

Abstract
Pancha karma is a modality of treatments commonly used in Ayurvedic hospitals. It has elaborate textual reference of its usage in various clinical conditions forming the basis of its extensive use in Ayurvedic clinical practice. Unfortunately, despite its unquestionable popularity and usage among Ayurvedic physicians and patients, it has not been evaluated rigorously on scientific parameters to identify its effectiveness, safety, and procedural standards. Considering the patient's opinion as an important determinant in this perspective, this study aims at identifying the patient's (actual recipients of pancha karma therapy) perception toward the effectiveness, safety, and standard of service delivery concerning pancha karma through a structured survey at a pre-identified pancha karma therapy unit in a secondary care Ayurvedic hospital. Majority of the survey respondents considered these therapies as safe and effective (88%). Ninety-four percent respondents have expressed their satisfaction to the standard of services provided to them at the pancha karma unit of the hospital concerned.
Keywords: Effectiveness, pancha karma, safety
INTRODUCTION
Pancha karma is one of the most trusted and utilized package of therapies seen in practice at Ayurvedic hospitals in India.[1]
Composed of a definitive pre-, peri- and posttreatment protocol, pancha karma is composed of five interventions (pancha meaning five, and karma meaning procedure) aiming at cleaning the body of the disease-causing milieu and hence rendering it instantly disease free or more cleaned and apt to further medications offered to cure such an illness.[2] Tracing its origin to the classical textual triad of Ayurveda (Charaka, Sushruta and Vagbhata Samhita), pancha karma has a history of many thousand years of uninterrupted practice. Being a part of samsodhana (correction through elimination) type of Ayurvedic therapeutics, pancha karma is considered superior to samsaman (correction through rebalance) therapies, for its potential of eradicating the disease completely and minimizing the chances of recurrences.[3]
Despite its historical precedence and practice, there are meager evidences proving the effectiveness, safety, and standard operative procedures (SOPs) of pancha karma under various clinical conditions. The effectiveness of pancha karma has been poorly evaluated in terms of its primary and secondary outcomes, treatment endpoints, and procedural standards. In the lack of definitive evidences, an advocacy of pancha karma as a dependable form of Ayurvedic therapeutics under various clinical conditions is questioned. In a literary search made at Pubmed and Google scholar, besides individual case reports, case series, and pilot and pragmatic trials,[4–9] we did not come across any of study which intends to identify a real-time patient's perception about pancha karma therapy on account of its effectiveness, safety, and procedural standards. Patients’ own preference and perception has been considered an important determinant to judge about the ultimate effectiveness of any intervention. This is more applicable in cases of integrated medicine or traditional medicine where a patient's previous experience, a cultural belief, and anecdotal claims play an important role in determining the net outcome of a given intervention.[10] This study is planned therefore to fill this observational gap by generating a real-time patient-centered perception and preference-based data about various aspects of pancha karma. Such data generation through observational studies is presumed crucial to identify the focus of research needs, design, plan, and implementation required for the optimal utilization of pancha karma in the coming future.
MATERIALS AND METHODS
A patient-based survey to identify the perceived efficacy, safety and standard of service delivery referring to pancha karma was conducted with the help of a formatted questionnaire. The questionnaire consisted of distinct components about the effectiveness, safety, and standard of service delivery in pancha karma therapy offered at a unit of pancha karma at a secondary care Ayurvedic hospital (please see the Appendix). The study however does not intend to use these terms in a strict scientific definition but uses them to identify the patient's perception around these terms and procedural standards are considered. Here, ‘Satisfaction’ is rating by the patient for the procedure, ‘safety’ is nonobservance of any specific discomfort during, before, or after the procedure, and ‘effectiveness’ is perceived benefits experienced after the procedures.
Participants of the survey were randomly selected from patients visiting the pancha karma unit of the hospital for their therapy during working hours and days during years 2009–2010. Participant's selection was devoid of any sex, age, and disease or procedure bias. In the case of minors being taken up for the survey, their parents’ consent was taken.
