

Abstract
Paget's disease of the breast is a rare type of cancer of the nipple–areola complex and that is often associated with an underlying in situ or invasive carcinoma. This article provides an overview and we review the main clinicopathological and therapeutic features of mammary Paget's disease.
Keywords: Breast, nipple, Paget's disease
INTRODUCTION
Paget's disease of the breast has been recognized as a distinct clinical entity for over 120 years. Since the condition in itself is often innocuous and limited to a surface appearance, it is sometimes dismissed, although actually indicative of a very serious underlying condition, breast cancer. Its clinical significance, pathogenesis, and surgical treatment remain topics of clinical debate. The aim of this review is to describe the characteristic clinical and pathologic features, histogenesis and treatment modalities of this entities.
EPIDEMIOLOGY
Paget's disease of the breast, a disorder of the nipple–areola complex, first described by Sir James Paget in 1874,[1] is an uncommon disease, accounting for 1–4.3% of all the breast carcinomas.[2] It is often associated with underlying ductal carcinoma in situ and/or invasive ductal cancer.[3] Paget's disease is much more frequent in women because of the predominance of breast cancer in females.[4] It occurs most commonly in post-menapousal women, often during the sixth decade of life (mean age 57 years), but it has been observed in adolescents[5] and in elderly patients also.[6]
CLINICAL FEATURES
The clinical appearance of the Paget's disease is usually a thickened, sometimes pigmented, eczematoid, erythematous weeping or crusted lesion with irregular borders [Figure 1a–c]. Usually, the lesion is limited to the nipple or extended to the areola, and in advanced cases it also may involve the surrounding skin. The surface of the lesion is occasionally slightly infiltrated. Complaints of pain or itching are frequent. The nipple may be retracted or deformed. Early changes including scaling and redness may be mistaken for eczema or some other inflammatory conditions.[3,7] The inflammatory component may be improved by topical treatment, a result that masks the underlying condition and this may cause delay in diagnosis.[3] Advanced lesions present as a round, ovoid or polycylic eczema-like plaque with a pink or red hue but it is sharply demarcated from the adjacent normal skin [Figure 1d]. These stages of the Paget's disease may result in ulceration and destruction of the nipple–areola complex[4] In these stages, serous and bloody discharge may occur. Retraction of the nipple can be seen. This clinical presentation is different from the changes seen with inflammatory carcinoma of the breast in which patients have diffuse breast erythema and secondary involvement of the skin and nipple.[3,7] The lesions are almost unilateral and very rarely bilateral.[8] Paget's disease may also develop on ectopic breasts[9] and accessory nipples.[5] No clinical and epidemiologic factors are known to predispose patients to develop Paget's disease. A 35-year-old patient who had systemic scleroderma involving the skin of the breast with coexistent Paget's disease has been described.[10]
Figure 1.
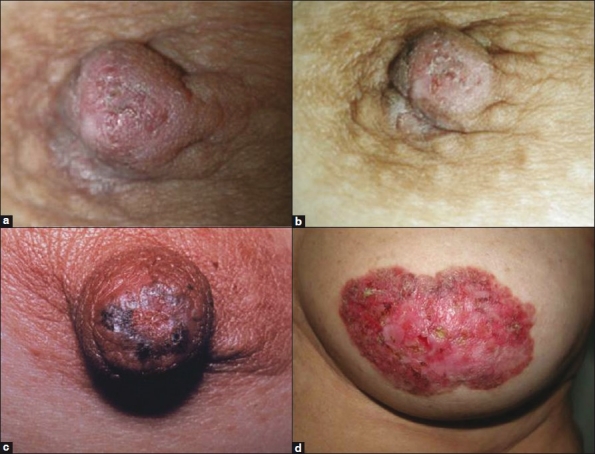
(a and b) Paget's disease of the nipple. The clinical appearance is usually a thickened, eczematoid crusted lesion with irregular borders. (c) Scaly, erythematous, crusty pigmentation and thickened plaques on the nipple, spreading to the surrounding areolar areas. (d) Advanced lesions show skin thickening, redness, erythema, erosion of the nipple and scaling around the nipple–areola
Mammary Paget's disease (MPD) is almost always associated with an underlying breast cancer in 92–100% of cases.[11,12] Approximately 50% of this patients present with an associated palpable mass in the breast.[3,4] In cases where mass is palpable, invasive carcinoma is likely to be found. On the other hand, patients presenting without a clinical mass more likely have ductal carcinoma in situ (DCIS).[13] The tumors which may or may not be palpable, located usually close to areola, tend to be central and are often multifocal.[11] Patients with periphery localized tumors also have been reported. In one study, Chaudary et al. reported that 45% of palpable invasive carcinomas associated with Paget's disease in their series were located in the upper, outer quadrant.[14] Multifocality of the underlying carcinoma in Paget's disease has been reported to be between 42% and 63% in various studies.[11,13] Lymph node enlargement is found more often in cases with palpable tumor.[13] Of note, Paget's disease of the breast may be asymptomatic and unsuspected clinically and may be diagnosed as a histologic finding by a pathologist on a mastectomy specimen.[3]
Paget's disease of the breast can also occur in men.[15–17] The clinical features in men appear to be similar to those in women. Although there are no significant pathologic and clinical differences between male and female MPD, prognosis seems to be worse in men compared with women.[18] But this remains controversial.
RADIOLOGIC FEATURES
Paget's disease is almost always associated with an underlying in situ or invasive cancer or both.[13] The diagnosis is generally made on the basis of clinical findings. However, when the signs are evident and Paget's disease is suspected, imaging should be performed to detect the underlying carcinoma. Radiologic findings are important to assess appropriate further management and the treatment of the disease. Conventional imaging modalities such as mammography (MMG) may depict a mass or calcification representative of invasive cancer or DCIS, respectively. However, MMG is not always a reliable procedure for detecting MPD. It is limited in its depiction of underlying DCIS in women with Paget's disease.[19] In one study, cancer was mammographically occult in 15% of 52 patients with Paget's disease.[20] In another study, Morrogh et al. found that 65% of patients with negative MMG had an underlying unifocal cancer.[21] The sensitivity of MMG seems to be significantly higher in the presence of a palpable mass.[19,22] However, bilateral MMG is still important to detect suspicious lesions such as masses or clusters of microcalcifications, to asses the contralateral breast and to exclude multifocal disease. Also, MMG should be used in follow-up visits in patients selected for conservative treatment.[23] Mammographic findings include skin, nipple and areolar thickening, nipple retraction, subareolar or more diffuse microcalcifications and a discrete mass or masses or architectural distortion.[19,20] Due to the multricentricity of Paget's disease, it is important to evaluate the entire breast, even if a subareolar tumor is noted on physical examination.
