

Abstract
Environmental status and diarrhea is regarded as a complex and multidimensional topic. Diarrhea is one of the main water-borne diseases considered to be endemic in many regions of the world and brings the major health threats to the world populations, both in tropical and subtropical poor countries. The state Meghalaya situated in the North-Eastern India is an upland landmass bound by seven districts surrounded within by different tribes. The population is predominantly rural, with 81.41% of the population belongs merely to the scheduled tribes. The state offers a wide range of disease environments, dominated by communicable diseases (35.68%), and diarrhea is one of the water-borne diseases that alter the society of the state. Various factors like poor environmental sanitation, unavailability of safe drinking water, seasonal rainfall, infected foods, infection through fomites, flies, cockroaches, etc. are the main culprit that led to the cause of diarrhea in the state. The local people are very much closely associated with nature, and with their ethnobiological knowledge about the plants available around them, they can easily avert and cure themselves from several disease complications. In this review, the information regarding the traditional method of utilization of 58 plant species that are used to treat and cure diarrhea and dysentery are enlisted briefly.
Keywords: Diarrhea, dysentery, Meghalaya, medicinal plants, sacred groves
INTRODUCTION
Meghalaya [Figure 1] which is regarded as one of the seven sisters among the seven states of the Northeastern India is surrounded by three distinct primitive aboriginal tribes - the Khasis, the Jaintias, and the Garos, each occupying the respective hills district in the state. The Khasis and the Jaintias are believed to belong from the “Mon Khmer” subfamily which originated basically from the Indo -Chinese linguistic family. On the other hand, the Garos along with the kacharis are believed to belong to a distinct tribe which subsequently got separated and these people are still primitive among the tribes in Meghalaya.[1] Most of these tribes have a close association with nature and lived among most of the dense vegetation which is categorized into tropical, temperate, alpine, and the grassland areas. These regions are richly well surrounded by various plant resources which are either utilized by these tribes as edible food, shelter, and fodder or used as medicinal purpose to treat various ailments. The tropical monsoonal climate of the state Meghalaya is believed to be responsible for adaptation and the growth of various plants ranging from herbs, shrubs to trees. These areas are geo-morphologically young and active. Most of the region is botanically under -explored or even unexplored. However, most of the explored plants are of medicinal values, which are well utilized by the local tribal for curing and treatment of various disease ailments. The use of medicinal plants in the world, and especially in India, contributes significantly to primary health-care and was mostly utilized on the basis of their ethno -botanical purpose. Primarily, it is interesting to investigate whether their traditional uses are either supported by actual pharmacological effects or merely based on folklore.[2,3] Seventy percent of the total area of the state is covered mostly by forest and 90% of this area is under the property of tribal communities.[4] Most of these forest falls under the religious sacred groves of which 79 groves were reported totally in the state and of which more than 1886 plant species of various families belonging to orchids, medicinal and ornamental plants, timber, and resin -yielding plants were preserved safe inside these sacred areas.[5]
Figure 1.