The survey was conducted at State Ayurvedic College and Hospital, Lucknow, Uttar Pradesh, India. This hospital is one of the largest secondary care Ayurvedic hospitals in the northern region of India. The hospital has a fully functional pancha karma unit with approximately 22,000–26,000 treatment enrollments in a year.
The survey was conducted through a one-to-one interview method where patients were asked to respond against given replies to specified questions on the effectiveness, safety, or quality of the pancha karma services they were receiving. As the survey is patient perception based, it is devoid of any objective to prove the efficacy of pancha karma procedures under a clinical condition through objective evaluations of physiopathological changes consequential to the treatment. Data observed through the survey were analyzed statistically to identify the gross trends of patients’ perception about the effectiveness, safety, and quality of pancha karma services offered to them.
RESULTS
A total of 160 patients were recruited for the survey. Among them, 10 could not complete the questionnaire and thereby only 150 completed responses were compiled to enter into data analysis.
Among the total registered patients, 60% (90) were females and 40% (60) were males. Participants’ age ranged between 4 and 65 years with a mean of 36 years. The mean duration of pancha karma therapy received by participants was 12 days with a range of 2–46 days.
Effectiveness
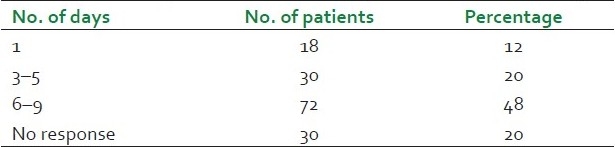
Upon enquiring about the efficacy experience of the procedures, 60% of participants found it better than their expectations whereas 19% found it below their expectations [Table 1]. Eighty percent participants however had expected even better effects from the therapy in the due course of time. An enquiry about effectiveness has shown 88% participants rating the therapy as high to moderately effective. Among surveyed patients, 80% have reported a relief of symptoms in a period of 1–9 days. The maximum response however was seen during 6–9 days (48% ; Table 2). Upon enquiring about the daily cost of pancha karma therapy, approximately 54% patients have reported it less than Rs. 100 for every day pancha karma therapy.
Table 1.
Rating pancha karma therapy effectiveness on the level of expectations
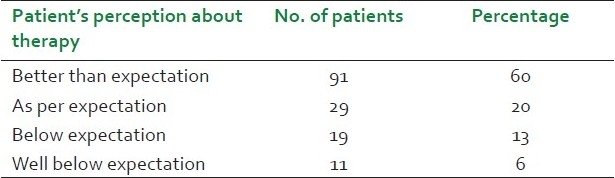
Table 2.
Response to therapy in treatment days
Safety
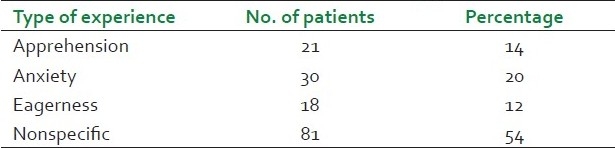
Fifty-four participants reported a nonspecific feeling before they received the pancha karma therapy. A small fraction of patients also reported feelings like apprehension (14%), anxiety (20%), and eagerness (12%; Table 3). None of the participants have reported any procedure-related problem during the therapy session. A minor fraction of patients (6%) have reported hypertension as a postprocedure complaint.
Table 3.
Experience before therapy
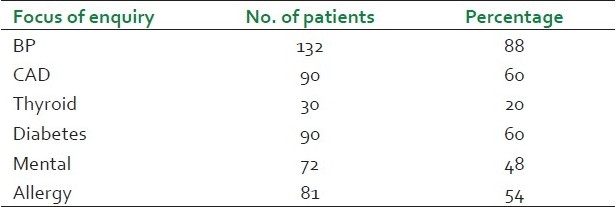
A total of 88% (132) participants have reported that they were enquired about their blood pressure before the treatment was given. Enquiries were narrowly followed by questions about diabetes (60%) and coronary artery disease (60%) [Table 4]. Only 68% (102) patients have reported to be provided with any specific instruction pertaining to these enquiries.