Ultrasound (US) examination may be helpful and should be considered as a part of the initial evaluation, especially when MMG is negative;[24] however, mostly the findings are nonspecific and resemble those in cases of infection. US images may reveal parenchymal heterogeneousness, hypoechoic areas, discrete masses, skin thickening or dilated ducts.[20]
Breast magnetic resonance imaging (MRI) is known to be highly sensitive for the detection of breast cancer, especially in patients whose mammographic or US findings are normal or the extent of disease is uncertain.[20,25] MRI may show abnormal nipple enhancement, thickening of the nipple–areola complex, an associated enhancing DCIS or invasive tumor, or a combination of these, even when clinically unsuspected.[26,27]
Because MMG and US have limitations in the evaluation of patients with Paget's disease, in the setting of clinically and mammographically occult disease, additional evaluation with MRI can help detect underlying invasive cancer and DCIS. Additionally, MRI may have a role in the preoperative evaluation of the patient and might facilitate appropriate further treatment decisions. While Paget's disease is primarily a clinical diagnosis, neither negative MMG nor MRI reliably can exclude an underlying malignancy. In fact, if the diagnosis is based solely on radiologic findings without careful clinical examination, it may result in a delay in diagnosis. As a result, both clinical and imaging findings are complementary and should be correlated to confirm or exclude a diagnosis of Paget's disease.
PATHOLOGICAL FEATURES
MPD is characterized by the invasion of epidermis by Paget's cells, malignant glandular epithelial cells with enlarged pleomorphic and hyperchromatic nuclei, with discernible but not prominent nucleoli, with abundant pale, clear cytoplasm, which often contains mucin. The cytoplasm may also contain melanin pigment. The cells do not form intercellular bridges with adjacent prickle cells. Mitotic figures may also be observed [Figures 2 and 3]. Paget's cells are more often located in the basal region of the epidermis either as single layers or as clusters of cells forming gland-like structures or nests. Because of the shrinkage artifact, the cells sometimes appear to lie within intraepidermal lacunae [Figure 4]. The number of cells varies greatly from a few isolated cells to complete replacement of parts of the epidermis. The epidermis may be eroded or hyperplastic, covered by ortho- or parakeratosis. Paget's cells are occasionally found within the outer epithelial layer of the hair follicles or the sweat gland excretory ducts. The underlying dermis shows reactive changes including variable degrees of telangiectasia and chronic inflammation, which cause the characteristic clinical appearance [Figure 4]. Ulceration is seen in advanced cases.[2,7] An underlying breast carcinoma is found in >90% of patients with Paget's disease.[13] This is nearly always of ductal type and may be either purely DCIS (most commonly associated with solid/comedo form) or a combination of DCIS and invasive carcinoma.[3]
Figure 2.
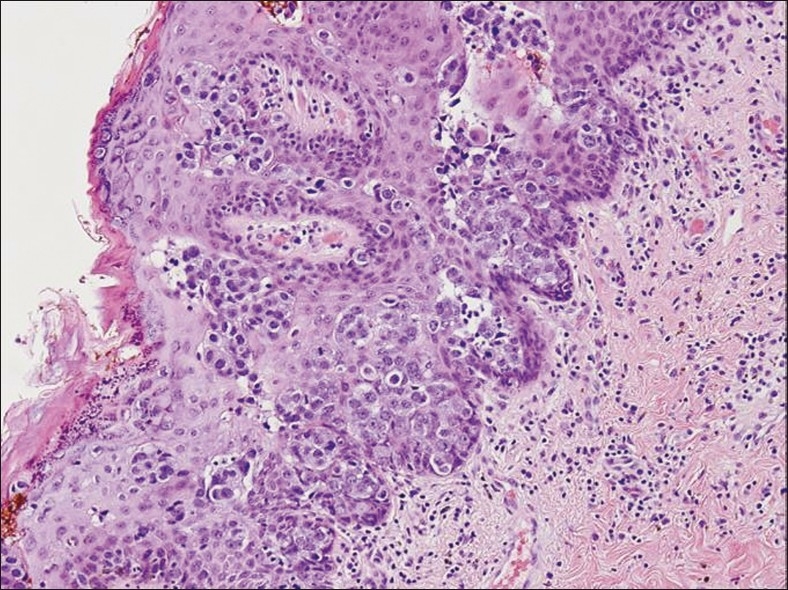
Paget's disease of the nipple. Nests and groups of malignant Paget's cells predominantly involving the lower layers of the epidermis. Epidermis may be eroded and hyperplastic (H and E, ×40)
Figure 3.
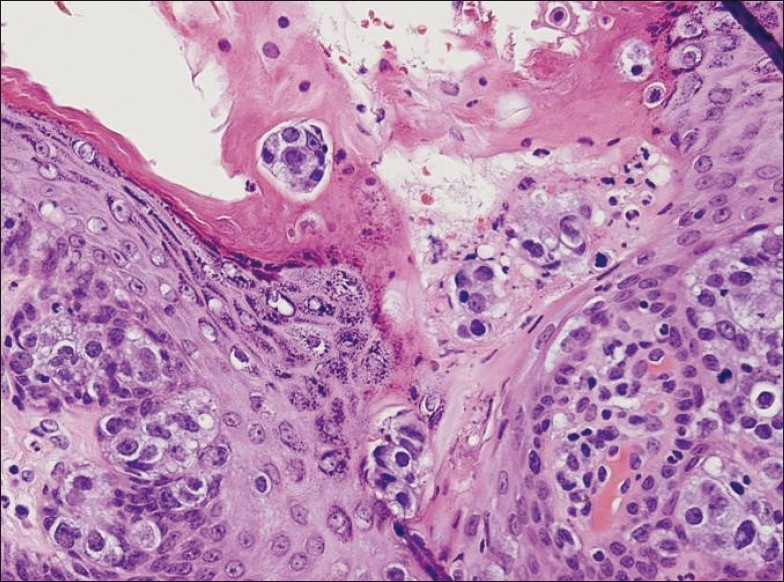
Paget's disease of the nipple with superficial ulceration. The tumor cells have abundant pale cytoplasm, pleomorphic and hyperchromatic nuclei with prominent nucleoli. Mitotic figures are seen (H and E, ×100)
Figure 4.