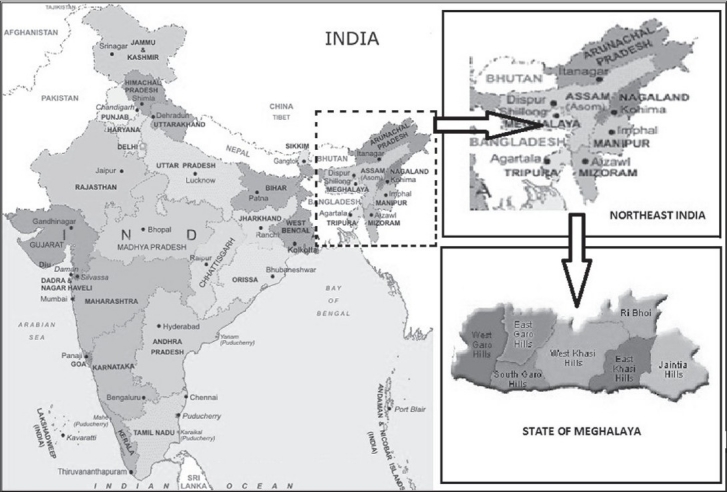
Map of India representing the state of Meghalaya with seven districts
CLIMATIC CONDITIONS OF THE STATE
The state has an approximate area of 22 549 -km2 and is globally situated between 25°47’-26°10’ N latitude and 89°45’-92°47’ E longitude.[1] The climate of the state is very much influenced by its topography and is controlled by seasonal winds like the south-west monsoon and the north-east winter winds. The temperature in the summer time reached as high as 25°C and in the winter season with the appearance of the higher altitudes, the temperature drops down up to as low as 2°C or sometimes even below freezing point at night and in the morning. The state has its record which is regarded presently as the world's rainiest and wettest place, with Mawsynram as the main affected area lying in the southern slopes of Khasi hills district of the state and occupying the maximum annual average rainfall of 1169 -cm in the world.[5] In 1974, Cherrapunji holds a worldwide record with the reported rainfall of 2500 -cm, but recently; it was surpassed by Mawsynram which is located nearby but a few miles away from it.[6,7]
DIARRHEAL DISEASE ENVIRONMENT OF THE STATE
Water quality, purity, and its accessibility affect substantial numbers of the world population,[8] and bacterial water contamination, particularly water -borne diseases, is likely to disturb the whole fabric of society. Diarrhea and dysentery are regarded as the two major wide-spread water -borne diseases. Both are said to be endemic in many regions of Asia and are the leading causes of high degree of morbidity and mortality. Diarrhea is considered to be one of the major health threats to the world populations both in tropical and subtropical poor countries, and is responsible for about 5 million deaths annually, of which 2.5 million falls under the children of less than 5 years.[9] World Health Organization (WHO) defines diarrhea as the “passage of loose or watery stools at least three times in a 24 hour period”, but emphasizes the importance of change in stool consistency rather than frequency, and the usefulness of parental insight in deciding whether children have diarrhea or not.[10] Blood in stool could indicate an acute diarrheal illness or dysentery, irrespective of frequency.[10,11] The major causative agents of diarrhea in human beings include various enteropathogens like Shigella flexneri, Escherichia coli, Staphylococcus aureus, Salmonella typhi, and Candida albicans,[12,13] On the other hand, Shigella spp. are also the most important causes of acute bloody diarrhea (dysentery) and account for about 15% of all deaths attributable to diarrhea in children younger than 5 years.[14] The major thread that can control the causes of various water -borne diseases is the use of advance multiple drug regime such as antibiotics among various enteropathogens. On the other hand, correct case management of acute diarrhea is also now well defined: Oral Rehydration Therapy and continued feeding are sufficient in the majority of episodes and antimicrobial treatment is only warranted in cases of dysentery, parasitic diseases, and severe cholera.[15]
Meghalaya with an estimated population of 2, 357, 510 (density of population is 104 person/ km2) is one among the smallest States in India.[16] The state is divided into seven districts viz. Jaintia Hills, East Khasi Hills, West Khasi Hills, East Garo Hills, West Garo Hills, South Garo Hills, and Ri -Bhoi district. The population is predominantly rural, with 81.41% of the population belongings merely to the scheduled tribes.[17] Though there has been several turn down in death rate, improvement in life expectancy, and increase in health infrastructure, the State's population is still uncovered and lack primary and central health-care services. According to information showed by the Executive Summary Report (1994) of the Directorate of Health Services, Government of Meghalaya, 35.68% covers both the diseases related to natural environment (mainly water -borne) as well as of communicable nature and is more as compared with the overall India rate of 20.80%.[17] Diseases of respiratory tract infections (including pneumonia) and other intestinal infectious diseases (like diarrhea, dysentery, gastroenteritis, etc.) are the two main groups prevailing all over Meghalaya. Among the seven districts of the state, diarrheal diseases ranked first in East Khasi Hill district and second in Ri Bhoi district along with acute respiratory infections. The National Family Health Survey report (1993) showed that one of every twelve children dies before reaching the age of five in the state and in relevant to this, diarrhea is likely to be considered worldwide as the important killer of children under age 5 years. The national average percentage of people suffering from diarrhea with blood (dysentery) is 2.6%. The prevalence in north -eastern states varies from 2.2% in Assam to 6.1% in Meghalaya, and when compared with national average, it is very much high. Meghalaya's prevalence rate of 6.1% is reported to be the highest in the country.[18] Unhealthy and unhygienic environment is the main culprit for the widespread and overflow of diarrhea and dysentery in the community. Even though the state reported the highest rainfall in the world, most of the villages situated in the higher slopes suffer mainly from shortage of drinking water throughout the year. The crisis of water in the state led the people living in households to use unhygienic surface water for drinking which are more prone to diarrheal infections than any other sources of drinking water. The incidence that leads to the overspread of these water borne diseases is directly related to the hot seasonal climate, poor environmental sanitation, and the quality of water available. Infected foods, fomites, flies, and cockroaches often spread infections that carry a variety of diarrheagenic enteropathogens. A temperature of 25 °C or more is the most suitable environment for faster breeding of these insects.[19] Moreover, in addition to all these factors, the variations in altitudes and seasonal rainfall are also the main factors in which diarrhea strikes in several districts of the state.[17] According to Mukherjee the highest proportion of this disease was observed in the Nongstoin block of the West Khasi Hills districts with an average of 39.18%, much higher than that of the state average of 20.57%. The main reason behind such discrepancy is the poor utilization of drinking water.
