

1. DISEASE CHARACTERISTICS
1.1 Name of the disease (synonyms)
Cystinuria; currently two additional autosomal recessive contiguous cystinuria-associated syndromes in 2p21 are known: HCS and the 2p21 deletion syndrome.
1.2 OMIM# of the disease
Cystinuria: 220100, HCS: 606407.
1.3 Name of the analysed genes or DNA/chromosome segments
SLC3A1, SLC7A9, 2p21.
1.4 OMIM# of the gene(s)
SLC3A1: 104614,
SLC7A9: 604144.
1.5 Mutational spectrum
Point mutations, multiexon deletions and duplications, genomic rearrangements.1, 2, 3, 4, 5, 6, 7, 8
1.6 Analytical methods
Sanger sequencing of the total coding region and the exon–intron boundaries of the SLC3A1 and SLC7A9 genes. MLPA, qPCR and microarray typing for detection of multiexon and whole gene imbalances.
1.7 Analytical validation
All mutations identified have to be confirmed by a second, independent test (PCR, qPCR, sequencing, MLPA). The segregation of the mutation should be confirmed in the parents and further relatives. Pathogenicity of novel missense alterations has to be verified by testing a set of at least 100 control chromosomes of the same ethnic origin and by in-silico prediction methods. To confirm their pathogenic nature, splice site variants should be characterised by cDNA analysis.
1.8 Estimated frequency of the disease (incidence at birth (‘birth prevalence') or population prevalence)
Cystinuria: birth prevalence: 1:7000
(HCS/2p21 deletions: 1:1 000 000)
1.9 If applicable, prevalence in the ethnic group of investigated person
Cystinuria: 1:2500 in Jewish Israelis of Libyan origin, 1:100 000 in Sweden.
HCS: allele frequencies for the most common deletions in Belgium: 1:333–1:7700.9
1.10 Diagnostic setting
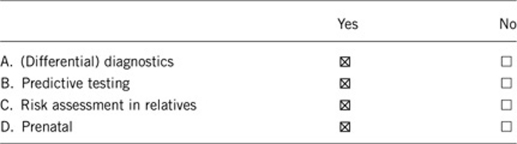
Comment:
Large genomic deletions in 2p21 include at least the SLC3A1 and PREPL genes; in the homozygote state the 2p21 deletion is associated with the hypotonia-cystinuria syndrome.
2. TEST CHARACTERISTICS
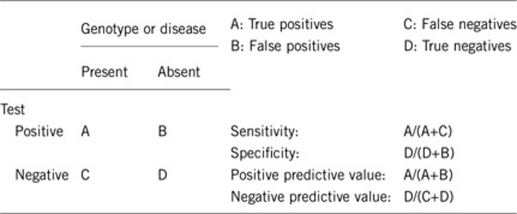
2.1 Analytical sensitivity (proportion of positive tests if the genotype is present)
Depending on the ethnic origin and the applied methods:
50–100%.
2.2 Analytical specificity (proportion of negative tests if the genotype is not present)
>98%.
2.3 Clinical sensitivity (proportion of positive tests if the disease is present)
The clinical sensitivity can be dependent on variable factors such as age or family history. In such cases a general statement should be given, even if a quantification can only be made case by case.
Depending on the ethnic origin and the applied methods:
50–100% (if the urinary excretion patterns revealed an increased cystine excretion).
2.4 Clinical specificity (proportion of negative tests if the disease is not present)
The clinical specificity can be dependent on variable factors such as age or family history. In such cases a general statement should be given, even if a quantification can only be made case by case.
>98%.
2.5 Positive clinical predictive value (life-time risk of developing the disease if the test is positive)
SLC3A1: increased urinary cystine excretion: 100%, kidney stone formation: 94%.
SLC7A9: increased urinary cystine excretion: 100%, kidney stone formation: 94%.
(in homozygotes or compound/mixed heterozygotes)
For SLC7A9 heterozygotes an increased urinary cystine excretion can be observed in 86–90% of cases and kidney stone formation in 2–18% of cases.
Polymorphisms of the SLC7A9 gene probably affect the clinical course in SLC7A9 mutation carriers.3
2.6 Negative clinical predictive value (probability not to develop the disease if the test is negative)
Assume an increased risk based on family history for a non-affected person. Allelic and locus heterogeneity may need to be considered.