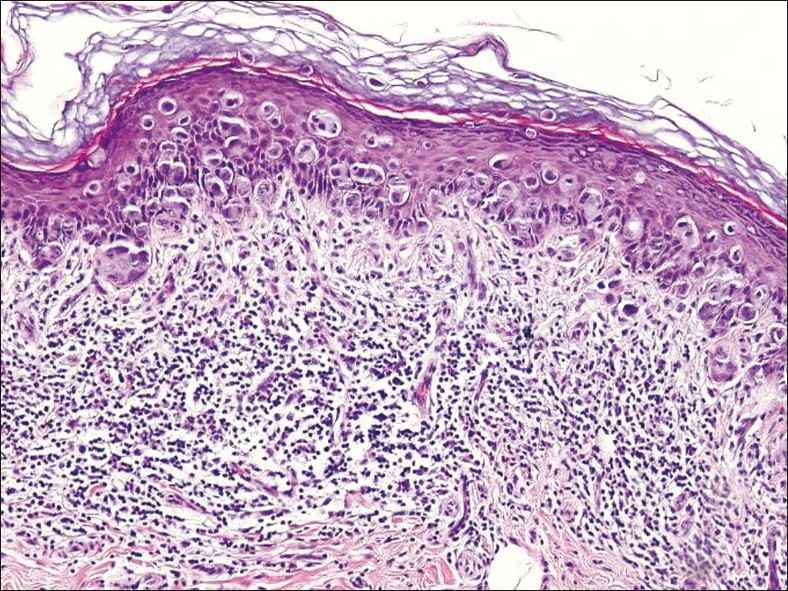
Carcinoma cells form a band in the deep epidermis and they are scattered individually throughout the squamous epithelium. The lacunar arrangement of carcinoma cells is commonly seen in Paget's disease. An extensive lymphocytic infiltrate with involvement largely concentrated in the deep epidermis (H and E, ×40)
Immunohistochemistry is useful not only in the diagnosis of the Paget's disease but also in differentiating it from other entities and in attempting to clarify the cell of origin in Paget's disease. Paget's cells show similar immunohistochemical staining pattern as that of adenocarcinomas growing within the breast. They show overexpression with low molecular weight cytokeratins (CKs), such as cytokeratin 7 (CK7) [Figure 5], and they typically do not express high molecular weight CKs, such as CK10, CK12, CK14, that stain the neoplastic cells of epidermoid carcinoma or Bowen's disease.[28,29] Paget's cells are positive for CK7 in nearly all cases and are not reactive for CK20. Absence of the CK7 reactivity in Paget's cells is usually associated with lack of CK7 reactivity in underlying carcinoma. This pattern of CK expression may help to predict the presence or absence of associated internal malignancy. Paget's cells also express other glandular antigens such as epithelial membrane antigen (EMA), carcinoembrionic antigen (CEA), gross cystic disease fluid protein 15 (GCDFP-15) and several mucins, but do not express either high molecular weight CKs or melanocytic antigens.[30] This immunostaining pattern and the presence of intracellular mucin in many cases favor the glandular origin of Paget's cells. Hormone receptor reactivity in the nuclei of the Paget's cells present the reactivity of underlying carcinoma also. About 50% of mammary carcinomas are negative for one or both of these markers. Negative results do not exclude a diagnosis of Paget's disease. Paget's disease often is estrogen and progesteron receptor negative because the underlying carcinomas tend to be poorly differentiated.[7] The ras oncogene product p21 overexpression has been demonstrated in mammary and extramammary Paget's disease.[31] Paget's cells also express p53,[32,33] cell cycle related antigens, such as p21, Ki-67, cyclin D1,[34,35] androgen receptors[36] and oncoprotein Her-2.[34,37] Of note, studies showed that the Her-2 oncoprotein may have a function in vivo to promote intraepithelial spread of adenocarcinoma cells. Generally, in many cases, there is correlation between positive staining for Her-2 oncoprotein of Paget's cells and underlying in situ or invasive breast carcinoma.[37,38] Also, recently, some studies suggested that NY-BY-1 expression or loss of pRb expression may have a role to play in the pathogenesis of Paget's disease.[33,35,39]
Figure 5.
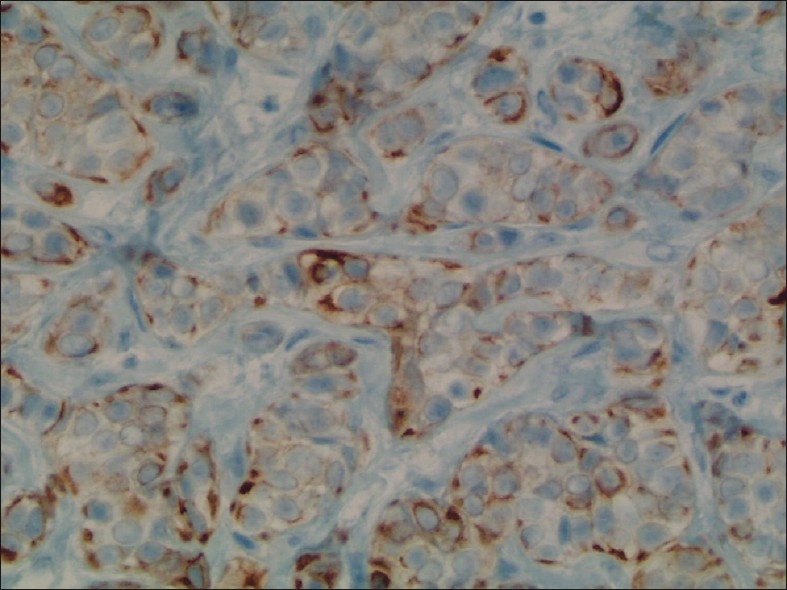
Paget's cells are highlighted by an immunostain for (CK7, ×200)
The combination of careful assesment of morphological features with appropriate immunohistochemical stains allows correct diagnosis in most cases of Paget's disease of the breast in clinical practice.
HISTOGENESIS
Since the histologic features of the Paget's disease of the breast were first described, its histogenesis has remained controversial. There are two main hypotheses to explain its nature and origin.