Table 4.
Pretreatment enquires made
Standard of service delivery
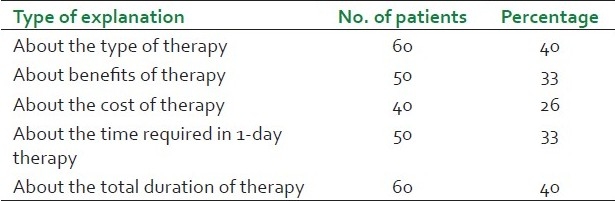
An enquiry was made against the preprocedural explanations given to patients [Table 5]. A total of 40% participants have reported to be explained about the type of therapy, 33% about expected benefits of the therapy, 26% about the expected cost of the therapy, 33% about the time required in 1-day therapy, and 40% have reported to be explained about the total duration of therapy. Interestingly, approximately 66% participants have reported that the explanations are given by trainee students and not by the consultants in the unit.
Table 5.
Pretreatment explanations to patients
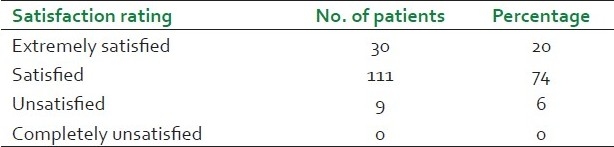
A total of 79% respondents have reported a consumption of less than 2 h in their daily therapy whereas 20% reported that more than 2 h were required in their daily therapy. Interestingly, 66% of the total respondents accepted that out of the total time consumed in their daily therapy, and the maximum share was taken by “waiting for their turn”[Tables 6 and 7]. A total of 66% respondents were satisfied with the cleanliness of the unit whereas 86% respondents were satisfied with the staff behavior [Tables 8 and 9]. Fifty-three percent respondents reported that facilities to maintain female privacy were grossly inadequate in the unit. Approximately, 66% participants reported to be refused the therapy even when they arrived at the unit. In 71% cases, this refusal was attributed to a mechanical breakdown [Tables 10 and 11]. This is important to observe that no respondent reported any such refusal on account of staff unavailability or due to their late arrival at the unit. Ninety-four percent respondents expressed their satisfaction to the services provided at the pancha karma unit at this particular hospital [Table 12].
Table 6.
Average time consumed in daily therapy

Table 7.
Activity in which the highest proportion of time was consumed

Table 8.
Cleanliness of the unit
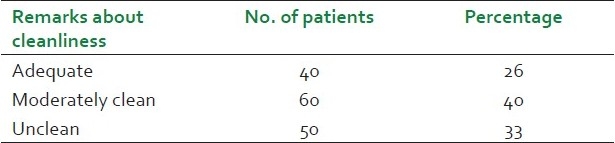
Table 9.
Rating of staff behavior

Table 10.
Number of patients refused to be provided with therapy after their arrival at unit
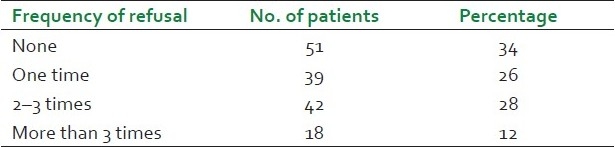
Table 11.
Cause of refusal
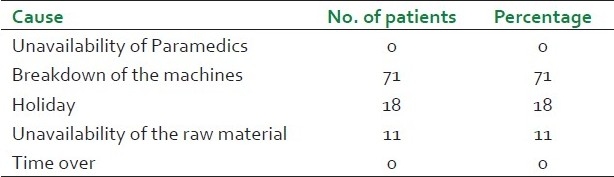
Table 12.