Index case in that family had been tested:
>99%.
Index case in that family had not been tested:
Depending on the affected gene and the degree of relationship.
3. CLINICAL UTILITY
3.1 (Differential) diagnosis: the tested person is clinically affected
(To be answered if in 1.10 ‘A' was marked)
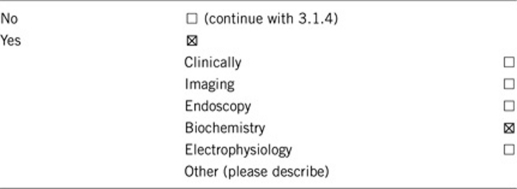
3.1.1 Can a diagnosis be made other than through a genetic test?
3.1.2 Describe the burden of alternative diagnostic methods to the patient?
In the majority of cases the initial diagnosis of cystinuria is achieved first by the identification of a cystine stone and then confirmed by biochemical or genetic data. Exception is the possible request of a diagnosis by siblings of affected subjects, who had not yet formed renal stones. In some situations, an increase in urinary cystine and dibasic amino acids exertion (on qualitative testing) does not allow a definite prognosis, because of the difficulty to differentiate between homozygotes (or compound heterozygotes) or heterozygotes. In these cases genetic testing might help to clarify the diagnosis. Alternatively, relatively low arginine and ornithine levels in heterozygotes in quantitative analysis of urine amino acids can also differentiate between the two.
3.1.3 How is the cost effectiveness of alternative diagnostic methods to be judged?
The cost effectiveness of biochemical and chemical urinary and stone analyses is very high.
3.1.4 Will disease management be influenced by the result of a genetic test?
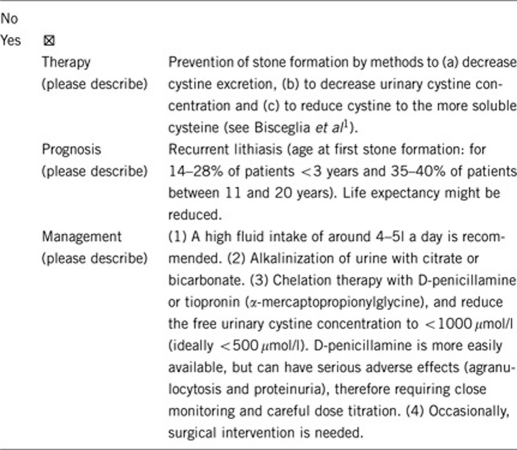
Patients with a preclinical diagnosis and therefore not yet formed renal stones, should not be treated with cystine-binding drugs (tiopronin or penicillamine). They should, however, be encouraged to drink water, particularly before going to sleep, to dilute urine overnight. The use of potassium citrate should also be discussed, at least in those patients with highest level of cystine.
3.2 Predictive setting: the tested person is clinically unaffected but carries an increased risk based on family history
(To be answered if in 1.10 ‘B' was marked)
3.2.1 Will the result of a genetic test influence lifestyle and prevention?
If the test result is positive (please describe):
Prevention of stone formation (see Bisceglia et al1) by dietary methods.
If the test result is negative (please describe):
No.
3.2.2 Which options in view of lifestyle and prevention do a person at-risk have if no genetic test has been done (please describe)?
Reducing the intake of protein is really difficult: reducing cystine intake is ineffective as it is converted from methionine and compliance to a lifelong reduction to protein is unlikely to be followed by the patient. Increase in oral fluid assumption is instead easy to achieve and it must be recommended, in particular in case of diarrhoea, vomit, fever or other reasons for temporary dehydration.
3.3 Genetic risk assessment in family members of a diseased person
(To be answered if in 1.10 ‘C' was marked)
3.3.1 Does the result of a genetic test resolve the genetic situation in that family?
Yes.
3.3.2 Can a genetic test in the index patient save genetic or other tests in family members?
Yes: in case of a known familial mutation, carriership can be confirmed or excluded.