The first theory, epidermotropic theory, suggests that the Paget's cells originate from ductal cancer cells that have migrated along the basal membrane of the nipple.[40,41] Epidermotropic theory is supported by the presence of underlying intraductal or invasive carcinoma in the majority of patients.[42] Additional support for the epidermotropic theory has been based on immunohistochemical studies demonstrating that in most cases of MPD, immunohistochemical staining is very similar to that of the associated underlying carcinoma.[43] The demonstration of overexpression of Her-2 protein in Paget's cells has led to the hypothesis that a motility factor secreted by epidermal keratinocytes is capable of attracting Paget's cells within the nipple epidermis. This factor, named “Heregulin-a.” could bind to the Her-2 family receptors that are expressed by Paget's cells. The Her-2 protein has a growth stimulating effect; furthermore, it enhances the motility of tumor cells by the interaction of the membrane-expressed neu-protein and a motility factor, resulting in chemotaxis and invasion of the epidermis by the Paget's cells.[44]
The second theory, called in situ malignant transformation or degeneration from existing cells, regards the Paget's cells as malignant keratinocytes appearing in situ, and therefore considers Paget's disease of the breast to be an in situ carcinoma, independent of any underlying carcinoma.[45–47] Further support for this theory has come from ultrastructural studies demonstrating microvilli and desmosomal attachments between the keratinocytes and Paget's cells, the findings which mitigate against the migratory nature of the Paget's cell and suggest an intraepidermal origin.[45,48]
Treatment for the Paget's disease depends upon the origin of Paget's cells. If the Paget's cells originated de novo in the nipple epithelium, then the need for mastectomy becomes controversial. In patients without an associated palpable or mammographic lesion, simple local treatment (resection of nipple–areolar complex or irradiation) followed by no additional therapy to the remaining breast parenchyma might be an appropriate therapeutic alternative. On the other hand, the epidermotropic theory which is associated with an in situ or invasive carcinoma of the breast, requires the standard therapy, often necessitating mastectomy.
DIAGNOSIS
The diagnosis of Paget's disease can be made from a wedge biopsy, a superficial “shave” biopsy of epidermis or punch biopsy. The wedge biopsy is the most useful method to make the diagnosis because the epidermis can adequately represent and the biopsy is likely to include a part of lactiferous duct. The shave biopsy is less likely to contain sufficient number of Paget's cells, especially when the surface of the lesion is ulcerated. Although a punch biopsy will include the underlying stroma and possibly part of a duct, there is frequently little epidermis to examine. None of these procedures are always successful; therefore, it is sometimes necessary to take a second biopsy or excise the nipple.[7] When a patient has nipple–areola skin changes, a full thickness biopsy of the nipple and areola is important to establish the diagnosis.
It may be possible to recognize the Paget's cells with immunocytochemistry. Cytologic examination of skin scrapings reveals single malignant cells with vacuolated cytoplasm and eccentric nuclei, three-dimensional aggragates and acinar groups consistent with glandular differentiation. However, the material obtained is variably cellular and often shows a backround of keratinous debris, which may lead to confusion with inflammatory skin conditions or squamous metaplasia.[49,50] The use of immunohistochemical stainings, such as carcinoembryonic antigen (CEA), mucin or Her-2 oncoprotein, has been suggested to enhance the diagnosis;[43] however, a negative result does not exclude a diagnosis of Paget's disease of the breast, and therefore open (surgical) biopsy should be considered as standard for the diagnosis of Paget's disease of the breast.
DIFFERENTIAL DIAGNOSIS
The clinical differential diagnoses of Paget's cells include inflammatory changes such as atopic or contact dermatitis of the nipple, chronic eczema, psoriasis, mammary ductal ectasia with chronic nipple discharge, syphilitic chancre as well as tumors such as benign intraductal papilloma, Bowen's disease, basal cell carcinoma, superficial spreading malignant melanoma (particularly in the pigmented lesions), erosive adenomatosis of the nipple and hyperplasia of mammary gland related cells (so called Toker cells).[51–54] Because of the close similarity to skin lesions, the diagnosis may be delayed or many cases can be misdiagnosed.
The characteristic histopathologic feature of the Paget's disease is the presence of Paget's cells. These cells more likely form clusters in the basal portion of the epidermis and have a distribution similar to that of junctional melanocytes. Distinguishing Paget's disease from melanoma is more difficult, especially when the carcinoma cells contain melanin pigment. Melanin can be present in both processes; however, the atypical cells in melanoma show prominent nesting along the dermoepidermal junction, whereas the cells of the Paget's disease are usually distributed more diffusely. Involvement of the dermoepidermal junction with extension directly into the papillary dermis from the neoplastic cells is a characteristic finding with malignant melanoma.[55,56] Acinar formation is not seen in melanoma and there is no intracellular mucin present. In difficult cases, immunohistochemical markers may be used to differentiate these entities.[56]
Longstanding lesions of Paget's disease often show prominent hyperkeratosis and parakeratosis with epidermal hyperplasia, elongation of rete ridges and reactive atypia of the keratinocytes. In these situations, Paget's disease can be misdiagnosed as Bowen's disease. Intracellular mucin, signet cells, glandular structures and acini formation favor Paget's disease. In cases where glandular differentiation is absent, immunohistochemistry will usually resolve this problem.[56,57]
In the original paper, Toker described the presence of clear cells within the nipple of the patients affected by breast carcinoma. However, similar cells were also identified in patients unaffected by breast cancer.[58] In this study, it was suggested that most Toker cells are benign but a few of them can show atypical cytological findings.[58] They appear to be a benign counterpart of the malignant cells of MPD. Recently, it has been hypothesized that Toker cells are derived from lactiferous ductal epithelium, and Toker cells have also been referred to as mammary gland precursor cells.[59] Zeng et al. hypothesize in their study that Toker cells share histogenesis with lactiferous duct epithelial cells because these cells are located in the transition zone between the epidermis and lactiferous duct, have cytological similarity, proliferate in association with the underlying proliferative process and share immunohistochemical reactivity (both lactiferous duct epithelium and some Toker cells are CK7+ and CAM5.2+).[60]
Toker cells are found in the epidermis of the nipple, immediately adjacent to the openings of the lactiferous ducts, along the basal layer of the epidermis or scattered in the stratum Malpighii. They are observed in about 10% of standard histological preparations of normal nipples.[52,61] Because of their morphological and immunohistochemical similarities to mammary Paget's cells, their presence may lead to confusion with MPD that lack an associated invasive carcinoma or focus of ductal in situ carcinoma. Especially in cases of Toker cell hyperplasia with cytologic atypia, it may be difficult to distinguish the Paget's cells of MPD from Toker cells. In most cases, Toker cells can be readily distinguished from Paget's cells, the latter having larger, pleomorphic and cytologically atypical nuclei.[61] Toker cells are usually dispersed singly, and small and medium-sized cells with pale or clear cytoplasm which may consist of a large (mucin-negative) vacuole that appears clear on routine stains.