ETHNOBOTANICAL PLANTS UTILIZED BY THE TRIBALS TO COMBAT DIARRHEAL DISEASE
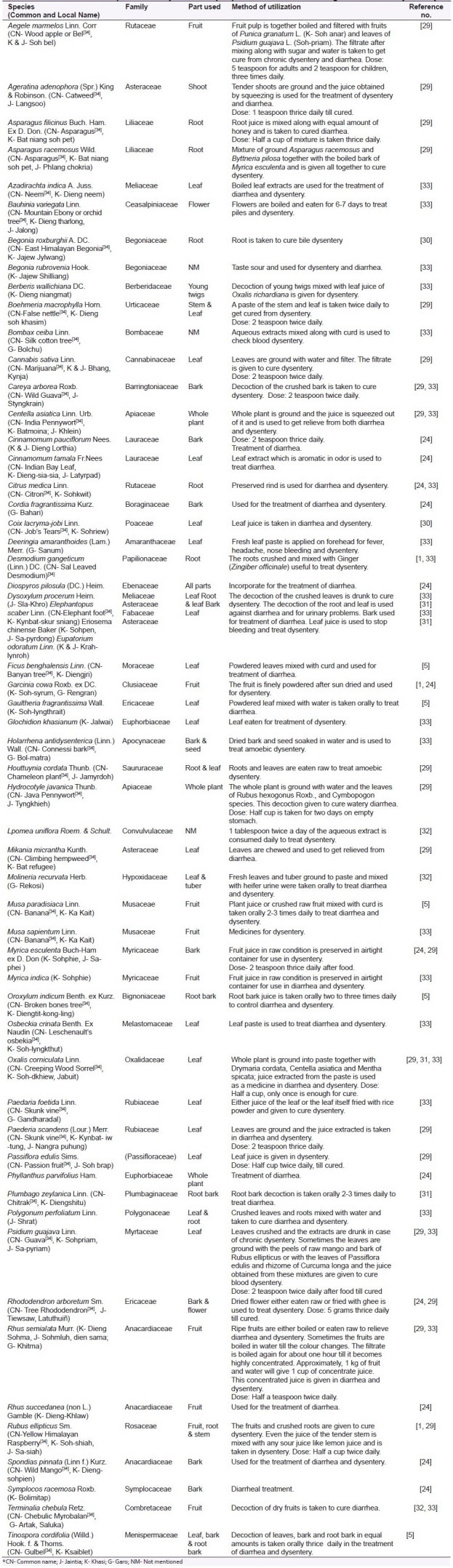
In order to combat the problems of diarrhea globally, the WHO in its Diarrheal Disease Control program has given a special emphasis on the use of traditional folklore medicines in the control and management of diarrhea.[20] Medicinal plants are promising and most suitable source of anti -diarrheal drugs.[21,22] Jaintia, along with the Khasi and Garo tribes of Meghalaya, use the ethnobotanical traditional knowledge of treatment based on herbal drugs to combat various diseases and treat different ailments. Some of the most commonly used medicinal herbs for the treatment of diarrhea and dysentery are enumerated alphabetically in the Table 1.