3.3.3 Does a positive genetic test result in the index patient enable a predictive test in a family member?
It is often asked for by parents of an affected child who have further children. It should be offered if informative biochemical data are not available to prove the diagnosis as type B carriers (heterozygote carriers with only one SLC7A9 mutation) often have a confounding urinary pattern. Positive result may induce positive behaviour in order to reduce future stone formation.
3.4 Prenatal diagnosis
(To be answered if in 1.10 ‘D' was marked)
3.4.1 Does a positive genetic test result in the index patient enable a prenatal diagnosis?
Yes, but a prediction of the clinical course is not possible.6, 10
4. IF APPLICABLE, FURTHER CONSEQUENCES OF TESTING
Please assume that the result of a genetic test has no immediate medical consequences. Is there any evidence that a genetic test is nevertheless useful for the patient or his/her relatives? (Please describe)
Yes, for the family genetic counselling is always useful.
Acknowledgments
This work was supported by CIBERER, EuroGentest2 (Unit 2: ‘Genetic testing as part of health care'), a Coordination Action under FP7 (Grant Agreement Number 261469) and the European Society of Human Genetics.
The authors declare no conflict of interests.
References
- Bisceglia L, Fischetti L, Bonis PD, et al. Large rearrangements detected by MLPA, point mutations, and survey of the frequency of mutations within the SLC3A1 and SLC7A9 genes in a cohort of 172 cystinuric Italian patients. Mol Genet Metab. 2010;99:42–52. doi: 10.1016/j.ymgme.2009.09.001. [DOI] [PubMed] [Google Scholar]
- Calonge MJ, Gasparini P, Chillarón J, et al. Cystinuria caused by mutations in rBAT, a gene involved in the transport of cystine. Nat Genet. 1994;6:420–425. doi: 10.1038/ng0494-420. [DOI] [PubMed] [Google Scholar]
- Chatzikyriakidou A, Sofikitis N, Kalfakakou V, Siamopoulos K, Georgiou I. Evidence for association of SLC7A9 gene haplotypes with cystinuria manifestation in SLC7A9 mutation carriers. Urol Res. 2006;34:299–303. doi: 10.1007/s00240-006-0060-6. [DOI] [PubMed] [Google Scholar]
- Chillarón J, Font-Llitjós M, Fort J, et al. Pathophysiology and treatment of cystinuria. Nat Rev Nephrol. 2010;6:424–444. doi: 10.1038/nrneph.2010.69. [DOI] [PubMed] [Google Scholar]
- Dello Strologo L, Pras E, Pontesilli C, et al. Comparison between SLC3A1 and SLC7A9 cystinuria patients and carriers: a need for a new classification. Am Soc Nephrol. 2002;13:2547–2553. doi: 10.1097/01.asn.0000029586.17680.e5. [DOI] [PubMed] [Google Scholar]
- Eggermann T, Elbracht M, Haverkamp F, Schmidt C, Zerres K. Isolated cystinuria (OMIM 238200) is not a separate entity but is caused by a mutation in the cystinuria gene SLC7A9. Clin Genet. 2007;71:597–598. doi: 10.1111/j.1399-0004.2007.00797.x. [DOI] [PubMed] [Google Scholar]
- Feliubadaló L, Font M, Purroy J, et al. Non-type I cystinuria caused by mutations in SLC7A9, encoding a subunit (bo,+AT) of rBAT. Nat Genet. 1999;23:52–57. doi: 10.1038/12652. [DOI] [PubMed] [Google Scholar]
- Font-Llitjós M, Jiménez-Vidal M, Bisceglia L, et al. New insights into cystinuria: 40 new mutations, genotype-phenotype correlation, and digenic inheritance causing partial phenotype. J Med Genet. 2005;42:58–68. doi: 10.1136/jmg.2004.022244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martens K, Heulens I, Meulemans S, et al. Global distribution of the most prevalent deletions causing hypotonia-cystinuria syndrome. Eur J Hum Genet. 2007;15:1029–1033. doi: 10.1038/sj.ejhg.5201881. [DOI] [PubMed] [Google Scholar]
- Pras E, Kochba I, Lubetzky A, Pras M, Sidi Y, Kastner DL. Biochemical and clinical studies in Libyan Jewish cystinuria patients and their relatives. Am J Med Genet. 1998;80:173–176. [PubMed] [Google Scholar]