A wide variety of antibodies have been used to distinguish Toker cells and Paget's cells immunohistochemically. Studies from several groups have shown that in the nipple, both Toker cells and Paget's cells express CK7, CAM5.2 and EMA,[62] but do not express CK20, GCFDP-15, high molecular weight keratin and S-100 protein.[54,63] CK7 and Her-2 have been proposed to be specific and sensitive markers for MPD.[64,65] In contrast to Paget's cells, Toker cells are usually negative for Her-2.[61] Tommaso et al. suggested in their study including 40 cases, the combined use of CD138/p53 and the lack of the immunoreactivity with these antibodies is very helpful in distinguishing Toker cells from those of Paget's disease.[65] In another study, Park et al. found that both high expression of Ki-67 and Her-2 were consistently positive in mammary Paget's cells but almost always negative in Toker cells.[61]
PROGNOSIS
Without treatment, the skin lesions invariably spread progressively before the development of invasive breast cancer, manifesting with a palpable mass followed by lymph node and visceral metastasis. Factors of unfavorable prognosis include the presence of a palpable breast tumor, lymph node enlargement, histological type of breast cancer, and age younger than 60 years.[4,66] The prognosis is different in patients with a palpable mass and those without a palpable mass. Patients with a palpable mass almost always have an associated underlying invasive carcinoma and a high rate of axillary lymph node metastasis.[12,34,42] Overall survival has been shown to correlate with lymph node status and is reported to be 75–95% in patients with negative lymph nodes and as low as 20–25% in those with positive lymph nodes.[34,42] In another study, the authors have demonstrated a 10-year disease-specific survival rate of 47% in patients with positive nodes and 93% in those with negative nodes.[66] These results showing that adjuvant treatment is recommended on the basis of lymph node status and features of the primary tumor as determined by final pathologic examination.
Although the clinical behavior in men is similar to that in women, men appear to have a worse prognosis, with an estimated 5-year survival rate of 20–30%.[15,18] Presence of Paget's disease of the breast does not seem to influence directly the prognosis of an underlying cancer in a given stage. However, in most clinical studies on Paget's disease of the breast, initiation of the treatment was inappropriately delayed, frequently longer than 12 months.
TREATMENT
The surgical treatment of Paget's disease is controversial. Mastectomy with or without axillary lymph node dissection has long been regarded as the standard therapy for Paget's disease, even in the absence of other clinical signs of malignancy.[67] The underlying mass is often invasive cancer with a high risk of axillary node metastases. The patients have a poorer prognosis and usually the appropriate therapy is based on the pathologic findings of the mass and axillary staging.[12] In the literature, almost all patients treated with local excision, radiotherapy, or both had the clinical presentation of Paget's disease without a palpable mass. Dixon et al. reported a high recurrence rate of 40% in patients treated with local excision alone, whose mammograms suggested in situ changes confined to the nipple area.[68] Polgar et al. reported a local recurrence rate of 33% with a median follow-up time of 6 years in 33 patients treated with local excision alone with or without underlying ductal carcinoma in situ confined to the nipple–areola complex.[69] They concluded that the local excision alone was not an appropriate treatment for patients with Paget's disease of the nipple.
With the increasing diagnosis of the early breast cancers and the findings from multiple randomized, prospective trials demonstrating that breast conserving therapy is a feasible alternative for patients with disease limited to the central segment of the breast,[66,70] the reported techniques for conservative management of Paget's disease vary widely. These include nipple excision alone (partial or complete), central segmentectomy alone, these resections plus radiation and radiation without resection.[68,71,72] Recent reports from several studies with long-term follow-up have shown that breast-conserving surgery is equivalent to mastectomy in terms of overall and disease-free survival in patients with breast cancer.[73–75] If conservative therapy is adopted, the patient should be followed up carefully with regular MMG.[76] Mastectomy should be reserved for the few occasions, when relapse occurs.[72]
Use of breast radiation therapy alone for the Paget's disease of the breast has been reported in limited numbers and with varying results.[71,72,77] Current studies suggest that irradiation of the breast tissue to a radical dose may be effective against DCIS.[78] This gives support to the view that selected patients with Paget's disease of the breast can be treated by radiotherapy as an alternative to radical surgery in selected patients with Paget's disease confined to the nipple, without clinical or radiological detectable breast tumor.[77]
In summary, Paget's disease of the nipple is almost always associated with an underlying invasive or non-invasive breast cancer. Breast conserving therapy has been shown to be a viable alternative to mastectomy as the treatment of Paget's disease. The surgical treatment plan must be chosen on the basis of careful clinical and radiological assessment of the patient. Postoperative adjuvant therapies should be based on the final tumor node metastasis stage.
AUTHOR'S PROFILE
Dr. Cansu Karakas, Cansu Karakas Experimental Radiation Oncology The University of Texas MD Anderson Cancer Center Unit-0066 1515 Holcombe Blvd Houston, TX