Table 1.
List of medicinal plants use by the tribal people of the state for curing diarrhea and dysentery
DISCUSSION
Diarrhea is regarded worldwide as one of the killer diseases and unfortunately, it happens to be among the symptoms of many other diseases.[23] The main cause of death from diarrhea is dehydration which results from the loss of electrolytes in diarrheal stools. The inappropriate utilization of sanitation and water for drinking is the main turnover that leads to the outbreak of the disease in the state Meghalaya. Hence, to restore personal comfort and convenience, many patients require antidiarrheal therapy and they were prescribed with several antidiarrheal drugs. In traditional medicine system, many plants or herbs are claimed to have antidiarrheal efficacy without any scientific basis.
The state Meghalaya is rich in plant biodiversity and majority of the population relies mainly on agriculture. The strange climatic and geographical positions as well as the physical features of various districts explain to a large extent the extreme isolation of tribes in different districts. Different tribes have their own way of living and adaptation. Their gradual contact with nature has led to the development of an inquisitive knowledge which ultimately is reflected in their traditional culture, local belief, religion, folklore, taboos, and dialects which are found to be ethno -botanically interesting. About 90% of the rural population in hilly terrain depends on traditional healthcare system.[24] Most of the tribes are farmers and quite a good number of medicine men, and different varieties of medicinal plants prepared in different formulation are sold that can be available during the market day (“Ka Iewduh in Khasi” and “Ka Iawmusiang in Jaintia”) which is held ones in a week in different areas of the state. The medicinal plants sold are mostly edible in nature. In most of the rural areas of the state, people belief that traditional medicines have a good impact in the treatment of various disease ailments and they rely mainly on the medicine men. The medicinal plants on which these medicines men prescribe for the cure of certain disease have an outstanding activity and are given in different formulations but mostly in extracted liquid form. Preparation might be either in extract of single herb or mixtures of one herb with others and may be dose –dependent, as shown with certain examples in Table 1. The mixtures of one or more herbs seem to have a synergistic effect that is more likely to produce a possible cure of the diseases. Most of the well -known plants like Aegele marmelos, Asparagus racemosus, Azadirachta indica, Cannabis sativa, Centella asiatica, Holarrhena antidysenterica, Terminalia chebula, etc. are found to be distributed in different areas of the state and used by the local tribes to treat the complications of diarrheal disorders. Despite the easy availability of medicinal plants in the local market, there are also various numerous medicinal plants that are still scientifically unexplored and unfamiliar. In fact, medicinal plants are also available in many religious forests or sacred groves in different areas of the state. The sacred groves are regarded as the virgin forest where there are various rules and restrictions held by the head of the tribes who are considered to be residences of the local deities. These groves are regarded as the treasure house of plant diversity and harbor a large number of valuable species either plant or wild life. Different groves have different restrictions which prevents the intruders from misuse of the land inside the forest area. Cutting of trees, plugging of twigs, flowers, and fruits, and spitting or urination is strictly prohibited. Various cultural and religious rites and rituals are also performed in these groves and except for medicinal purposes, none of the plant species is harmed in any way.[25,26] A number of the medicinal plant species of antidiarrheal value were found to be distributed inside the two sacred groove forests (Swer and Mairang sacred groves) situated in Meghalaya.[24] Most of these plant species are woody in nature and they are found mostly in the disturbed sacred groves forest of Swer. Species like Cinnamomum tamala, Diospyros pilosula, Phyllanthus parvifolius, Rhododendron arboretum, Spondias pinnata, and Symplocos racemosa are found to be present in the Swer sacred groves and very less species are distributed in the undisturbed Mairang sacred groves. Species like Cinnamomum pauciflorum, Garcinia cowa, Myrica esculenta, and Cordia fragrantissima are found to be well distributed both in the forest of Swer and Mairang sacred groves. In addition to these two sacred groves, there are a lot more that has been reported in the state of which 15 of 79 sacred groves were found only in the Jaintia hills district alone. Plant belonging to some strange families like Magnoliaceae, Himantandraceae, Digneriaceae, Eupomatiaceae, Winteraceae, Trochodendraceae, Lardizabalaceae, Poaceae, Fabaceae, and Orchidaceae are found to be distributed inside these sacred forests.[27,28]
CONCLUSION
Traditional health-care system is an age -old practice performed since ancient time by the people in the state of Meghalaya. It is seen that different plant species were ethnobiologically used by the local people to overcome the complications of diarrhea and dysentery which are the dreadful diseases of the state. The pharmacological screening of the antidiarrheal activity and the isolation of a pure lead compounds from each of the individual plants will give the excellent information in regard with the true remedial activity to cure diarrheal complications.
