of Family and Preventive Medicine University of California, San Diego 9500 Gilman Drive # 0811 La Jolla, CA 92093 USA jkerr@ucsd.edu
Kelli L. Cain, Department of Psychology San Diego State University 3900 Fifth Avenue, Suite 310 San Diego, CA 92103 USA kcain@projects.sdsu.edu
Abby C. King, Dept. of Health Research & Policy and Stanford Prevention Research Center, Dept. of Medicine Stanford University School of Medicine 259 Campus Drive HRP Redwood Building, T221 Stanford, CA 94305-5405 king@stanford.edu
References
- Abercrombie LC, et al. Income and racial disparities in access to public parks and private recreation facilities. Am. J. Prev. Med. 2008;34:9–15. doi: 10.1016/j.amepre.2007.09.030. [DOI] [PubMed] [Google Scholar]
- Bors P, et al. The Active Living by Design National Program. Am. J. Prev. Med. 2009;37:S313–S321. doi: 10.1016/j.amepre.2009.09.027. [DOI] [PubMed] [Google Scholar]
- Buman MP, et al. Objective light-intensity physical activity associations with rated health in older adults. Am. J. Epidemiol. Online. 2010 doi: 10.1093/aje/kwq249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson JA, et al. Brief Physical Activity-Related Psychosocial Measures: Reliability and Construct Validity. J. Phys. Act. Health. doi: 10.1123/jpah.9.8.1178. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerin E, et al. Recreational facilities and leisure-time physical activity: An analysis of moderators and self-efficacy as a mediator. Health Psychol. 2008;27:S126–S135. doi: 10.1037/0278-6133.27.2(Suppl.).S126. [DOI] [PubMed] [Google Scholar]
- Clarke P, Nieuwenhuijsen ER. Environment for the Healthy Ageing: A Critical Review. Maturitas. 2009;64:14–19. doi: 10.1016/j.maturitas.2009.07.011. [DOI] [PubMed] [Google Scholar]
- Frank LD, et al. Healthy aging and where you live: Community design relationships with physical activity and body weight in older Americans. J. Phys. Act. Health. 2010a;7:S82–S90. doi: 10.1123/jpah.7.s1.s82. [DOI] [PubMed] [Google Scholar]
- Frank LD, et al. The development of a walkability index: application to the Neighborhood Quality of Life Study. Br. J. Sports Med. 2010b;43:124–131. doi: 10.1136/bjsm.2009.058701. [DOI] [PubMed] [Google Scholar]
- Freedson PS, et al. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sport Exerc. 1998;30:777–781. doi: 10.1097/00005768-199805000-00021. [DOI] [PubMed] [Google Scholar]
- Giles-Corti B, Donovan RJ. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med. 2002;54:1793–1812. doi: 10.1016/s0277-9536(01)00150-2. [DOI] [PubMed] [Google Scholar]
- Giles-Corti B, Donovan RJ. Relative influences of individual, social environmental, and physical environmental correlates of walking. Am. J. Public. Health. 2003;93:1583–1589. doi: 10.2105/ajph.93.9.1583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giles-Corti B, et al. Understanding physical activity environmental correlates: increased specificity for ecological models. Exerc. Sport Sci. Rev. 2005;33:175–181. doi: 10.1097/00003677-200510000-00005. [DOI] [PubMed] [Google Scholar]
- Hall KS, McAuley E. Individual, social environmental and physical environmental barriers to achieving 10,000 steps per day among older women. Health Educ. Res. 2010;25:478–488. doi: 10.1093/her/cyq019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joseph A, et al. Presences and visibility of outdoor and indoor physical activity features and participation in physical activity among older adults in retirement communities. J. Hous. Elderly. 2005;19:2–32. [Google Scholar]
- Kahn EB, et al. The effectiveness of interventions to increase physical activity. Am. J. Prev. Med. 2002;22:73–107. doi: 10.1016/s0749-3797(02)00434-8. [DOI] [PubMed] [Google Scholar]
- King AC, et al. Physical activity interventions targeting older adults: A critical review and recommendations. Am. J. Prev. Med. 1998;15:316–333. doi: 10.1016/s0749-3797(98)00085-3. [DOI] [PubMed] [Google Scholar]
- King AC, et al. Aging in Neighborhoods Differing in Walkability and Income: Associations with Physical Activity and Obesity in Older Adults. Under review. [DOI] [PMC free article] [PubMed]
- Marcus BH, Rakowski W, Rossi JS. Assessing motivational readiness and decision making for exercise. Health Psychol. 1992;11:257–261. doi: 10.1037//0278-6133.11.4.257. [DOI] [PubMed] [Google Scholar]