Overall satisfaction
DISCUSSION
In a conventional, medical decision-making model, a patient rarely comes into the scene beyond the level of getting informed of the proposed interventions for the purpose of obtaining an informed consent. Do patients’ own belief, cultural context, and preferences play any role in determining the net outcomes of a therapeutic intervention? Contrary to the conventional medicine where lifetime interventional decisions about patients are made in context to randomized controlled trials (RCTs) who often fail to prove their external validity,[11] decisions in complementary and alternative medicine (CAM) are invariably influenced by factors affecting the real life may it be the patient's own preference, perception, or belief. Unfortunately, despite their huge and perceptible influences upon decision making and thereby upon ultimate outcomes, patients’ perspectives are rarely given importance in clinical trials of CAM. Taking the example of pancha karma in this study, we can clearly notice that among 80% of the participants, the responses obtained through therapy were either in concordance or even better than the preconceived expectations. This clearly points out the impact of a mindset upon the net outcome in a given intervention. Efficacy and effectiveness are two different observations which need to be clarified in reference to CAM. Efficacy is the absolute therapeutic effect of a regime which can be observed in an ideal controlled situation as is often created in RCTs. This controlled situation is however beyond the visibility in real clinical situations where one has to find pragmatic solutions to complex clinical situations often mixed with a social–economical–cultural matrix. Efficacy observations of a strictly controlled experimental design thereby often need to be diluted to effectiveness assessments where the assessments are evaluated in reference to the real-life contexts. For its inherent complexity of decision making and applications, an effectiveness research seems more apt to CAM compared to the efficacy as is observed in conventional medicine. There have been various works done to delineate the comparative effectiveness, cost effectiveness, and overall effectiveness of CAM approaches of healthcare;[12–14] however, none have focused upon the issues specific to Ayurveda.
Observational studies play a key role in determining the effectiveness of a given regime in a particular situation. Without framing the outcomes into fixed primary or secondary judgmental endpoints, it gives us an idea about the overall effects of the intervention. Needless to say, in CAM, most important ones among these effects are the feeling of well-being, improved physiological and vital status, and a better tolerance of symptoms. Patients’ own perception about effectiveness, safety, and quality of the services offered to them could possibly be the strongest evidence to make a judgment against these variables. For its invaluable importance, a patient's opinion can be utilized as a compulsive argument to prove or to disprove the significance of an intervention under a given condition. For these many reasons, the undertaken study gives us opportunities to think beyond the conventional frame of efficacy as is conceived under the RCT model. The study gives us valuable opinion pieces about the effectiveness, safety and quality of services offered in pancha karma in a particular setting. Its high effectiveness rating (88%), low cost, minimal risk, and satisfactory delivery makes it a persona grata among various interventions often practiced in Ayurveda. The study however has many limitations. It does not address the effectiveness in reference to a particular type of the procedure in pancha karma. We have learned that it is snehana and swedana which are most commonly practiced in pancha karma units, and observations seem to reflect the responses obtained by these therapies alone and not by a comprehensive pancha karma.[1] For being conducted at one setting only, possibilities of procedural variations which may affect the effectiveness observation cannot be ruled out. Moreover, as the observations are not made in reference to specific diseases, this is difficult to frame the effectiveness of pancha karma in a particular clinical condition. A patient's bias in choosing the responses in pursuit of obtaining more benefits from the therapy as well as from the center cannot be ruled out from the study. The educational background of the patient and his awareness about the procedures can also be influential in a response choice. Randomization and third party (those not involved in giving the treatment) evaluation would possibly have added more objectivity to the study. There are potential possibilities of strengthening such instruments in reference to their construct and content validity, if they could be assisted with experts in other disciplines – social sciences, economics, statistics, and psychologists.