ACKNOWLEDGEMENT
Authors are thankful to the Botanical Survey of India, Shillong -793 001, Meghalaya, and to Mr. H. Carehome Pakyntein (President -Jaintia Indigenous Medicine Association) for their valuable help and support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Rao RR. Ethnobotany of Meghalaya: Medicinal plants used by Khasi and Garo tribes. Econ Bot. 1981;35:4–9. [Google Scholar]
- 2.Mauri P, Pietta P. Electrospray characterization of selected medicinal plant extracts. J Pharm Biomd Anal. 2000;23:61–8. doi: 10.1016/s0731-7085(00)00264-8. [DOI] [PubMed] [Google Scholar]
- 3.Jain SK, Tarafder CR. Medicinal plant-lore of the santals. Ecin Bot. 1970;24:241–5. [Google Scholar]
- 4.Kayang H. Tribal knowledge on wild edible plants of Meghalaya, Northeast India. Indian J Tradit Knowl. 2007;6:177–81. [Google Scholar]
- 5.Jaiswal V. Cultures and ethnobotany of Jaintia tribal community of Meghalaya, Northeast India- A mini review. Indian J Tradit Knowl. 2010;9:38–44. [Google Scholar]
- 6.Kumar R, Singh RD, Sharma KD. Water resources of India. Curr Sci. 2005;89:794–881. [Google Scholar]
- 7.Dolui AK, Sharma HK, Marein TB, Lalhriatpuii T. Folk herbal remedies of Meghalaya. Indian J Tradit Knowl. 2004;3:358–64. [Google Scholar]
- 8.Bartram J, Lewis K, Lenton R, Wright A. Focusing on improved water and sanitation for health. Lancet. 2005;365:810–2. doi: 10.1016/S0140-6736(05)17991-4. [DOI] [PubMed] [Google Scholar]
- 9.Heinrich M, Heneka B, Ankli A, Rimpler H, Sticher O, Kostiza T. Spasmolytic and antidiarrheal properties of the Yucatec Mayan medicinal plant Casimiroa tetrameria. J Pharm and Pharmacol. 2005;57:1081–5. doi: 10.1211/jpp.57.9.0002. [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization: The treatment of diarrhea: a manual for physicians and other senior health workers, WHO/CDR/95.3. Geneva: World Health Organization; 1995. [Google Scholar]
- 11.Baqui AH, Black RE, Yunus M, Hoque AR, Chowdhury HR, Sack RB. Methodological issues in diarrheal diseases epidemiology:Definition of diarrheal episodes. Int J Epidemiol. 1991;20:1057–63. doi: 10.1093/ije/20.4.1057. [DOI] [PubMed] [Google Scholar]
- 12.Anne JM, Geboes K. Infectious colitis. Acta Endoscopica. 2002;32:2. [Google Scholar]
- 13.Robert K, Egon S, Daniela B, Florian D, Christoph W, Gunter JK, et al. Role of candida in antibiotic-associated diarrhea. J Infect Dis. 2001;184:1065–9. doi: 10.1086/323550. [DOI] [PubMed] [Google Scholar]
- 14.World Health Organization: The management of bloody diarrhea in young children: WHO/CDD/94.49. Geneva: World Health Organization; 1994. [PMC free article] [PubMed] [Google Scholar]
- 15.World Health Organization: A Manual for the treatment of diarrhea for use by physicians and other senior health workers. WH0/CDD/80.2. Geneva: World Health Organization; 1990. [Google Scholar]
- 16.Seth SD, Sharma B. Medicinal plants in India. Ind J Med Res. 2004;120:9–11. [PubMed] [Google Scholar]
- 17.Mukherjee S, editor. Proceedings of the third International Conference on Environment and Health, Chennai, India, 2003 December 15-17. Chennai: Department of Geography, University of Madras and Faculty of Environmental Studies, York University; 2003. Geo-Medical aspects of acute diarrheal diseases in Meghalaya; pp. 276–83. [Google Scholar]