ACKNOWLEDGMENTS
I would like to thank Dr. Khandan Keyomarsi for the critical reading of this manuscript. I also thank Dr. Aysegul Sahin for helpful discussions during the writing of this manuscript.
REFERENCES
- 1.Paget J. On the disease of the mammary areola preceding cancer of the mammary gland. St Bartholomews Hosp Rep. 1874;10:87–9. [Google Scholar]
- 2.Tavassoli FA. Norwalk, Connecticut: AppletonandLange; 1999. Pathology of the breast; pp. 731–60. [Google Scholar]
- 3.Sakorafas GH, Blanchard K, Sarr MG, Farley DR. Paget's disease of the breast. Cancer Treat Rev. 2001;27:9–18. doi: 10.1053/ctrv.2000.0203. [DOI] [PubMed] [Google Scholar]
- 4.Kanitakis J. Mammary and extramammary Paget's disease. J Eur Acad Dermatol Venereol. 2007;21:581–90. doi: 10.1111/j.1468-3083.2007.02154.x. [DOI] [PubMed] [Google Scholar]
- 5.Martin VG, Pellettiere EV, Gress D, Miller AW. Paget's disease in an adolescent arising in a supernumerary nipple. J Cutan Pathol. 1994;21:283–6. doi: 10.1111/j.1600-0560.1994.tb00275.x. [DOI] [PubMed] [Google Scholar]
- 6.Ascensao AC, Marques MS, Capitao-Mor M. Paget's disease of the nipple.Clinical and pathological review of 109 female patients. Dermatologica. 1985;170:170–9. [PubMed] [Google Scholar]
- 7.Rosen PP. Rosen's breast pathology. 2nd ed. Philadelphia: Lippincott-Raven; 2001. Paget's disease of the nipple; pp. 565–80. [Google Scholar]
- 8.Franceschini G, Masetti R, D’Ugo D, Palumbo F, D’Alba P, Mulè A, et al. Synchronous bilateral Paget's disease of the nipple associated with bilateral breast carcinoma. Breast J. 2005;11:355–6. doi: 10.1111/j.1075-122X.2005.21722.x. [DOI] [PubMed] [Google Scholar]
- 9.Kao GF, Graham JH, Helwig EB. Paget's disease of the ectopic breast with an underlying intraductal carcinoma: Report of a case. J Cutan Pathol. 1986;13:59–66. doi: 10.1111/j.1600-0560.1986.tb00461.x. [DOI] [PubMed] [Google Scholar]
- 10.Suster S, Ronnen M, Huszar M, J Bubis JJ. Paget's disease of the breast with underlying carcinoma arising in systemic scleroderma. J Dermatol Surg Oncol. 1988;14:648–50. doi: 10.1111/j.1524-4725.1988.tb03394.x. [DOI] [PubMed] [Google Scholar]
- 11.Kothari AS, Beechey-Newman N, Hamed H, Fentiman IS, D’Arrigo C, Hanby AM, et al. Paget disease of the nipple: A multifocal manifestation of higher-risk disease. Cancer. 2002;95:1–7. doi: 10.1002/cncr.10638. [DOI] [PubMed] [Google Scholar]
- 12.Kollmorgen DR, Varanasi JS, Edge SB, Carson WE., 3rd Paget's disease of the breast: a 33-year experience. J Am Coll Surg. 1998;187:171–7. doi: 10.1016/s1072-7515(98)00143-4. [DOI] [PubMed] [Google Scholar]
- 13.Yim JH, Wick MR, Philpott GW, Norton JA, Doherty GM. Underlying pathology in mammary Paget's disease. Ann Surg Oncol. 1997;4:287–92. doi: 10.1007/BF02303576. [DOI] [PubMed] [Google Scholar]
- 14.Chaudary MA, Millis RR, Lane EB, Miller NA. Paget's disease of the nipple: a 10-year review including clinical, pathological and immunohistochemical findings. Breast Cancer Res Treat. 1986;8:139–46. doi: 10.1007/BF01807702. [DOI] [PubMed] [Google Scholar]
- 15.Lancer HA, Moschella SL. Paget's disease of the male breast. J Am Acad Dermatol. 1982;7:393–6. doi: 10.1016/s0190-9622(82)70126-4. [DOI] [PubMed] [Google Scholar]
- 16.O’Sullivan ST, McGreal GT, Lyons A, Burke L, Geoghegan JG, Brady MP. Paget's disease of the breast in a man without underlying breast carcinoma. J Clin Pathol. 1994;47:851–2. doi: 10.1136/jcp.47.9.851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ho TC, Jacques M, Schopflocher P. Pigmented Paget's disease of the male breast. J Am Acad Dermatol. 1990;23:338–41. doi: 10.1016/0190-9622(90)70217-6. [DOI] [PubMed] [Google Scholar]
- 18.Deasai DC, Brennan EJ, Carp NZ. Paget's disease of the male breast. Am Surg. 1996;62:1068–72. [PubMed] [Google Scholar]
- 19.Ikeda DM, Helvie MA, Frank TS, Chapel KL, Andersson IT. Paget disease of the nipple: radiologic-pathologic correlation. Radiology. 1993;189:89–94. doi: 10.1148/radiology.189.1.8396786. [DOI] [PubMed] [Google Scholar]
- 20.Gunhan-Bilgen I, Oktay A. Paget's disease of the breast: clinical, mammographic, sonographic and pathologic findings in 52 cases. Eur J Radiol. 2006;60:256–63. doi: 10.1016/j.ejrad.2006.06.010. [DOI] [PubMed] [Google Scholar]
- 21.Morrough M, Morris EA, Liberman L, Van Zee K, Cody HS, 3rd, King TA. MRI indentifies otherwise occult disease in select patients with Paget disease of the nipple. J Am Coll Surg. 2008;206:316–21. doi: 10.1016/j.jamcollsurg.2007.07.046. [DOI] [PubMed] [Google Scholar]
- 22.Sawyer RH, Asbury DL. Mammographic appearances in Paget's disease of the breast. Clin Radiol. 1994;49:185–8. doi: 10.1016/s0009-9260(05)81773-8. [DOI] [PubMed] [Google Scholar]
- 23.Burke ET, Brauning MP, McLelland R, Pisan ED, Cooper LL. Paget disease of the breast: a pictorial assay. Radiographics. 1998;18:1459–64. doi: 10.1148/radiographics.18.6.9821194. [DOI] [PubMed] [Google Scholar]
- 24.Yang WT, King W, Metreweli C. Clinically and mammographically occult invasive ductal carcinoma diagnosed by ultra- sound: the focally dilated duct. Australas Radiol. 1997;41:73–5. doi: 10.1111/j.1440-1673.1997.tb00476.x. [DOI] [PubMed] [Google Scholar]
- 25.Morrogh M, Morris EA, Liberman L, Borgen PI, King TA. The predictive value of ductography and magnetic resonance imaging in the management of nipple discharge. Ann Surg Oncol. 2007;14:3369–77. doi: 10.1245/s10434-007-9530-5. [DOI] [PubMed] [Google Scholar]
- 26.Amano G, Yajima M, Moroboshi Y, Kuriya Y, Ohuchi N. MRI accurately depicts underlying DCIS in a patient with Paget's disease of the breast without palpable mass and mammography findings. Jpn J Clin Oncol. 2005;35:149–53. doi: 10.1093/jjco/hyi044. [DOI] [PubMed] [Google Scholar]