A few more points as observed in the study deserve to be mentioned here. Procedural explanations are found attempted by trainees mostly in the studied hospital. Due to their less experience and enthusiasm, an overprojection of pancha karma in reference to its procedural details or expected benefits cannot be ruled out. Moreover, the noninvolvement of the senior consultants in the department in the process of explanation underlines an institutional deficit. The identification of “waiting for their turn” as one major component of the total time consumed in pancha karma procedures further explains a poor resource–patient ratio at the particular center. How the patient's stay can be reduced in the hospital without compromising with the services provided to them is a serious aspect which adds to the quality of the hospital. A gross inadequacy of female privacy is the issue which may ultimately affect the net outcomes of an intervention. If patients are not finding themselves comfortable during the treatment or during the process of preparing for the treatment, they may remain stressed which is going to affect the outcomes negatively. This issue may be particularly true with female patients. The refusal of services on account of a mechanical breakdown points out poor equipment maintenance services exercised in the hospital. A thorough record-keeping of the equipments and a regular maintenance check could have prevented such breakdowns and resulting sufferings to the services provided to patients.
Finally, the questionnaire used in the study is also found linked with certain construct and content issues which might have affected the net response of the survey. Individual items used in the questionnaire could have been clearer in their construct in order to express what they actually intend. Despite these limitations, the study gives us a valuable opinion piece that pancha karma in general is well accepted in the community on account of the effectiveness, safety, and quality of the services delivered.
National Accreditation Board for Hospitals and Healthcare Providers (NABH) has recently brought Ayush hospitals and wellness centers also under its ambit. It has issued a detailed guideline in reference to various aspects of services offered in an Ayush hospital in order to acquire a NABH certification.[15] The present study, by providing a patient's perception and expectation in reference to panch karma services in an Ayush hospital, may help making these guidelines more pragmatic and closer to the real-life situation. This study would further help us identify the gaps between the “perceived” and the “practiced” standard of pancha karma procedures when the same evaluated in light of set procedural standards as are elaborated in classical texts of Ayurveda.[16]
APPENDICES
Survey format for evaluating the efficacy, safety, and standard of the delivery of pancha karma procedures through a pilot survey of recipient's (patient's) opinion at a pancha karma unit in an Ayurvedic teaching hospital
A. EVALUATION OF EFFECTIVENESS
-
I perceive the pancha karma procedure which I am experiencing as
- Highly effective
- Moderatelyeffective
- Minimally effective
- Not effective
-
This opinion is based upon following observations (please write the symptoms and level of their grade before therapy and also on the day of survey)
-
My observations are verifiable/not verifiable through objective changes to the following signs (please mention about the sign, their status before therapy and also on the day of survey)
-
My observations are verifiable/not verifiable through objective changes to the following investigations (please mention about the investigation, their value before therapy, and also on the day of survey)

-
Responses to the therapy were observable to me after
- First therapy day
- 3–5 therapy days
- 6–9 therapy days
- Not observed so far
-
Actual per day cost of the therapy comes to me as
- Less than Rs.100/-
- Less than Rs. 300/-
- More than Rs. 300/-
-
Highest proportion of this cost is incurred for
- Transportation
- Medicine used during the therapy
- Medicine and special care advised following the therapy
-
At your expectation rating, responses observed during the therapy are (please mark the best suitable option)
- Better than expectation
- As per expectation
- Below expectation
- Well below expectation
-
Do you wish to continue the therapy. If yes, then which is the most appropriate reason to explain this continuation?
- Receiving benefit and expect some more
- Not receiving benefits but expect some after continuation
- There are no other remedies available
- Other treatments are not affordable
-
Would you like to recommend pancha karma therapy to your family and friends?
- Definitely yes
- Yes
- Can’t say
- No
-
Have you been explained (by your referring physician or the pancha karma physician) about the expected benefits of therapy and possible number of therapy days to have the observable effects?