- 18.Medind.nic.in. Diarrhea: Morbidity, mortality and immunization. Meghalaya: 1999. p. 73. Available from: http://medind.nic.in/haa/t04/i1/haat04i1p71.pdf . [Google Scholar]
- 19.Park K. Preventive and Social Medicine. Jabalpur: M/s B. Bhanot Publishers; 1997. pp. 171–4. [Google Scholar]
- 20.Anonymous, Epidemic diarrhoea due to Vibrio cholera. Wkly Epidemic Rec. 1979;16:121. [Google Scholar]
- 21.Maikere-Faniyo R, Van PL, Mutwewingabo A, Habiyaremye FX. Study of Rwandese medicinal plants used in the treatment of diarrhea. J Ethnopharmacol. 1989;26:101–9. doi: 10.1016/0378-8741(89)90057-3. [DOI] [PubMed] [Google Scholar]
- 22.Almeida CE, Karnikowski MG, Foleto R, Baldisserotto B. Analysis of antidiarrhoeic effect of plants used in popular medicine. Revista de Saude Publica. 1995;29:428–33. doi: 10.1590/s0034-89101995000600002. [DOI] [PubMed] [Google Scholar]
- 23.Farthing MJ. Diarrhea: A significant worldwide problem. Int J Antimicrob Agents. 2000;14:65–9. doi: 10.1016/s0924-8579(99)00149-1. [DOI] [PubMed] [Google Scholar]
- 24.Laloo RC, Kharlukhi S, Jeeva S, Mishra BP. Status of medicinal plants in the disturbed and the undisturbed sacred forest of Meghalaya, Northeast India: Population structure and regeneration efficacy of some important species. Curr Sci. 2006;90:225–32. [Google Scholar]
- 25.Jeeva S, Mishra BP, Venugopal N, Kharlukhi L, Laloo RC. Traditional knowledge and biodiversity conservation in the sacred groves of Meghalaya. Indian J Tradit Knowl. 2006;5:563–8. [Google Scholar]
- 26.Jeeva S, Mishra BP, Venugopal N, Laloo RC. Sacred forests: Traditional ecological heritage in Meghalaya. J Scott Res Forum. 2006;1:93–7. [Google Scholar]
- 27.Kumar Y. Floristic studies on Balphakram wild life sanctuary in Meghalaya-5, rare endemic and threatened flora. J Megh Sci Soc. 1991;11:33–48. [Google Scholar]
- 28.Jamir SA, Pandey HN. Vascular plant diversity in the sacred groves of Jaintia hills in Northeast India. Biodiv Conserv. 2003;12:1497–510. [Google Scholar]
- 29.Ahmed AA, Borthakur SK. In: Ethnobotanical Wisdom of the Khasis (Hynniew Treps) of Meghalaya. Singh Bishen, Pal Singh Mahendra., editors. DehraDun- 01: India: 2005. pp. 114–47. [Google Scholar]
- 30.Hynniewta SR, Yogendra K. Herbal remedies among the Khasi traditional healers and village folks in Meghalaya. Indian J Tradit Knowl. 2008;7:581–6. [Google Scholar]
- 31.Neogi B, Prasad MN, Rao RR. Ethnobotany of some weeds of Khasi and Garo Hills, Meghalaya, Northeastern India. Econ Bot. 1989;43:471–9. [Google Scholar]
- 32.Maikhuri RK, Gangwar AK. Ethnobiological notes on the Khasi and Garo tribes of Meghalaya, Northeast India. Econ Bot. 1993;47:345–57. [Google Scholar]
- 33.Frlht.org.in. Medicinal plants conservation and sustainable utilization- Meghalaya, India. Annexure- C. Meghalaya. 2003. pp. 55–75. Available from: http://www.frlht.org.in/html/reports/meghalayaslpc.pdf .
- 34.Flowersofindia.net. Flowers by botanical name. Available from: http://www.flowersofindia.net/botanical.html .