- 27.Frei KA, Bonel HM, Pelte MF, Hylton NM, Kinkel K. Paget disease of the breast: findings at magnetic resonance imaging and histopathologic correlation. Invest Radiol. 2005;40:363–7. doi: 10.1097/01.rli.0000163742.40401.4e. [DOI] [PubMed] [Google Scholar]
- 28.Smith KJ, Tuur S, Corvette D, Lupton GP, Skelton HG. Cytokeratin 7 staining in mammary and extramammary Paget's disease. Mod Pathol. 1997;11:1069–74. [PubMed] [Google Scholar]
- 29.Yao DX, Hoda SA, Chiu A, Ring L, Rosen PP. Intraepidermal cytokeratin 7 immunoreactive cells in the non-neoplastic nipple may represent interepithelial extension of lactiferous duct cells. Histopathology. 2002;40:230–6. doi: 10.1046/j.1365-2559.2002.01362.x. [DOI] [PubMed] [Google Scholar]
- 30.Kanitakis J. Solid cutaneous tumours. In: Kanitakis J, Vassileva S, Woodley D, editors. Diagnostic Immunohistochemistry of the Skin. An Illustrated Text. London: Chapman and Hall Medical; 1998. pp. 279–99. [Google Scholar]
- 31.Mori O, Hachisuka H, Nakano S, Sasai Y, Shiku H. Expression of ras p21 in mammary and extramammary Paget's disease. Arch Pathol Lab Med. 1990;114:858–61. [PubMed] [Google Scholar]
- 32.Kanitakis J, Thivolet J, Claudy A. p53 protein expression in mammary and extramammary Paget's disease. Anticancer Res. 1993;13:2429–33. [PubMed] [Google Scholar]
- 33.Ellis PE, Fong LF, Rolfe KJ, Crow JC, Reid WM, Davidson T, et al. The role of p53 and Ki67 in Paget's disease of the vulva and the breast. Gynecol Oncol. 2002;86:150–6. doi: 10.1006/gyno.2002.6629. [DOI] [PubMed] [Google Scholar]
- 34.Fu W, Lobocki CA, Silberberg BK, Chelladurai M, Young SC. Molecular markers in Paget disease of the breast. J Surg Oncol. 2001;77:171–8. doi: 10.1002/jso.1090. [DOI] [PubMed] [Google Scholar]
- 35.Ellis PE, MacLean AB, Crow JC, Wong Te Fong LF, Rolfe KJ, Perrett CW. Expression of cyclin D1 and retinoblastoma protein in Paget's disease of the vulva and breast: an immunohistochemical study of 108 cases. Histopathology. 2009;55:709–15. doi: 10.1111/j.1365-2559.2009.03434.x. [DOI] [PubMed] [Google Scholar]
- 36.Liegl B, Horn L, Moinfar F. Androgen receptors are frequently expressed in mammary and extramammary Paget's disease. Mod Pathol. 2005;18:1283–8. doi: 10.1038/modpathol.3800437. [DOI] [PubMed] [Google Scholar]
- 37.Sek P, Zawrocki A, Biernat W, Piekarski JH. HER2 molecular subtype is a dominant subtype of mammary Paget's cells.An immunohistochemical study. Histopathology. 2010;57:564–71. doi: 10.1111/j.1365-2559.2010.03665.x. [DOI] [PubMed] [Google Scholar]
- 38.Wolber RA, Dupuis BA, Wick MR. Expression of c-erbB-2 oncoprotein in mammary and extramammary Paget's disease. Am J Clin Pathol. 1991;96:243–7. doi: 10.1093/ajcp/96.2.243. [DOI] [PubMed] [Google Scholar]
- 39.Giger O, Caduff R, O’Meara A, Diener PA, Knuth A, Jager D, et al. Frequent expression of the breast differentiation antigen NY-BR-1 in mammary and extramammary Paget's disease. Pathol Int. 2010;60:726–34. doi: 10.1111/j.1440-1827.2010.02591.x. [DOI] [PubMed] [Google Scholar]
- 40.Muir R. The pathogenesis of Paget's disease of the nipple and associated lesions. Br J Surg. 1935;22:728–37. [Google Scholar]
- 41.Muir R. Further observations on Paget's disease of the nipple and associated lesions. J Pathol. 1939;49:299–312. [Google Scholar]
- 42.Ashikari R, Park K, Huvos AG, Urban JA. Paget's disease of the breast. Cancer. 1970;26:680–85. doi: 10.1002/1097-0142(197009)26:3<680::aid-cncr2820260329>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 43.Cohen C, Guarner J, DeRose PB. Mammary Paget's disease and associated carcinoma.An immunohistochemical study. Arch Pathol Lab Med. 1993;117:291–4. [PubMed] [Google Scholar]
- 44.Schelfhout VR, Coene ED, Delaey B, Thys S, Page DL, De Potter CR. Pathogenesis of Paget's disease: epidermal heregulin-alpha, motility factor, and the HER receptor family. J Natl Cancer Inst. 2000;92:622–8. doi: 10.1093/jnci/92.8.622. [DOI] [PubMed] [Google Scholar]
- 45.Sagami S. Electron microscopic studies in Paget's disease. Med J Osaka Univ. 1963;14:173–88. [PubMed] [Google Scholar]
- 46.Sagebiel RW. Ultrastructural observations on epidermal cells in Paget's disease of the breast. Am J Pathol. 1969;57:49–64. [PMC free article] [PubMed] [Google Scholar]
- 47.Lagios MD, Westdahl PR, Rose MR, Concannon S. Paget's disease of the nipple.Alternative management in cases without or with minimal extent of underlying breast carcinoma. Cancer. 1984;54:545–51. doi: 10.1002/1097-0142(19840801)54:3<545::aid-cncr2820540327>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 48.Jahn H, Osther PJ, Nielsen EH, Rasmussen G, Andersen J. An electron microscopic study of clinical Paget's disease of the nipple. APMIS. 1995;103:628–34. doi: 10.1111/j.1699-0463.1995.tb01415.x. [DOI] [PubMed] [Google Scholar]
- 49.Lucarotti ME, Dumm JM, Webb AJ. Scrape cytology in the diagnosis of Paget's disease of the breast. Cytopathology. 1994;5:301–5. doi: 10.1111/j.1365-2303.1994.tb00434.x. [DOI] [PubMed] [Google Scholar]
- 50.Samarasinghe D, Frost F, Sterrett G, Whitaker D, Ingram D, Shiner H. Cytological diagnosis of Paget's disease of the nipple by scrape smears: a report of five cases. Diagn Cytopathol. 1993;9:291–5. doi: 10.1002/dc.2840090309. [DOI] [PubMed] [Google Scholar]
- 51.Hitchcock A, Topham S, Bell J, Gullick W, Elston CW, Ellis IO. Routine diagnosis of mammary Paget's disease.A modern approach. Am J Surg Pathol. 1992;16:58–61. doi: 10.1097/00000478-199201000-00008. [DOI] [PubMed] [Google Scholar]
- 52.van der Putte SC, Toonstra J, Hennipman A. Mammary Paget's disease confined to the areola and associated with multifocal Toker cell hyperplasia. Am J Dermatopathol. 1995;17:487–93. doi: 10.1097/00000372-199510000-00010. [DOI] [PubMed] [Google Scholar]
- 53.Miller L, Tyler W, Maroon M, Miller OF., 3rd Erosive adenomatosis of the nipple: a benign imitator of malignant breast disease. Cutis. 1997;59:91–2. [PubMed] [Google Scholar]