- Yes and in explicit details
- Yes but incomprehensible
- No
B. EVALUATION OF SAFETY
-
Have you been explained (by your referring physician or by treating physician) about the possible safety precautions before the procedures are performed?
- Yes and in explicit details
- Yes but incomprehensibly
- No
-
Have you been enquired about following before the actual procedures are performed?
-
Did you receive any specific instruction in reference to these enquiries before the actual procedures are performed?
- Yes
- No
- Don’t know
If yes, can you name few of these specific instructions given to you?
-
What was your experience just before you received the pancha karma therapy for the first time?
- Apprehension
- Anxiety
- Eagerness
- Nonspecific feelings
Did you experience any problem during the procedure any day? If yes, please mention it (Please mention the exact nature of the problem and its time of occurrence)
-
What was the severity of the problem?
- Severe
- Moderate
- Mild
-
While receiving the treatment, how frequently this problem was observed?
- Experienced once
- Experienced more than once
- Experience every time
Did you experience any problem after the procedure any day? If yes, please mention it (Please mention the exact nature of the problem and its time of occurrence)
-
How common “After the procedure problem” is
- Experienced once
- Experienced more than once
- Experience every time
-
In your opinion, is this problem associated with pancha karma procedure which is advised for you?
- Definitely yes
- Yes
- Don’t know
- No
-
Did you notify these problems to your treating physician/paramedics
- Yes
- No
-
How the physician/paramedics reacted once you notified your problems during to the procedure?
- Stopped the treatment
- Stopped the treatment and advised to have a reexamination before the restart of the therapy
- Modified the therapy suitably
- Did not take any action
-
Were you satisfied with the action taken in your case?
- Yes and completely
- Yes but partially
- No
C. EVALUATION OF STANDARD OF DELIVERY OF PROCEDURES
-
Have you been explained by your physician about the following before you actually received the treatment
-
After being referred to pancha karma therapy from OPD, how was your way to the pancha karma unit?
- Easy
- With moderate difficulty
- With much difficulty
-
What were the major difficulties you experienced to reach the pancha karma unit?
-
Is there any formal registration/enquiry system in the pancha karma unit to deal with new arrivals?
- Yes
- No
- don’t know
-
What is the usual procedure to get treatment in this pancha karma unit (in your opinion)?
- First come first serve
- Making acquaintance with paramedics
- Get registered and wait till your turn comes
-
Did you get reexamined/enquired for your problems before you actually receive the treatment for the first time
- Yes
- No
-
If yes, who enquired about your problems?
- Physician
- Paramedic who is actually doing the procedure
- Under training students
-
From your arrival at a pancha karma unit till you finish with your treatment on a single day, how much time does it take? (On average)
- Less than 1 hour
- 1–2 hour
- More than 2 hours
-
Can you mark the following in order of their time consumption ratio in your case (mark 1 for most time consuming followed by 2, 3, 4 for less time consuming ones)
- Waiting for the turn
- Preparation of the procedure
- Actual procedure
- After procedure
-
What is your opinion about the waiting area with reference to the space and comfort?
- Adequate
- Moderately inadequate
- Severely inadequate
-
What is your opinion about the general cleanliness of the unit?
- Adequately clean
- Moderately clean
- Unclean
- Severely unclean
-
What is your opinion about the general cleanliness of the paramedics in the unit?
- Adequately clean
- Moderately clean
- Unclean
- Severely unclean
-
What are you ratings about the behavior and approach of paramedics in the unit?
- Extremely satisfactory
- Satisfactory
- Unsatisfactory
- Completely unsatisfactory
-
Is there enough provision to maintain privacy of the female patients receiving treatment?
- Yes
- No
- Don’t know
-
Is there any availability and accessibility of changing rooms/pretreatment room to change the cloth before you receive the therapy?
- Yes
- No
- Don’t know
-
Is there any availability and accessibility to postprocedure rest rooms to avoid instant exposure of environment just after the therapy?