- Marcus BH, et al. Physical activity intervention studies: What we know and what we need to know. A scientific statement from the American Heart Association Council on nutrition, physical activity, and metabolism (Subcommittee on Physical Activity); Council on Cardiovascular Disease in the Young; and the Interdisciplinary Working Group on Quality of Care and Outcomes Research. 2006 doi: 10.1161/CIRCULATIONAHA.106.179683. Available at http://www.circulationaha.org. [DOI] [PubMed]
- McLeroy KR, et al. An ecological perspective on health promotion programs. Health Educ. Behav. 1988;15:351–377. doi: 10.1177/109019818801500401. [DOI] [PubMed] [Google Scholar]
- Miller NE, et al. Estimating absolute and relative physical activity intensity across age via accelerometry in adults. J. Aging Phys. Act. 2010;18:158–170. doi: 10.1123/japa.18.2.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson ME, et al. Physical activity and public health in older adults. Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1435–1445. doi: 10.1161/CIRCULATIONAHA.107.185650. [DOI] [PubMed] [Google Scholar]
- Pruitt LA, et al. Use of accelerometry to measure physical activity in older adults at risk for mobility disability. J. Aging Phys. Act. 2008;16:416–434. doi: 10.1123/japa.16.4.416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhodes RE, et al. Integrating the perceived neighborhood environment and the theory of planned behavior when predicting walking in a Canadian adult sample. Am. J. Health Promot. 2006;21:110–118. doi: 10.4278/0890-1171-21.2.110. [DOI] [PubMed] [Google Scholar]
- Saelens BE, et al. Environmental correlates of walking and cycling: Findings from the transportation, urban design, and planning literatures. Ann. Behav. Med. 2003a;25:80–91. doi: 10.1207/S15324796ABM2502_03. [DOI] [PubMed] [Google Scholar]
- Saelens BE, et al. Neighborhood-based differences in physical activity: an environment scale evaluation. Am. J. Public Health. 2003b;93:1552–1558. doi: 10.2105/ajph.93.9.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallis JF, et al. The development of scales to measure social support for diet and exercise behaviors. Prev. Med. 1987;16:825–836. doi: 10.1016/0091-7435(87)90022-3. [DOI] [PubMed] [Google Scholar]
- Sallis JF, et al. An ecological approach to creating more physically active communities. Annu. Rev. Publ. Health. 2006;27:297–322. doi: 10.1146/annurev.publhealth.27.021405.102100. [DOI] [PubMed] [Google Scholar]
- Sallis JF, et al. Rimer BK. In: Ecological models of health behavior, in Health behavior and health education: Theory, research and practice. 4th Edition Glanz K, Viswanath K, editors. Josey-Bass; San Francisco CA: 2008. [Google Scholar]
- Samuels SE, et al. The California Endowment’s health eating, active communities program. A midpoint review. Am. J. Public Health. 2010;100:2114–2123. doi: 10.2105/AJPH.2010.192781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart AL, et al. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Med. Sci. Sport Exerc. 2001;33:1126–1141. doi: 10.1097/00005768-200107000-00010. [DOI] [PubMed] [Google Scholar]
- Stokols D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996;10:282–298. doi: 10.4278/0890-1171-10.4.282. [DOI] [PubMed] [Google Scholar]
- Troiano RP, et al. Physical activity in the United States measured by accelerometer. Med. Sci. Sport Exerc. 2008;40:181–180. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- Trost SG, et al. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sport Exerc. 2002;34:1996–2001. doi: 10.1097/00005768-200212000-00020. [DOI] [PubMed] [Google Scholar]
- US Department of Health and Human Services USDHHS physical activity guidelines for Americans. 2008 http://www.health.gov/paguidelines Web site. Updated 2008.
- van Cauwenberg J, et al. Relationship between the physical environment and physical activity in older adults: a systematic review. Health Place. 2010;17:458–469. doi: 10.1016/j.healthplace.2010.11.010. [DOI] [PubMed] [Google Scholar]
- Yen IH, et al. Neighborhood environment in studies of health of older adults: A systematic review. Am. J. Prev. Med. 2009;37:455–463. doi: 10.1016/j.amepre.2009.06.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.