- 54.Lundquist K, Kohler S, Rouse RV. Intraepidermal cytokeratin 7 expression is not restricted to Paget cells but is also seen in Toker cells and Merkel cells. Am J Surg Pathol. 1999;23:212–9. doi: 10.1097/00000478-199902000-00011. [DOI] [PubMed] [Google Scholar]
- 55.Mitchell S, Lachica R, Randall MB, Beech DJ. Paget's disease of the breast areola mimicking cutaneous melanoma. Breast J. 2006;12:233–6. doi: 10.1111/j.1075-122X.2006.00247.x. [DOI] [PubMed] [Google Scholar]
- 56.Lloyd J, Flanagan AM. Mammary and extramammary Paget's disease. J Clin Pathol. 2000;53:742–9. doi: 10.1136/jcp.53.10.742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Reed W, Oppedal BR, Eeg Larsen T. Immunohistology is valuable in distinguishing between Paget's disease, Bowen's disease and superficial spreading malignant melanoma. Histopathology. 1990;16:583–8. doi: 10.1111/j.1365-2559.1990.tb01163.x. [DOI] [PubMed] [Google Scholar]
- 58.Toker C. Clear cells of nipple epidermis. Cancer. 1970;25:601–10. doi: 10.1002/1097-0142(197003)25:3<601::aid-cncr2820250315>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- 59.Mai KT, Yazdi HM, Perkins DG. Mammary Paget's disease: evidence of diverse origin of the disease with a subgroup of Paget's disease developing from the superficial portion of the lactiferous duct and a discontinuous pattern of tumor spread. Pathol Int. 1999;49:956–61. doi: 10.1046/j.1440-1827.1999.00976.x. [DOI] [PubMed] [Google Scholar]
- 60.Zeng Z, Melamed J, Symmans PJ, Cangiarella JF, Shapiro RL, Peralta H, et al. Benign proliferative nipple duct lesions frequently contain CAM 5.2 and anti-cytokeratin 7 immunoreactive cells in the overlying epidermis. Am J Surg Pathol. 1999;23:1349–55. doi: 10.1097/00000478-199911000-00005. [DOI] [PubMed] [Google Scholar]
- 61.Park S, Suh YL. Useful immunohistochemical markers for distinguishing Paget cells from Toker cells. Pathology. 2009;41:640–4. doi: 10.3109/00313020903273092. [DOI] [PubMed] [Google Scholar]
- 62.Kohler S, Rouse RV, Smoller BR. The differential diagnosis of pagetoid cells in the epidermis. Mod Pathol. 1998;11:79–92. [PubMed] [Google Scholar]
- 63.Willman JH, Golitz LE, Fitzpatrick JE. Clear cells of Toker in accessory nipples. J Cutan Pathol. 2003;30:256–60. doi: 10.1046/j.0303-6987.2003.046.x. [DOI] [PubMed] [Google Scholar]
- 64.Keatings L, Sinclair J, Wright C, Corbett IP, Watchorn C, Hennessy C, et al. c-erbB-2 oncoprotein expression in mammary and extramammary Paget's disease: an immunohistochemical study. Histopathology. 1990;17:243–7. doi: 10.1111/j.1365-2559.1990.tb00714.x. [DOI] [PubMed] [Google Scholar]
- 65.Di Tommaso L, Franchi G, Destro A, Broglia F, Minuti F, Rahal D, et al. Toker cells of the breast.Morphological and immunohistochemical characterization of 40 cases. Hum Pathol. 2008;39:1295–300. doi: 10.1016/j.humpath.2008.01.018. [DOI] [PubMed] [Google Scholar]
- 66.Kawase K, Dimaio DJ, Tucker SL, Buchholz TA, Ross MI, Feig BW, et al. Paget's disease of the breast: there is a role for breast-conserving therapy. Ann Surg Oncol. 2005;12:391–7. doi: 10.1245/ASO.2005.05.026. [DOI] [PubMed] [Google Scholar]
- 67.Paone JF, Baker RR. Pathogenesis and treatment of Paget's disease of the breast. Cancer. 1981;48:825–9. doi: 10.1002/1097-0142(19810801)48:3<825::aid-cncr2820480326>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 68.Dixon AR, Galea MH, Ellis IO, Elston CW, Blamey RW. Paget's disease of the nipple. Br J Surg. 1991;78:722–3. doi: 10.1002/bjs.1800780627. [DOI] [PubMed] [Google Scholar]
- 69.Polgar C, Orosz Z, Kovacs T, Fodor J. Breast-conserving therapy for Paget disease of the nipple: a prospective European Organization for Research and Treatment of Cancer Study of 61 patients. Cancer. 2002;94:1904–5. doi: 10.1002/cncr.10405. [DOI] [PubMed] [Google Scholar]
- 70.Bijker N, Rutgers E, Duchateau L, Peterse JL, Julien JP, Cataliotti L. Breast-conserving therapy for Paget disease of the nipple: a prospective European organization for Research and Treatment of Cancer study of 61 patients. Cancer. 2001;91:472–7. doi: 10.1002/1097-0142(20010201)91:3<472::aid-cncr1024>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 71.Bulens P, Vanuytsel L, Rijnders A, van der chueren E. Breast conserving treatment of Paget's disease. Radiother Oncol. 1990;17:305–9. doi: 10.1016/0167-8140(90)90004-g. [DOI] [PubMed] [Google Scholar]
- 72.Stockdale AD, Brierley JD, White WF, Folkes A, Rostom AY. Radiotherapy for Paget's disease of the nipple: a conservative alternative. Lancet. 1989;2:664–6. doi: 10.1016/s0140-6736(89)90904-5. [DOI] [PubMed] [Google Scholar]
- 73.van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92:1143–50. doi: 10.1093/jnci/92.14.1143. [DOI] [PubMed] [Google Scholar]
- 74.Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347:1227–32. doi: 10.1056/NEJMoa020989. [DOI] [PubMed] [Google Scholar]
- 75.Fisher B, Anderson S, Bryant J, Margolese RG, Deutch M, Fisher ER, et al. Twenty-year follow up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41. doi: 10.1056/NEJMoa022152. [DOI] [PubMed] [Google Scholar]
- 76.el-Sharkawi A, Waters JS. The place for conservative treatment in the management of Paget's disease of the nipple. Eur J Surg Oncol. 1992;18:301–3. [PubMed] [Google Scholar]
- 77.Fourquet A, Campana F, Vielh P, Schlinger P, Jullien D, Vilcoq JR. Paget's disease of the nipple without detectable breast tumor: conservative management with radiation therapy. Int J Radiat Oncol Biol Phys. 1987;13:1463–5. doi: 10.1016/0360-3016(87)90311-7. [DOI] [PubMed] [Google Scholar]
- 78.Stotter AT, McNeese M, Oswald MJ, Ames FC, Romsdahl MM. The role of limited surgery with irradiation in primary treatment of ductal in-situ breast cancer. Int J Radiat Oncol Biol Phys. 1990;18:283–7. doi: 10.1016/0360-3016(90)90090-7. [DOI] [PubMed] [Google Scholar]