- Yes
- No
- Don’t know
-
Have you been refused to be provided with therapy some day despite your arrival in time? If yes, how often this happened?
- Once
- More than once
- More than three times
-
When refused, what was the assigned reason of nonavailability of treatment?
- Unavailability of paramedics
- Holiday
- Breakdown of the apparatus of the procedure
- Unavailability of the raw material
- Time finished
-
Do you feel that the paramedics in pancha karma do better if you oblige them with cash or kind?
- Yes
- No
- Don’t know
-
How do you rate the delivery of the pancha karma procedure in this pancha karma unit?
- Extremely satisfactory
- Satisfactory
- Unsatisfactory
- Completely unsatisfactory
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Rastogi S. Pancha karma: Exploring through evidences. Light on Ayurveda Journal. 2011;9:30–6. [Google Scholar]
- 2.Singh RH, Rastogi S. Vol. 2. Pondicherry, India: 1994. Molecular basis of samsodana effect in Panca karma therapy; New Approaches Med Health; pp. 35–41. (translated and published in Italian language in Empedocle, 1(12) No2, 1994 p 3-10. [Google Scholar]
- 3.Tripathi BN, editor. Varanasi, India: Chaukhambha prakashana; 2008. Charak Samhita sutra sthan. [Google Scholar]
- 4.Rastogi S, Singh RH. Duchennes muscular dystrophy-management through pinda sweda therapy. Journal of Research in Ayurveda and Siddha. 1996;17:105–11. [Google Scholar]
- 5.Rastogi S, Alias A. Management of chronic venous insufficiency with hydrotherapy. Cardiology Today. 2001;5:244. [Google Scholar]
- 6.Rastogi S, Ranjana, Rastogi R. Jala Neti application in acute rhino sinusitis. Indian J Tradit Knowl. 2007;6:328–33. [Google Scholar]
- 7.Rastogi S. CAM management of Peripheral Arterial occlusive disease (PAOD): A Case Report. Complement Health Pract Rev. 2008;13:198–203. [Google Scholar]
- 8.Rastogi S, Chawla S, Singh RK. Ayurvedic management of unilateral loss of vision following a blunt injury to eye: A case report. Complement Health Pract Rev. 2009;14:84–92. [Google Scholar]
- 9.Basler AJ. Pilot Study Investigating the Effects of Ayurvedic Abhyanga Massage on Subjective Stress Experience. J Altern Complement Med. 2011;17:435–40. doi: 10.1089/acm.2010.0281. [DOI] [PubMed] [Google Scholar]
- 10.Shannon S, Weil A, Kaplan BJ. Medical decision making in integrative medicine: Safety, efficacy and patient preference. Altern Complem Ther. 2011;17:84–91. [Google Scholar]
- 11.Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342:1887–92. doi: 10.1056/NEJM200006223422507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Herman PM, Craig BM, Caspi O. Is complementary and alternative medicine (CAM) cost-effective? A systematic review. BMC Complement Altern Med. 2005;5:11. doi: 10.1186/1472-6882-5-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ventegodt S, Andersen NJ, Kandel I, Merrick J. Comparative analysis of cost-effectiveness of non-drug medicine (nonpharmaceutical,holistic, complementary and alternative medicine/CAM) and biomedicine (pharmaceutical drugs) for all clinical conditions. Int J Disabil Hum Dev. 2009;8:243–58. [Google Scholar]
- 14.Aickin M. Comparative effectiveness research and CAM. J Altern Complement Med. 2010;16:1–2. doi: 10.1089/acm.2009.0718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Accreditation program for Ayush Hospitals. [Last accessed on 2011 June 27]. Available from: http://www.qcin.org/nabh/iapah/
- 16.Guidelines on basic training and safety in Pancha Karma (2008) [Last accessed on 2011 June 27]. Available from: http://www.ccras.nic.in/Training_Modules/20081103_Panchakarma.htm .