

To the editor:
In a recent article in Molecular Therapy, Hogarty1 elucidated the still unresolved issue regarding the role of interleukin-17A (IL-17A) in the pathogenesis of Langerhans cell histiocytosis (LCH) and whether serum IL-17A could be used as a systemic biomarker of the disease. In the same article, it was stated that the “IL-17A issue,” beyond its academic interest, has definite therapeutic implications, given that IL-17A-targeted treatments are now in preclinical development for LCH. Therefore, clear conclusions are urgently required that can be obtained only through collective work.
LCH is a rare disease of obscure etiology, involving single or multiple systems of the human body. Although all lesions share common histopathological features, LCH has an unpredictable clinical course ranging from spontaneous resolution to disseminated disease, compromising vital functions with occasionally fatal consequences. It is characterized by the clonal accumulation and/or proliferation of specific dendritic cells that resemble the normal epidermal Langerhans cell; however, there is ongoing debate over whether the origin of the disease is immunological or neoplastic.
IL-17, also known as IL-17A and cytotoxic T lymphocyte–associated antigen 8 (CTLA-8), is a T cell–specific proinflammatory cytokine involved in chronic inflammatory states presenting with granuloma formation and also in bone resorption through RANKL induction in osteoblasts.2 Histological features of LCH resembling granulomas, as well as osteolytic bone lesions of the disease, provide indications of a possible central role of IL-17A in LCH pathogenesis. Recently, Coury et al. implicated IL-17A, favoring the immune etiology of LCH.3 These authors demonstrated increased serum IL-17A concentrations in 13 subjects (2 adults) at various stages of LCH (12 patients with multiple-system disease; all patients had received several chemoimmunotherapy treatments).3 They also suggested that IL-17A was originating from the dendritic cells rather than the T cells, and, although total serum IL-17A concentrations did not correlate with the activity of the disease, serum IL-17A-dependent fusion activity did correlate with the activity of LCH.3
On the basis of these findings, a potential IL-17A-targeted therapy was proposed as a future therapeutic approach in LCH, whereas IL-17A appeared as a possible biomarker to monitor disease activity. Therefore, and according to these findings, IL-17A-targeted treatments, which are currently in phase I and phase II trials for other inflammatory conditions, are also considered in LCH.1 However, another research group was unable to identify any IL-17A messenger RNA expression in 12 lesions from 10 pediatric patients with LCH.4 Peters et al. studied plasma samples from 26 LCH patients with active disease and 46 pediatric control subjects and reported IL-17A at background levels in LCH patients at concentrations consistent with controls in two different standard enzyme-linked immunosorbent assay (ELISA) kits. In addition, IL-17A concentrations of both patients and controls were highly variable according to the development ELISA kit utilized in the study by Coury et al.3 Moreover, the principal antibody employed by Coury et al. cross-reacted with protein lysate from LCH lesions. Therefore, it was suggested that the lack of identifiable IL-17A transcripts or protein expression in the lesions precludes the possibility of lesional IL-17A production and subsequent autocrine and/or paracrine action.1
LCH is rarer in adults than in children, with an estimated annual incidence of 1 case per 560,000 inhabitants, and it is therefore regarded as an “orphan disease.”5 In our recent study of 25 adults with LCH at various disease stages who had previously received a variety of treatments, we found decreased bone mineral density as well as decreased bone turnover in those treated with chemotherapy or glucocorticoids or both.6 In the same patients, we have now measured serum IL-17A concentrations in duplicates (standard deviation and coefficient of variation values of 5.9 and 4.7%, respectively) using one of the three commercial kits employed in the study by Peters et al. (Human IL-17 Quantikine ELISA kit, D1700; R&D Systems Europe, Abingdon, UK). No differences were found between those 25 patients and 50 age-, sex-, and body mass index–matched controls (patients, 154 ± 19 pg/ml vs. controls, 132 ± 16 pg/ml; Mann-Whitney test, P = 0.144), as well as no association between LCH activity and serum levels of IL-17A. These differences remained nonsignificant after exclusion of the two apparently healthy controls with high IL-17 values (outliers, Figure 1) (patients 154 ± 19 pg/ml vs. controls, 115 ± 10 pg/ml; Mann-Whitney test, P = 0.072).
Figure 1.
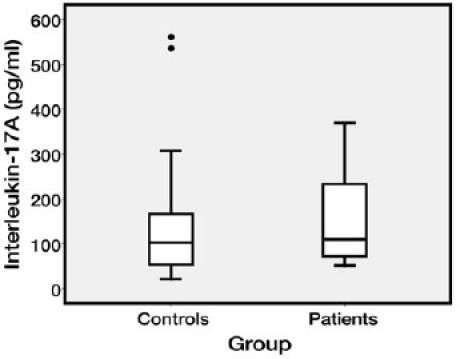
Interleukin-17A levels in patients and controls.
From our findings, it seems that serum IL-17A is not ubiquitously increased among LCH patients with active disease. Multicenter studies with large numbers of patients are needed to define whether several parameters such as age (adults vs. children), disease extension and involvement, and treatment administered can influence IL-17A. Our findings are in agreement with those from the previous groups that failed to demonstrate a correlation between IL-17A concentrations and disease activity, and they suggest that serum IL-17A cannot serve as a biomarker to differentiate patients with LCH and active disease or indicate those who might benefit from an IL-17A-targeted therapeutic approach.
REFERENCES
- Hogarty MD. IL-17A in LCH: systemic biomarker, local factor, or none of the above. Mol Ther. 2011;19:1405–1406. doi: 10.1038/mt.2011.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sato K, Suematsu A, Okamoto K, Yamaguchi A, Morishita Y, Kadono Y.et al. (2006Th17 functions as an osteoclastogenic helper T cell subset that links T cell activation and bone destruction J Exp Med 2032673–2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coury F, Annels N, Rivollier A, Olsson S, Santoro A, Speziani C.et al. (2008Langerhans cell histiocytosis reveals a new IL-17A-dependent pathway of dendritic cell fusion Nat Med 1481–87. [DOI] [PubMed] [Google Scholar]
- Peters TL, McClain KL., and, Allen CE. Neither IL-17A mRNA nor IL-17A protein are detectable in Langerhans cell histiocytosis lesions. Mol Ther. 2011;19:1433–1439. doi: 10.1038/mt.2011.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malpas JS. Langerhans cell histiocytosis in adults. Hematol Oncol Clin North Am. 1998;12:259–268. doi: 10.1016/s0889-8588(05)70509-8. [DOI] [PubMed] [Google Scholar]
- Makras P, Terpos E, Kanakis G, Papatheodorou A, Anastasilakis AD, Kokkoris P.et al. (2011Reduced bone mineral density in adult patients with Langerhans cell histiocytosis Pediatr Blood Cancere-pub ahead of print 11 May 2011. [DOI] [PubMed]